LESSON 3
THEMES :
1. DERMATOPHYTOSIS: TRICHOPHYTOSIS (INFILTRATIVE PURULENT, SUPERFICIAL). MICROSPORIA.
RUBROPHYTOSIS (TYPES ACCORDING LOCATION). TINEA UNGUINUM (ONYCHOMYCOSIS). TINEA PEDIS, TYPES. TINEA CRURIS.
2. CUTANEOUS AND NAIL CANDIDIASIS: CUTANEOUS CANDIDIASIS, CANDIDAL PARONYCHIA, CANDIDAL ONYCHOMYCOSIS, ANGULUR CHEILITIS, CANDIDAL CHEILITIS, AND DENTURE STOMATITIS. CANDIDAL VULVOVAGINITIS, CANDIDAL BALANOPOSTHITIS. LABORATORY DIAGNOSTIC. PITURIASIS VERSICOLOR.

TINEA CORPORIS
http://emedicine.medscape.com/article/1091473-overview
http://www.youtube.com/watch?v=tfpPwiXH8vk
Tinea corporis is a superficial dermatophyte infection characterized by either inflammatory or noninflammatory lesions on the glabrous skin (ie, skin regions except the scalp, groin, palms, and soles). Three anamorphic (asexual or imperfect) genera cause dermatophytoses: Trichophyton, Microsporum, and Epidermophyton. Dermatophytes may infect humans (anthropophilic), infect nonhuman mammals (zoophilic), or reside primarily in the soil (geophilic).
Pathophysiology
Dermatophytes preferentially inhabit the nonliving, cornified layers of the skin, hair, and nail, which is attractive for its warm, moist environment conducive to fungal proliferation. Fungi may release keratinases and other enzymes to invade deeper into the stratum corneum, although typically the depth of infection is limited to the epidermis and, at times, its appendages. They generally do not invade deeply, owing to nonspecific host defense mechanisms that can include the activation of serum inhibitory factor, complement, and polymorphonuclear leukocytes.
Following the incubation period of 1-3 weeks, dermatophytes invade peripherally in a centrifugal pattern. In response to the infection, the active border has an increased epidermal cell proliferation with resultant scaling. This creates a partial defense by way of shedding the infected skin and leaving new, healthy skin central to the advancing lesion. Elimination of dermatophytes is achieved by cell-mediated immunity.
Trichophyton rubrum is a common dermatophyte and, because of its cell wall, is resistant to eradication. This protective barrier contains mannan, which may inhibit cell-mediated immunity, hinder the proliferation of keratinocytes, and enhance the organism’s resistance to the skin’s natural defenses.
History
Symptoms, contact history, recent travel, and international residence are relevant clues in the history of a person with tinea corporis.
· Infected patients may have variable symptoms.
o Patients can be asymptomatic.
o A pruritic, annular plaque is characteristic of a symptomatic infection. Patients occasionally can experience a burning sensation.
o HIV-positive or immunocompromised patients may develop severe pruritus or pain.
· Tinea corporis may result from contact with infected humans, animals, or inanimate objects. The history may include occupational (eg, farm worker, zookeeper, laboratory worker, veterinarian), environmental (eg, gardening, contact with animals), or recreational (eg, contact sports, contact with sports facilities) exposure.
· A few clinical variants are described, with distinct presentations.
o Majocchi granuloma, typically caused by T rubrum, is a fungal infection in hair, hair follicles, and, often, the surrounding dermis, with an associated granulomatous reaction. Majocchi granuloma often occurs in females who shave their legs.
o Tinea corporis gladiatorum is a dermatophyte infection spread by skin-to-skin contact between wrestlers.
o Tinea imbricata is a form of tinea corporis found mainly in Southeast Asia, the South Pacific, Central America, and South America. It is caused by Trichophyton concentricum.
o Tinea incognito is tinea corporis with an altered, nonclassic presentation due to corticosteroid treatment.
Physical
Tinea corporis can manifest in a variety of ways.
Typically, the lesion begins as an erythematous, scaly plaque that may rapidly worsen and enlarge, as shown in the image below.
Large, erythematous, scaly plaque.
Following central resolution, the lesion may become annular in shape, as is shown in the image below.
Annular plaque.
As a result of the inflammation, scale, crust, papules, vesicles, and even bullae can develop, especially in the advancing border.
Rarely, tinea corporis can present as purpuric macules, called tinea corporis purpurica.One report describes 2 cases of tinea corporis purpurica resulting from self-inoculation with Trichophyton violaceum.
Infections due to zoophilic or geophilic dermatophytes may produce a more intense inflammatory response than those caused by anthropophilic microbes.
HIV-infected or immunocompromised patients often have atypical presentations including deep abscesses or a disseminated skin infection.
Majocchi granuloma manifests as perifollicular, granulomatous nodules typically in a distinct location, which is the lower two thirds of the leg in females.
Tinea corporis gladiatorum often manifests on the head, neck, and arms, which is a distribution consistent with the areas of skin-to-skin contact in wrestling.
Tinea imbricata is recognized clinically by its distinct scaly plaques arranged in concentric rings.
Causes
Tinea corporis can be caused by a variety of dermatophytes, although prevalence and patient history are very helpful in identifying the most likely organism.
Internationally, the most common cause is T rubrum.
T tonsurans, Trichophyton mentagrophytes, Trichophyton interdigitale, Trichophyton verrucosum,Microsporum canis, and Microsporum gypseum are also known to produce infection.
Tinea imbricata is caused by Trichophyton concentricum.
Dermatophytoses may be acquired from different sources, such as people, animals, or soil.
Infected humans are the most common source of tinea corporis in the United States.
Contact with contaminated household pets, farm animals, and fomites (eg hair brushes, towels) can spread infection.
T verrucosum causes 98% of dermatophyte infections in cattle and is showing increasing prevalence of infection in human contacts.
T mentagrophytes is spread by rabbits, guinea pigs, and small rodents.
Infection with M gypseum, a geophilic organism, can mimic tinea imbricata in presentation.
Because fungal arthroconidia can survive in the environment, recurrent outbreaks may occur.
Differential Diagnoses
![]() Lupus Erythematosus, Subacute Cutaneous
Lupus Erythematosus, Subacute Cutaneous
![]() Lymphocytic Skin Infiltration
Lymphocytic Skin Infiltration
![]() Psoriasis, Annular
Psoriasis, Annular
Laboratory Studies
A potassium hydroxide (KOH) examination of skin scrapings may be diagnostic in tinea corporis.
A KOH test is a microscopic preparation used to visualize fungal elements removed from the skin’s stratum corneum.
The sample should be taken from the active border of a lesion because this region provides the highest yield of fungal elements. A KOH preparation from a vesicular lesion should be made from the roof of the vesicle.
The KOH helps dissolve the keratin and leaves fungal elements intact, revealing numerous septate, branching hyphae amongst epithelial cells.
A counterstain, such as chlorazol black E or Parker blue-black ink, may help visualize hyphae under the microscope.
A fungal culture is often used as an adjunct to KOH for diagnosis. Fungal culture is more specific than KOH for detecting a dermatophyte infection; therefore, if the clinical suspicion is high yet the KOH result is negative, a fungal culture should be obtained.
A few culture mediums are available for dermatophyte growth.
Sabouraud agar containing neopeptone or polypeptone agar and glucose is often used for fungal culture. However, it does not contain antibiotics and may allow overgrowth of fungal and bacterial contaminants.
Mycosel, a commonly used agar, is similar to Sabouraud agar but has antibiotics.
Commonly, dermatophyte test medium (DTM) is used. It contains antibacterial (ie, gentamicin, chlortetracycline) and antifungal (ie, cycloheximide) solutions in a nutrient agar base. This combination isolates dermatophytes while suppressing other fungal and bacterial species that may contaminate the culture.
Following culture inoculation, potential fungal growth is monitored for 2 weeks.
Positive culture results vary depending on the medium used.
DTM contains phenol red solution, which causes a color change from straw-yellow to bright-red under alkaline conditions, indicating a positive dermatophyte culture result. However, the color makes identification of culture morphology (particularly pigmentation) difficult.
Sabouraud or Mycosel agar should be used to assess gross and microscopic colony characteristics.
If the above clinical evaluations are inconclusive, the molecular method of polymerase chain reaction for fungal DNA identification can be applied.
For atypical presentations of tinea corporis, further evaluation for HIV infection and/or an immunocompromised state should be considered.
Medical Care
Topical therapy is recommended for a localized infection because dermatophytes rarely invade living tissues. Topical therapy should be applied to the lesion and at least 2 cm beyond this area once or twice a day for at least 2 weeks, depending on which agent is used.Topical azoles and allylamines show high rates of clinical efficacy. These agents inhibit the synthesis of ergosterol, a major fungal cell membrane sterol.
The topical azoles (eg, econazole, ketoconazole, clotrimazole, miconazole, oxiconazole, sulconazole, sertaconazole) inhibit the enzyme lanosterol 14-alpha-demethylase, a cytochrome P-450–dependent enzyme that converts lanosterol to ergosterol. Inhibition of this enzyme results in unstable fungal cell membranes and causes membrane leakage. The weakened dermatophyte is unable to reproduce and is slowly killed by fungistatic action. Sertaconazole nitrate is one of the newest topical azoles. It has fungicidal and anti-inflammatory abilities and is used as a broad-spectrum agent. It may have a reservoir effect and therefore is a good choice for noncompliant patients. Lastly, Liebel et al published in vitro data in 2006, reporting this drug has anti-itch properties.
Allylamines (eg, naftifine, terbinafine) and the related benzylamine butenafine inhibit squalene epoxidase, which converts squalene to ergosterol. Inhibition of this enzyme causes squalene, a substance toxic to fungal cells, to accumulate intracellularly and leads to rapid cell death. Allylamines bind effectively to the stratum corneum because of their lipophilic nature. They also penetrate deeply into hair follicles.
Ciclopirox olamine is a topical fungicidal agent. It causes membrane instability by accumulating inside fungal cells and interfering with amino acid transport across the fungal cell membrane.
A low-to-medium potency topical corticosteroid can be added to the topical antifungal regimen to relieve symptoms. The steroid can provide rapid relief from the inflammatory component of the infection, but the steroid should only be applied for the first few days of treatment. Prolonged use of steroids can lead to persistent and recurrent infections, longer duration of treatment regimens, and adverse effects of skin atrophy, striae, and telangiectasias.
Systemic therapy may be indicated for tinea corporis that includes extensive skin infection, immunosuppression, resistance to topical antifungal therapy, and comorbidities of tinea capitis or tinea unguium. Use of oral agents requires attention to potential drug interactions and monitoring for adverse effects.
The mechanism of action or oral micronized griseofulvin against dermatophytes is disruption of the microtubule mitotic spindle formation in metaphase, causing arrest of fungal cell mitosis. A dose of 10 mg/kg/d for 4 weeks is effective. In addition, griseofulvin induces the cytochrome P-450 enzyme system and can increase the metabolism of CYP-450–dependent drugs. It is the systemic drug of choice for tinea corporis infections in children.
Systemic azoles (eg, fluconazole, itraconazole, ketoconazole) function similar to the topical agents, causing cell membrane destruction.
Oral ketoconazole at 3-4 mg/kg/d may be given. However, this agent carries an associated risk of hepatitis in less than 1 in 10,000 cases and now is seldom used orally for dermatophyte infections.
Fluconazole at 50-100 mg/d or 150 mg once weekly for 2-4 weeks is used with good results.
Oral itraconazole in doses of 100 mg/d for 2 weeks shows high efficacy. With an increased dose of 200 mg/d, the treatment duration can be reduced to 1 week. However, the cytochrome P-450 activity of itraconazole allows for potential interactions with other commonly prescribed drugs.
Based on E-test for susceptibility of T rubrum, voriconazole was the most active and fluconazole was the least active of the azole drugs.
Oral terbinafine may be used at a dosage of 250 mg/d for 2 weeks; the potential exists for cytochrome P-450, specifically CYP-2D6, drug interactions with this agent.
Medication Summary
The goals of pharmacotherapy are to reduce morbidity and to prevent complications. Topical antifungal agents are effective for treating most cases of tinea corporis. Systemic therapy may be indicated for tinea corporis that is extensive, involves immunocompromised patients, or is refractory to topical therapy. For severe infections, systemic therapy can be combined with topical antifungal treatments.
Oral granules of terbinafine (Lamisil) are available in packets containing 125 mg and 187.5 mg and are for use in children with tinea capitis who are aged 4 years and older; these granules can be sprinkled once daily on pudding or mashed potatoes. While approved only for tinea capitis, these oral granules likely are used off label in children with tinea corporis when systemic therapy is needed. The suggested dosing schedule for tinea capitis is 125 mg/d for less than 25 kg body weight, 187.5 mg/d for 25-35 kg body weight, and 250 mg/d for greater than 35 kg body weight.
Topical allylamines
Naftifine 1% cream or gel (Naftin)
Terbinafine topical (Lamisil)
Topical pyridones
Ciclopirox olamine 1% cream (Loprox)
Topical benzylamines
Butenafine 1% cream (Mentax)
Systemic azoles
Fluconazole (Diflucan)
Itraconazole (Sporanox)
Ketoconazole (Nizoral)
Systemic allylamines
Terbinafine (Lamisil, Daskil)
Other systemic antifungals
Griseofulvin (Fulvicin)
Topical azoles
Clotrimazole 1% cream (Mycelex, Lotrimin)
Ketoconazole topical (Nizoral)
Miconazole topical (Monistat)
Oxiconazole 1% cream (Oxistat)
Sertaconazole 2% cream (Ertaczo)
Sulconazole 1% cream or solution (Exelderm)
References:
1. Seyfarth F, Goetze S, Erhard M, Burmester A, Elsner P, Hipler UC. [Infection with a rare geophilic dermatophyte.]. Hautarzt. Aug 14 2009;[Medline].
2. Yehia MA, El-Ammawi TS, Al-Mazidi KM, Abu El-Ela MA, Al-Ajmi HS. The Spectrum of Fungal Infections with a Special Reference to Dermatophytoses in the Capital Area of Kuwait During 2000-2005: A Retrospective Analysis. Mycopathologia. Nov 17 2009;[Medline].
3. Ilkit M, Saracli M, Kurdak H, et al. Clonal outbreak of Trichophyton tonsurans tinea capitis gladiatorum among wrestlers in Adana, Turkey. Med Mycol. Oct 14 2009;[Medline].
4. Romano C, Massai L, Strangi R, Feci L, Miracco C, Fimiani M. Tinea corporis purpurica and onychomycosis caused by Trichophyton violaceum. Mycoses. Sep 22 2009;[Medline].
5. Mapelli ET, Borghi E, Cerri A, Sciota R, Morace G, Menni S. Tinea corporis due to Trichophyton rubrum in a Woman and Tinea capitis in her 15-Day-Old Baby: Molecular Evidence of Vertical Transmission. Mycopathologia. Oct 14 2011;[Medline].
6. Carod JF, Ratsitorahina M, Raherimandimby H, Hincky Vitrat V, Ravaolimalala Andrianaja V, Contet-Audonneau N. Outbreak of Tinea capitis and corporis in a primary school in Antananarivo, Madagascar. J Infect Dev Ctries. Oct 13 2011;5(10):732-6. [Medline].
7. Hryncewicz-Gwózdz A, Beck-Jendroschek V, Brasch J, Kalinowska K, Jagielski T. Tinea capitis and tinea corporis with a severe inflammatory response due to Trichophyton tonsurans. Acta Derm Venereol. Oct 2011;91(6):708-10. [Medline].
TINEA CAPITIS
1. http://emedicine.medscape.com/article/1091351-overview
2. http://www.youtube.com/watch?v=dNU0Cht2fiw
Background
Tinea capitis is a disease caused by superficial fungal infection of the skin of the scalp, eyebrows, and eyelashes, with a propensity for attacking hair shafts and follicles (see the image below). The disease is considered to be a form of superficial mycosis or dermatophytosis. Several synonyms are used, including ringworm of the scalp and tinea tonsurans. In the United States and other regions of the world, the incidence of tinea capitis is increasing.
Gray-patch ringworm (microsporosis) is an ectothrix infection or prepubertal tinea capitis seen here in an African American male child. Gray patch refers to the scaling with lack of inflammation, as noted in this patient. Hairs in the involved areas assume a characteristic dull, grayish, discolored appearance. Infected hairs are broken and shorter. Papular lesions around hair shafts spread and form typical patches of ring forms, as shown. Culture from the lesional hair grew Microsporum canis.
Dermatophytosis includes several distinct clinical entities, depending on the anatomic site and etiologic agents involved. Clinically, the conditions include tinea capitis, tinea favosa (favus resulting from infection by Trichophyton schoenleinii), tinea corporis (ringworm of glabrous skin), tinea imbricata (ringworm resulting from infection by Trichophyton concentricum), tinea cruris (ringworm of the groin), tinea unguium or onychomycosis (ringworm of the nail), tinea pedis (ringworm of the feet), tinea barbae (ringworm of the beard), and tinea manuum (ringworm of the hand).
Clinical presentation of tinea capitis varies from a scaly noninflamed dermatosis resembling seborrheic dermatitis to an inflammatory disease with scaly erythematous lesions and hair loss or alopecia that may progress to severely inflame deep abscesses termed kerion, with the potential for scarring and permanent alopecia. The type of disease elicited depends on interaction between the host and the etiologic agents.
The term tinea originally indicated larvae of insects that fed on clothes and books. Subsequently, it meant parasitic infestation of the skin. By the mid 16th century, the term was used to describe diseases of the hairy scalp. The term ringworm referred to skin diseases that assumed a ring form, including tinea. The causative agents of tinea infections of the beard and scalp were described first by Remak and Schönlein, then by Gruby, during the 1830s. Approximately 50 years later, in Sabouraud’s dissertation, the endothrix type of tinea capitis infection was demonstrated, and it was known that multiple species of fungi cause the disease. Simple culture methods were described and treatment using x-ray epilation was reported in 1904. Effective treatment of tinea capitis by griseofulvin became available in the 1950s.
Pathophysiology
Tinea capitis is caused by fungi of species of genera Trichophyton and Microsporum. Tinea capitis is the most common pediatric dermatophyte infection worldwide. The age predilection is believed to result from the presence of Pityrosporum orbiculare (Pityrosporum ovale), which is part of normal flora, and from the fungistatic properties of fatty acids of short and medium chains in postpubertal sebum.
Causative agents of tinea capitis include keratinophilic fungi termed dermatophytes. These molds usually are present ionliving cornified layers of skin and its appendages and sometimes are capable of invading the outermost layer of skin, stratum corneum, or other keratinized skin appendages derived from epidermis, such as hair and nails.
Dermatophytes are among the most common infectious agents of humans, causing a variety of clinical conditions that are collectively termed dermatophytosis. From the site of inoculation, the fungal hyphae grow centrifugally in the stratum corneum. The fungus continues downward growth into the hair, invading keratin as it is formed. The zone of involvement extends upwards at the rate at which hair grows, and it is visible above the skin surface by days 12-14. Infected hairs are brittle, and by the third week, broken hairs are evident.
Three types of in vivo hair invasion are recognized.
· Ectothrix invasion is characterized by the development of arthroconidia on the exterior of the hair shaft. The cuticle of the hair is destroyed, and infected hairs usually fluoresce a bright greenish-yellow color under a Wood lamp ultraviolet light. Common agents include Microsporum canis, Microsporum gypseum, Trichophyton equinum, and Trichophyton verrucosum.
· Endothrix hair invasion is characterized by the development of arthroconidia within the hair shaft only. The cuticle of the hair remains intact and infected hairs do not fluoresce under a Wood lamp ultraviolet light. All endothrix-producing agents are anthropophilic (eg, Trichophyton tonsurans, Trichophyton violaceum).
· Favus, usually caused by T schoenleinii, produces favuslike crusts or scutula and corresponding hair loss.
Tinea Capitis Clinical Presentation
History
![]() Tinea capitis begins as a small erythematous papule around a hair shaft on the scalp, eyebrows, or eyelashes.
Tinea capitis begins as a small erythematous papule around a hair shaft on the scalp, eyebrows, or eyelashes.
![]() Within a few days, the red papule becomes paler and scaly, and the hairs appear discolored, lusterless, and brittle. They break off a few millimeters above the scalp skin surface.
Within a few days, the red papule becomes paler and scaly, and the hairs appear discolored, lusterless, and brittle. They break off a few millimeters above the scalp skin surface.
![]() The lesion spreads, forming numerous papules in a typical ring form. Ring-shaped lesions may coalesce with other infected areas.
The lesion spreads, forming numerous papules in a typical ring form. Ring-shaped lesions may coalesce with other infected areas.
![]() Pruritus usually is minimal but may be intense at times.
Pruritus usually is minimal but may be intense at times.
![]() Alopecia is common in infected areas.
Alopecia is common in infected areas.
![]() Inflammation may be mild or severe. Deep boggy red areas characterized by a severe acute inflammatory infiltrate with pustule formation are termed kerions or kerion celsi (see the image below).
Inflammation may be mild or severe. Deep boggy red areas characterized by a severe acute inflammatory infiltrate with pustule formation are termed kerions or kerion celsi (see the image below).
Typical lesions of kerion celsi on the vertex scalp of a young Chinese boy.
Favus (also termed tinea favosa) is a severe form of tinea capitis.
Favus is a chronic infection caused most commonly by T schoenleinii and, occasionally, by T violaceum or Microsporum gypsum.
Scalp lesions are characterized by the presence of yellow cup-shaped crusts termed scutula, which surround the infected hair follicles.
Favus is seen predominantly in Africa, the Mediterranean, and the Middle East and, rarely, in North America and South America, usually in descendants of immigrants from endemic areas.
Favus usually is acquired early in life and has a tendency to cluster in families.
In favus, infected hairs appear yellow.
Physical
A variety of clinical presentations of tinea capitis are recognized as being inflammatory or noninflammatory and are usually associated with patchy alopecia. However, the infection may be widespread, and the clinical appearances can be subtle. In urban areas, tinea capitis should be considered in the differential diagnosis of children older than 3 months with a scaly scalp until proveegative by mycological examination. Infection may also be associated with painful regional lymphadenopathy, especially in the inflammatory variants.
Pertinent physical findings are limited to the skin of scalp, eyebrows, and eyelashes.
Primary skin lesions of tinea capitis
Lesions begin as red papules with progression to grayish ring-formed patches containing perifollicular papules.
Pustules with inflamed crusts, exudate, matted infected hairs, and debris may be seen.
Black dot tinea capitis refers to an infection with fracture of the hair, leaving the infected dark stubs visible in the follicular orifices.
Kerion celsi may progress to a patchy or diffuse distribution and to severe hair loss with scarring alopecia (see the image below).
Discrete patches of hair loss or alopecia caused by Trichophyton violaceum infection of the vertex scalp of a young Taiwanese boy. Courtesy of Skin Diseases in Chinese by Yau-Chin Lu, MD. Permission granted by Medicine Today Publishing Co, Taipei, Taiwan, 1981.
Id reaction: Dermatophyte idiosyncratic or id reactions are manifestations of the immune response to dermatophytosis.
Id reactions occur at a distant site, and the lesions are devoid of organisms.
Id reactions may be triggered by antifungal treatment.
The most common type of id reaction is an acute vesicular dermatitis of the hands and feet. The grouped vesicles are tense, pruritic, and sometimes painful. Id reactions are noted in patients with inflammatory ringworm of the feet, primarily resulting from infection by Trichophyton mentagrophytes. Similar lesions may occur on the trunk in tinea capitis.
Vesicular lesions may evolve into a scaly eczematoid reaction or a follicular papulovesicular eruption.
Other less common types of id reactions include annular erythema and erythema nodosum. These patients have a strong delayed-type hypersensitivity reaction to intradermal trichophytin.
Distribution of tinea capitis lesions: Skin lesions appear on the scalp with extension to the eyebrows and/or eyelashes.
Regional lymph nodes: Cervical lymphadenopathy may develop in patients with severe inflammation associated with kerion formation..
Differential Diagnoses
![]() Id Reaction (Autoeczematization)
Id Reaction (Autoeczematization)
![]() Lupus Erythematosus, Subacute Cutaneous
Lupus Erythematosus, Subacute Cutaneous
Laboratory Studies
Laboratory diagnosis of tinea capitis depends on examination and culture of skin rubbings, skin scrapings, or hair pluckings (epilated hair) from lesions.
Before specimen collection, any ointment or other local applications present should be removed with alcohol.
Infected hairs appearing as broken stubs are best for examination. They can be removed with forceps without undue trauma or collected by gentle rubbing with a moist gauze pad; broken, infected hairs adhere to the gauze. A toothbrush may be used in a similar fashion.Alternatively, affected areas can be scraped with the end of a glass slide or with a blunt scalpel to harvest affected hairs, broken-off hair stubs, and scalp scale. This is preferable to plucking, which may remove uninvolved hairs. Scrapings may be transported in a folded square of paper. Skin specimens may be scraped directly onto special black cards, which make it easier to see how much material has been collected and provide ideal conditions for transportation to the laboratory; however, affected hairs are easier to see on white paper than on black paper.
Definitive diagnosis depends on an adequate amount of clinical material submitted for examination by direct microscopy and culture. The turn-around time for culture may take several weeks.
Selected hair samples are cultured or allowed to soften in 10-20% potassium hydroxide (KOH) before examination under the microscope. Examination of KOH preparations (KOH mount) usually determines the proper diagnosis if a tinea infection exists.
Conventional sampling of a kerion can be difficult. Negative results are not uncommon in these cases. The diagnosis and decision to treat lesions of kerion may need to be made clinically. A moistened standard bacteriological swab taken from the pustular areas and inoculated onto the culture plate may yield a positive result.
Microscopic examination of the infected hairs may provide immediate confirmation of the diagnosis of ringworm and establishes whether the fungus is small-spore or large-spore ectothrix or endothrix.
Culture provides precise identification of the species for epidemiologic purposes.Primary isolation is carried out at room temperature, usually on Sabouraud agar containing antibiotics (penicillin/streptomycin or chloramphenicol) and cycloheximide (Acti-Dione), which is an antifungal agent that suppresses the growth of environmental contaminant fungi. In cases of tender kerion, the agar plate can be inoculated directly by pressing it gently against the lesion. Most dermatophytes can be identified within 2 weeks, although T verrucosum grows best at 37°C and may have formed only into small and granular colonies at this stage. Identification depends on gross colony and microscopic morphology. Specimens should be inoculated on to primary isolation media, such as Sabouraud dextrose, and incubated at 26-28°C for 4 weeks. The growth of any dermatophyte is significant.
In some cases, other tests involving nutritional requirements and hair penetration in vitro are necessary to confirm the identification.
Wood lamp examination: In 1925, Margarot and Deveze observed that infected hairs and some fungus cultures fluoresce in ultraviolet light. The black light commonly is termed Wood lamp. Light is filtered through a Wood nickel oxide glass (barium silicate with nickel oxide), which allows only the long ultraviolet rays to pass (peak at 365 nm). Wood lamp examination is useful for certain ectothrix infections (eg, those caused by M canis,M audouinii,Microsporum rivalieri). In cases with endothrix infection, however, negative Wood lamp examination findings are of no practical value for screening or monitoring infections.
Hairs infected by M canis, M audouinii, M rivalieri, and M ferrugineum fluoresce a bright green to yellow-green color (see the image below).
Wood lamp examination of a gray-patch area on the scalp. In Microsporum canis infection, scalp hairs emit a diagnostic brilliant green fluorescence. Trichophyton tonsurans does not fluoresce with Wood lamp.
Hairs infected by T schoenleinii may show a dull green or blue-white color, and hyphae regress leaving spaces within the hair shaft.
T verrucosum exhibits a green fluorescence in cow hairs, but infected human hairs do not fluoresce.
The fluorescent substance appears to be produced by the fungus only in actively growing infected hairs.
Infected hairs remain fluorescent for many years after the arthroconidia have died.
When a diagnosis of ringworm is under consideration, the scalp is examined under a Wood lamp. If fluorescent infected hairs are present, hairs are removed for light microscopic examination and culture. Infections caused by Microsporum species fluoresce a typical green color.
Unfortunately, most tinea capitis infections in North America are caused by T tonsurans and do not demonstrate fluorescence.
In favus, infected hairs appear yellow (see the image below).
Wood lamp examination of a gray-patch area on the scalp. In Microsporum canis infection, scalp hairs emit a diagnostic brilliant green fluorescence. Trichophyton tonsurans does not fluoresce with Wood lamp.
Serology is not required for a diagnosis of dermatophytosis.
Videodermatoscopy: A small study in patients with tinea capitis from M canis found that comma hairs were a prominent and distinctive feature on videodermatoscopy; comma hairs were not seen in patients with alopecia areata.
Medical Care
Choice of treatment for tinea capitis is determined by the species of fungus concerned, the degree of inflammation, and in some cases, by the immunologic and nutritional status of the patient.
Systemic administration of griseofulvin provided the first effective oral therapy for tinea capitis.
Topical treatment alone usually is ineffective and is not recommended for the management of tinea capitis.
Newer antifungal medications, such as ketoconazole, itraconazole, terbinafine, and fluconazole, have been reported as effective alternative therapeutic agents for tinea capitis. Of these agents, itraconazole and terbinafine are used most commonly.
Selenium sulfide shampoo may reduce the risk of spreading the infection early in the course of therapy by reducing the number of viable spores that are shed.
Medication Summary
Antifungal agents
Griseofulvin (Fulvicin)
Itraconazole (Sporanox)
Ketoconazole (Nizoral)
Further Outpatient Care
Household contacts of tinea capitis patients should be screened for clinically silent fungal carriage on the scalp. Asymptomatic carriers, including adults and siblings in the family of patients with tinea capitis and patient caretakers and playmates, require active treatment, since they may act as a continuing source of infection.
Shampoo and oral antimycotic therapy have been advocated for eradication of the carrier state.
Studies have shown that most children who received griseofulvin plus biweekly shampooing with 2.5% selenium sulfide were negative for fungi on scalp culture after 2 weeks.
Shampoo containing povidone-iodine has been shown to be more effective in producing negative cultures than shampoos containing econazole and selenium sulfide and than Johnson’s Baby Shampoo. Therapeutic shampoos are applied twice weekly for 15 minutes for 4 consecutive weeks. Both povidone-iodine and selenium shampoos require further clinical study for the control of fungal spore loads in infected children and asymptomatic carriers.
Classrooms with young children (ie, kindergarten through second grade) must be evaluated for tinea capitis infection, since these children are most susceptible and have a greater risk of disease transmission.
Playmates in close physical contact with patients can spread tinea capitis organisms by sharing toys or personal objects including combs and hairbrushes. These individuals need to be evaluated for the presence of infection.
References:
1. Seebacher C, Bouchara JP, Mignon B. Updates on the epidemiology of dermatophyte infections. Mycopathologia. Nov-Dec 2008;166(5-6):335-52. [Medline].
2. Slowinska M, Rudnicka L, Schwartz RA, et al. Comma hairs: a dermatoscopic marker for tinea capitis: a rapid diagnostic method. J Am Acad Dermatol. Nov 2008;59(5 Suppl):S77-9. [Medline].
3. Gupta AK, Cooper EA, Bowen JE. Meta-analysis: griseofulvin efficacy in the treatment of tinea capitis. J Drugs Dermatol. Apr 2008;7(4):369-72. [Medline].
4. Ghannoum MA, Wraith LA, Cai B, Nyirady J, Isham N. Susceptibility of dermatophyte isolates obtained from a large worldwide terbinafine tinea capitis clinical trial. Br J Dermatol. Sep 2008;159(3):711-3. [Medline].
5. [Best Evidence] Elewski BE, Caceres HW, DeLeon L, et al. Terbinafine hydrochloride oral granules versus oral griseofulvin suspension in children with tinea capitis: results of two randomized, investigator-blinded, multicenter, international, controlled trials. J Am Acad Dermatol. Jul 2008;59(1):41-54. [Medline].
6. Tey HL, Tan AS, Chan YC. Meta-analysis of randomized, controlled trials comparing griseofulvin and terbinafine in the treatment of tinea capitis. J Am Acad Dermatol. Apr 2011;64(4):663-70. [Medline].
ONYCHOMYCOSIS,TINEA UNGUIUM
1. http://mulicia.pixnet.net/blog/post/26749579-%E7%94%B2%E7%99%AC-onychomycosis%EF%BC%8Ctinea-unguium
2. http://www.metacafe.com/watch/yt-asp9r5WjBnc/how_to_treat_toe_nail_fungus_iodine/
Distal lateral subungual onychomycosis
Lateral fungal nail involvement in onychomycosis
Superficial white onychomycosis
Proximal subungual white onychomycosis
TINEA PEDIS
http://emedicine.medscape.com/article/1091684-overview
http://www.youtube.com/watch?v=CWvF23hnOAs
Background
Tinea pedis has afflicted humanity for centuries, so it is perhaps surprising that the condition was not described until Pellizzari did so in 1888. The first report of tinea pedis was in 1908 by Whitfield, who, with Sabouraud, believed that tinea pedis was a very rare infection caused by the same organisms that produce tinea capitis.
Tinea pedis is the term used for a dermatophyte infection of the soles of the feet and the interdigital spaces. Tinea pedis is most commonly caused by Trichophyton rubrum, a dermatophyte initially endemic only to a small region of Southeast Asia and in parts of Africa and Australia. Interestingly, tinea pedis was not noted in these areas then, possibly because these populations did not wear occlusive footwear. The colonization of the T rubrum –endemic regions by Europeaations helped to spread the fungus throughout Europe. Wars with accompanying mass movements of troops and refugees, the general increase in available means of travel, and the rise in the use of occlusive footwear have all combined to make T rubrum the world’s most prevalent dermatophyte.
The first reported case of tinea pedis in the United States was noted in Birmingham, Alabama, in the 1920s. World War I troops returning from battle may have transported T rubrum to the United States.
Pathophysiology
T rubrum, Trichophyton mentagrophytes, and Epidermophyton floccosum most commonly cause tinea pedis, with T rubrum being the most common cause worldwide. Trichophyton tonsurans has also been implicated in children. Nondermatophyte causes include Scytalidium dimidiatum, Scytalidium hyalinum, and, rarely, Candida species.
Using enzymes called keratinases, dermatophyte fungi invade the superficial keratin of the skin, and the infection remains limited to this layer. Dermatophyte cell walls also contain mannans, which can inhibit the body’s immune response. T rubrum in particular contains mannans that may reduce keratinocyte proliferation, resulting in a decreased rate of sloughing and a chronic state of infection.
Temperature and serum factors, such as beta globulins and ferritin, appear to have a growth-inhibitory effect on dermatophytes; however, this pathophysiology is not completely understood. Sebum also is inhibitory, thus partly explaining the propensity for dermatophyte infection of the feet, which have no sebaceous glands. Host factors such as breaks in the skin and maceration of the skin may aid in dermatophyte invasion. The cutaneous presentation of tinea pedis is also dependent on the host’s immune system and the infecting dermatophyte.
Tinea Pedis Clinical Presentation
History
Commonly, tinea pedis patients describe pruritic, scaly soles and, often, painful fissures between the toes. Less often, patients describe vesicular or ulcerative lesions. Some tinea pedis patients, especially elderly persons, may simply attribute their scaling feet to dry skin.
Physical
Patients with tinea pedis have the following 4 possible clinical presentations:
1. Interdigital tinea pedis
- The interdigital presentation is the most characteristic type of tinea pedis, with erythema, maceration, fissuring, and scaling, most often seen between the fourth and fifth toes. This type is often accompanied by pruritus.
- The dorsal surface of the foot is usually clear, but some extension onto the plantar surface of the foot may occur.
- This type can be associated with the dermatophytosis complex, which is an infection with fungi followed by an infection with bacteria.
2. Chronic hyperkeratotic tinea pedis
- The hyperkeratotic type of tinea pedis is characterized by chronic plantar erythema with slight scaling to diffuse hyperkeratosis.
- This type can be asymptomatic or pruritic.This type is also called moccasin tinea pedis, after its moccasinlike distribution. Both feet are usually affected.
- Typically, the dorsal surface of the foot is clear, but, in severe cases, the condition may extend onto the sides of the foot.
3. Inflammatory/vesicular tinea pedis
- Painful, pruritic vesicles or bullae, most often on the instep or anterior plantar surface, characterize the inflammatory/vesicular type.
- The lesions can contain either clear or purulent fluid; after they rupture, scaling with erythema persists.
- Cellulitis, lymphangitis, and adenopathy can complicate this type of tinea pedis.
- The inflammatory/vesicular type can be associated with an eruption called the dermatophytid reaction, which develops on the palmar surface of one or both hands and/or the sides of the fingers. Papules, vesicles, and occasionally bullae or pustules may occur, often in a symmetrical fashion, and it may mimic dyshidrosis (pompholyx). This is an allergy or hypersensitivity response to the infection on the foot, and it contains no fungal elements. The specific explanation of this phenomenon is still unclear. Distinguishing between a dermatophytid reaction and dyshidrosis can be difficult. Dermatophytid reactions are associated with vesicular tinea pedis; therefore, a close inspection of the feet is necessary in patients with vesicular hand dermatoses. The dermatophytid reaction resolves when the tinea pedis infection is treated, and treatment of the hands with topical steroids can hasten resolution.
4. Ulcerative tinea pedis
- The ulcerative variety is characterized by rapidly spreading vesiculopustular lesions, ulcers, and erosions, typically in the web spaces, and is often accompanied by a secondary bacterial infection.
- Cellulitis, lymphangitis, pyrexia, and malaise can accompany this infection.
- Occasionally, large areas, even the entire sole, can be sloughed.
- This type is commonly seen in immunocompromised and diabetic patients.
Patients may have other associated dermatophyte infections, such as onychomycosis, tinea cruris, and tinea manuum. Tinea manuum is often unilateral and associated with moccasin-type tinea pedis (2-feet–1-hand syndrome). One study suggests the scratching habits of the infected individual result in transmission of the dermatophytes from the feet to the hand.
Causes
The interdigital type of tinea pedis is usually caused by T rubrum. It is more pruritic in hot, humid environments. Other possible causative organisms in tinea pedis include T mentagrophytes var interdigitale and E floccosum.
![]() Hyperhidrosis is a risk factor for infection.
Hyperhidrosis is a risk factor for infection.
![]() Candida albicans and bacteria can complicate the process as secondary pathogens.
Candida albicans and bacteria can complicate the process as secondary pathogens.
![]() In 1993, the term dermatophytosis complex was coined to describe the manifestation of moist, oozing, pruritic toe-web spaces from which bacteria, but not dermatophytes, have been isolated. Common culprits include Pseudomonas, Proteus, and Staphylococcus aureus. Experts believe that dermatophytes invade the stratum corneum, paving the way for secondary bacterial infection.
In 1993, the term dermatophytosis complex was coined to describe the manifestation of moist, oozing, pruritic toe-web spaces from which bacteria, but not dermatophytes, have been isolated. Common culprits include Pseudomonas, Proteus, and Staphylococcus aureus. Experts believe that dermatophytes invade the stratum corneum, paving the way for secondary bacterial infection.
The chronic hyperkeratotic type of tinea pedis is usually caused by T rubrum. Other possible causative organisms include T mentagrophytes var interdigitale, E floccosum, and the nondermatophyte molds Scytalidium hyalinum and Scytalidium dimidiatum.
Both the inflammatory/vesicular type of tinea pedis and the ulcerative type of tinea pedis are most commonly caused by the zoophilic fungus T mentagrophytes var mentagrophytes.
A hot, humid, tropical environment and prolonged use of occlusive footwear, with the resulting complications of hyperhidrosis and maceration, are risk factors for all types of tinea pedis. Certain activities, such as swimming and communal bathing, may also increase the risk of infection.
Tinea pedis is more common in some families, and certain people may have a genetic predisposition to the infection. A defect in cell-mediated immunity may predispose some individuals to develop tinea pedis, but this is not certain.
Differential Diagnoses
Laboratory Studies
In suspected tinea pedis, order direct potassium hydroxide (KOH) staining for fungal elements. Usually, the fungal elements are easily identified from scaly lesions. Using counterstains may enhance the visibility of the hyaline hyphae found in dermatophyte infections. Examples include the chitin-specific stains chlorazol black E, which stains hyphae blue-black, and calcofluor, which fluoresces hyphae under a fluorescent microscope.
A sample from skin scrapings may be obtained using a No. 15 blade.
When blisters are present, the highest fungal yield is obtained by scraping the roof of the vesicle.
A fungal culture may be performed to confirm the diagnosis of tinea pedis and to identify the pathogenic species.
Common media include dermatophyte test medium, Mycosel, or mycobiotic agar.
Use caution when choosing the correct culture medium because certain media (eg, dermatophyte test medium) contain cycloheximide, which inhibits the growth of nondermatophyte molds. Because these fungi can be a factor in tinea pedis, use agar without cycloheximide.
Tinea Pedis Treatment & Management
Medication Summary
Tinea pedis can be treated with topical or oral antifungals or a combination of both.Topical agents are used for 1-6 weeks, depending on manufacturers’ recommendations. A patient with chronic hyperkeratotic (moccasin) tinea pedis should be instructed to apply medication to the bottoms and sides of his or her feet. For interdigital tinea pedis, even though symptoms may not be present, a patient should apply the topical agent to the interdigital areas and to the soles because of the likelihood of plantar-surface infection.
Recurrence of tinea pedis is often due to a patient’s discontinuance of medication after symptoms abate. A simple strategy to increase a patient’s compliance is to prescribe a large quantity of topical medicine, which may motivate a patient to continue use until the entire tube is empty.
Moccasin-type tinea pedis is often recalcitrant to topical antifungals alone, owing to the thickness of the scale on the plantar surface. The concomitant use of topical urea or other keratolytics with topical antifungals should improve the response to topical agents. In addition, for moccasin tinea pedis caused by Scytalidium species, Whitfield solution, containing benzoic and salicylic acids, can be beneficial. However, patients with extensive chronic hyperkeratotic tinea pedis or inflammatory/vesicular tinea pedis usually require oral therapy, as do patients with concomitant onychomycosis, diabetes, peripheral vascular disease, or immunocompromising conditions.
Topical imidazoles
Clotrimazole 1% (Mycelex, Lotrimin)
Econazole (Spectazole Topical)
Ketoconazole topical (Nizoral)
Miconazole topical (Monistat)
Oxiconazole 1% cream (Oxistat)
Sertaconazole nitrate cream (Ertaczo)
Topical pyridones
Ciclopirox 1% cream (Loprox)
Topical allylamines
Naftifine 1% cream and gel (Naftin)
Terbinafine topical (Lamisil)
Topical benzylamines
Butenafine (Mentax)
Oral antimycotics
Itraconazole (Sporanox)
Terbinafine (Lamisil, Daskil)
Fluconazole (Diflucan)
Dermatological agents
Ammonium lactate lotion (Lac Hydrin)
![]() Urea, topical (Carmol-40, Keralac)
Urea, topical (Carmol-40, Keralac)
References:
1. Lopez-Martinez R, Manzano-Gayosso P, Hernandez-Hernandez F, Bazan-Mora E, Mendez-Tovar LJ. Dynamics of dermatophytosis frequency in Mexico: an analysis of 2084 cases. Med Mycol. Nov 3 2009;[Medline].
2. Zhan P, Ge YP, Lu XL, She XD, Li ZH, Liu WD. A case-control analysis and laboratory study of the two feet-one hand syndrome in two dermatology hospitals in China. Clin Exp Dermatol. Oct 23 2009;[Medline].
3. Parish LC, Parish JL, Routh HB, Fleischer AB Jr, Avakian EV, Plaum S, et al. A randomized, double-blind, vehicle-controlled efficacy and safety study of naftifine 2% cream in the treatment of tinea pedis. J Drugs Dermatol. Nov 1 2011;10(11):1282-8. [Medline].
4. Weinberg JM, Koestenblatt EK. Treatment of interdigital tinea pedis: once-daily therapy with sertaconazole nitrate. J Drugs Dermatol. Oct 1 2011;10(10):1135-40. [Medline].
5. Carrillo-Muñoz AJ, Tur-Tur C, Cárdenes DC, Estivill D, Giusiano G. Sertaconazole nitrate shows fungicidal and fungistatic activities against Trichophyton rubrum, Trichophyton mentagrophytes, and Epidermophyton 6. floccosum, causative agents of tinea pedis. Antimicrob Agents Chemother. Sep 2011;55(9):4420-1. [Medline]. [Full Text].
7. Matricciani L, Talbot K, Jones S. Safety and efficacy of tinea pedis and onychomycosis treatment in people with diabetes: a systematic review. J Foot Ankle Res. Dec 4 2011;4:26. [Medline]. [Full Text].
TINEA CRURIS
http://emedicine.medscape.com/article/1091806-overview
http://www.youtube.com/watch?v=Hmmgb0zXvAk
Background
Tinea cruris, a pruritic superficial fungal infection of the groin and adjacent skin, is the second most common clinical presentation for dermatophytosis. Tinea cruris is a common and important clinical problem that may, at times, be a diagnostic and therapeutic challenge.
Pathophysiology
The most common etiologic agents for tinea cruris include Trichophyton rubrum and Epidermophyton floccosum; less commonly Trichophyton mentagrophytes and Trichophyton verrucosum are involved. Tinea cruris is a contagious infection transmitted by fomites, such as contaminated towels or hotel bedroom sheets, or by autoinoculation from a reservoir on the hands or feet (tinea manuum, tinea pedis, tinea unguium). The etiologic agents in tinea cruris produce keratinases, which allow invasion of the cornified cell layer of the epidermis. The host immune response may prevent deeper invasion. Risk factors for initial tinea cruris infection or reinfection include wearing tight-fitting or wet clothing or undergarments.
Tinea Cruris Clinical Presentation
Physical
Tinea cruris manifests as a symmetric erythematous rash in the groin, as shown in the images below.
Tinea cruris.
Tinea cruris.
Tinea cruris.
- Large patches of erythema with central clearing are centered on the inguinal creases and extend distally down the medial aspects of the thighs and proximally to the lower abdomen and pubic area.
- Scale is demarcated sharply at the periphery.
- In acute tinea cruris infections, the rash may be moist and exudative.
- Chronic infections typically are dry with a papular annular or arciform border and barely perceptible scale at the margin.
- Central areas typically are hyperpigmented and contain a scattering of erythematous papules and a little scale.
- The penis and scrotum typically are spared in tinea cruris; however, the infection may extend to the perineum and buttocks.
- Secondary changes of excoriation, lichenification, and impetiginization may be present as a result of pruritus.
- Chronic infections modified by the application of topical corticosteroids are more erythematous, less scaly, and may have follicular pustules.
- Approximately one half of patients with tinea cruris have coexisting tinea pedis.
- Erythematous-scale plaques and erythematous-liquenificated plaques were the most frequently found clinical types in an excellent Brazilian study.T rubrum was the prevalent dermatophyte in 90% of the cases, followed by T tonsurans (6%) and T mentagrophytes (4%).
Differential Diagnoses
![]() Familial Benign Pemphigus (Hailey-Hailey Disease)
Familial Benign Pemphigus (Hailey-Hailey Disease)
Laboratory Studies
Microscopic examination of a potassium hydroxide (KOH) wet mount of scales is diagnostic in tinea cruris. The procedure for KOH wet mount is as follows:
o Clean the area with 70% alcohol.
o Collect scales from the margin of the lesion; use a scalpel or the edge of a glass slide for this purpose. Cover the collected scales with a cover slip; allow a drop of KOH (10-15% wt/vol) to run under the cover slip.
o The keratin and debris should dissolve after a few minutes. The process can be hastened by heating the slide or by the addition of a keratolytic or dimethyl sulfoxide to the KOH formulation.
o The addition of 1 drop of lactophenol cotton blue solution to the wet mount preparation heightens the contrast and aids in the diagnosis.
o Negative results on KOH preparation do not exclude fungal infection.
o Scale culture is useful for fungal identification but is a more specific, albeit less sensitive, diagnostic test than KOH wet mount.
![]() Growth on Mycosel or Sabouraud agar plates usually is sufficient within 3-6 weeks to allow specific fungal identification.
Growth on Mycosel or Sabouraud agar plates usually is sufficient within 3-6 weeks to allow specific fungal identification.
Tinea Cruris Treatment
Medical Care
Clinical cure of an uncomplicated tinea cruris infection usually can be achieved using topical antifungal agents of the imidazole or allylamine family. Consider patients unable to use topical treatments consistently or with extensive or recalcitrant infection as candidates for systemic administration of antifungal therapy, which has been proven safe in immunocompetent persons.
Prevention of tinea cruris reinfection is an essential component of disease management. Patients with tinea cruris often have concurrent dermatophyte infections of the feet and hands.
- Treat all active areas of tinea cruris infection simultaneously to prevent reinfection of the groin from other body sites.
- Advise patients with tinea pedis to put on their socks before their undershorts to reduce the possibility of direct contamination.
- Advise patients with tinea cruris to dry the crural folds completely after bathing and to use separate towels for drying the groin and other parts of the body.
Medication Summary
To achieve the best results, particularly with follicular or extensive tinea cruris, the authors often recommend a combination of topical and systemic therapy.
Antifungal agents
Terbinafine (Lamisil)
Butenafine (Mentax)
Clotrimazole topical (Lotrimin, Mycelex)
Miconazole (Micatin, Monistat-Derm)
Ketoconazole topical (Nizoral)
Econazole (Spectazole)
Naftifine (Naftin)
Oxiconazole (Oxistat)
Tolnaftate (Tinactin)
Ciclopirox (Loprox)
Itraconazole (Sporanox)
Sulconazole (Exelderm)
References:
1. Yehia MA, El-Ammawi TS, Al-Mazidi KM, Abu El-Ela MA, Al-Ajmi HS. The Spectrum of Fungal Infections with a Special Reference to Dermatophytoses in the Capital Area of Kuwait During 2000-2005: A Retrospective Analysis. Mycopathologia. Nov 17 2009;[Medline].
2. Koksal F, Er E, Samasti M. Causative agents of superficial mycoses in Istanbul, Turkey: retrospective study. Mycopathologia. Sep 2009;168(3):117-23. [Medline].
3. Parish LC, Parish JL, Routh HB, Avakian E, Olayinka B, Pappert EJ, et al. A double-blind, randomized, vehicle-controlled study evaluating the efficacy and safety of naftifine 2% cream in tinea cruris. J Drugs Dermatol. Oct 1 2011;10(10):1142-7. [Medline].
TINEA BARBAE
http://emedicine.medscape.com/article/1091252-overview
http://www.youtube.com/watch?v=x9tyMh6WFP8
Background
Tinea barbae is a superficial dermatophyte infection that is limited to the bearded areas of the face and neck and occurs almost exclusively in older adolescent and adult males. The clinical presentation of tinea barbae includes inflammatory, deep, kerionlike plaques and noninflammatory superficial patches resembling tinea corporis or bacterial folliculitis.
Pathophysiology
Tinea barbae is caused by the keratinophilic fungi (dermatophytes) that are responsible for most superficial fungal skin infections. They infect the stratum corneum of the epidermis, hair, and nails. Several enzymes, including keratinases, are released by dermatophytes, which help them invade the epidermis. The mechanism that causes tinea barbae is similar to that of tinea capitis. In both diseases, hair and hair follicles are invaded by fungi, producing an inflammatory response. Tinea barbae is caused by both zoophilic and anthropophilic dermatophytes.
Infection caused by zoophilic dermatophytes usually is of greater severity than that produced by anthropophilic organisms. Thus, zoophilic dermatophytes are the primary cause of inflammatory kerionlike plaques, which most likely result from a more intense host reaction. Kerion formation has been described as resulting from Trichophyton rubrum infection.T rubrum, an anthropophilic dermatophyte, can invade hair shafts and deeper tissues (although rarely), resulting in an inflammatory reaction. Usually, infection involving hair is more severe; therefore, tinea barbae caused by anthropophilic dermatophytes often has a more severe course than tinea corporis caused by the same pathogen.
The formation of kerion is postulated by 2 theories. The first theory suggests that it results from diffusion of metabolites and/or toxins from the fungus; however, kerion formation most likely results from an immunologic response to dermatophyte antigens.
Tinea Barbae Clinical Presentation
Physical
Clinical manifestations of tinea barbae relate to the causative pathogen. Two clinical varieties of the disease are identified as follows:
Inflammatory deeper tinea barbae is caused primarily by zoophilic dermatophytes. This variety, termed a kerion, is the most common clinical presentation. Most patients show solitary plaques or nodules; however, multiple plaques are relatively common. Usually localized on the chin, cheeks, or neck, involvement of the upper lip is rare. The characteristic lesion is an inflammatory reddish nodule with pustules and draining sinuses on the surface. Hairs are loose or broken, and depilation is easy and painless. Pus-filled whitish masses involve the hair root and follicle. Over time, the surface of the indurated nodule is covered by exudate and crust. This variety of tinea barbae usually is associated with generalized symptoms, such as regional lymphadenopathy, malaise, and fever.
Noninflammatory superficial tinea barbae is caused by anthropophilic dermatophytes. This variety of barbae is less common and resembles common tinea corporis or bacterial folliculitis (sycosiform variety). Typically, erythematous patches show an active border composed of papules, vesicles, and/or crusts. Hairs are brokeext to the skin, or they plug the hair follicle. In the sycosiform variety, small follicular pustules are observed. Hairs are broken or loose. This variety represents a chronic variant of tinea barbae.
Inflammatory tinea barbae resulting from Trichophyton mentagrophytesvar granulosuminfection.
Wax model of kerionlike tinea barbae. Courtesy of the Museum of the Department of Dermatology, University of Medicine, Wroclaw, Poland.
Causes
Tinea barbae is caused by several dermatophytes, including zoophilic and anthropophilic organisms; however, zoophilic dermatophyte infection occurs more commonly. Frequently, animals (eg, cattle, horses, cats, dogs) constitute the source of infection.Trichophyton species are most common, thus the term trichophytosis barbae also is used. Among zoophilic dermatophytes, Trichophyton mentagrophytes var granulosum and Trichophyton verrucosum are the most common causative agents Microsporum canis and Trichophyton mentagrophytes var erinacei may cause tinea barbae but are rare.
T rubrum and Trichophyton violaceum are the most common anthropophilic dermatophytes responsible for tinea barbae; however, infections from Trichophyton megninii (endemic in Sardinia, Sicily, Portugal) and Trichophyton schoenleinii (endemic in Eurasia, Africa, Brazil) also may occur, especially in endemic regions. Infection of bearded skin by anthropophilic dermatophytes may be the result of autoinoculation from tinea pedis or onychomycosis.
Other reported causative organisms include Trichophyton interdigitale and Microsporum nanum.
Differential Diagnoses
Tinea Barbae Medication
Medication Summary
Antifungals
Griseofulvin (Fulvicin P/G, Grifulvin V)
Terbinafine (Lamisil)
Itraconazole (Sporanox)
Fluconazole (Diflucan)
References:
1. Szepietowski JC, Matusiak L. Trichophyon rubrum autoinoculation from infected nails is not such a rare phenomenon. Mycoses. 2008;51:345-346.
2. Sander CS, Sander O, Khatib A, Berger T. Tinea barbae spreading to locus minoris resistentiae. Eur J Dermatol. Mar-Apr 2009;19(2):173-4. [Medline].
PITURIASIS VERSICOLOR
http://emedicine.medscape.com/article/1091575-overview
http://www.metacafe.com/watch/9540867/tinea_versicolor_pityriasis_versicolor/
Background
Tinea versicolor is a common, benign, superficial cutaneous fungal infection usually characterized by hypopigmented or hyperpigmented macules and patches on the chest and the back. In patients with a predisposition, tinea versicolor may chronically recur. The fungal infection is localized to the stratum corneum. Note the image below.
In patients with lighter skin color, lesions frequently are light tan or salmon colored.
Pathophysiology
Tinea versicolor is caused by the dimorphic, lipophilic organisms in the genus Malassezia, formerly known as Pityrosporum. Eleven species are recognized within this classification of yeasts, of which Malassezia globosa and Malassezia furfur are the predominant species isolated in tinea versicolor.Malassezia is extremely difficult to propagate in laboratory culture and is culturable only in media enriched with C12- to C14-sized fatty acids. Malassezia is naturally found on the skin surfaces of many animals, including humans. Indeed, it can be isolated in 18% of infants and 90-100% of adults.
The organism can be found on healthy skin and on skin regions demonstrating cutaneous disease. In patients with clinical disease, the organism is found in both the yeast (spore) stage and the filamentous (hyphal) form. Factors that lead to the conversion of the saprophytic yeast to the parasitic, mycelial morphologic form include a genetic predisposition; warm, humid environments; immunosuppression; malnutrition; and Cushing disease. Human peptide cathelicidin LL-37 plays a role in skin defense against this organism.
Even though Malassezia is a component of the normal flora, it can also be an opportunistic pathogen. The organism is considered to be a factor in other cutaneous diseases, including Pityrosporum folliculitis, confluent and reticulate papillomatosis, seborrheic dermatitis, and some forms of atopic dermatitis. Malassezia species have also been shown to be a pulmonary pathogen in patients with immunosuppression due to stem cell transplantation.
Clinical Presentation
Tinea versicolor can present in 4 forms.
1. Tinea versicolor – Form 1
The most common appearance of the disease is as numerous, well-marginated, finely scaly, oval-to-round macules scattered over the trunk and/or the chest, with occasional extension to the lower part of the abdomen, the neck, and the proximal extremities.
The macules tend to coalesce, forming irregularly shaped patches of pigmentary alteration. As the name versicolor implies, the disease characteristically reveals a variance in skin hue. The involved areas can be either darker or lighter than the surrounding skin.
The condition is more noticeable during the summer months when the discrepancy in color from the normal skin becomes more apparent.
Light scraping of the involved skin with a scalpel blade characteristically yields a copious amount of keratin.
2. Tinea versicolor – Form 2
An inverse form of tinea versicolor also exists in which the condition has an entirely different distribution, affecting the flexural regions, the face, or isolated areas of the extremities. This form of tinea versicolor is more often seen in hosts who are immunocompromised.
This form of the disease can be confused with candidiasis, seborrheic dermatitis, psoriasis, erythrasma, and dermatophyte infections.
3. Tinea versicolor – Form 3
The third form of Malassezia infections of the skin involves the hair follicle. This condition is typically localized to the back, the chest, and the extremities.
This form can be clinically difficult to differentiate from bacterial folliculitis. The presentation of Pityrosporum folliculitis is a perifollicular, erythematous papule or pustule.
Predisposing factors include diabetes, high humidity, steroid or antibiotic therapy, and immunosuppressant therapy. Additionally, several reports reveal that M furfur also plays a role in seborrheic dermatitis.
4. Tinea versicolor – Form 4
Another clinical presentation is multiple firm, 2- to 3-mm, monomorphic, red-brown, inflammatory papules. These lesions may, or may not also demonstrate a fine white scale.
The lesions are usually found on the torso and are asymptomatic.
Histologically, the rash demonstrates not only fungal hyphae and spores in the stratum corneum, but also an interface dermatitis in the superficial dermis.
Causes
Most cases of tinea versicolor occur in healthy individuals with no immunologic deficiencies. Nevertheless, several factors predispose some people to develop this condition. These factors include genetic predisposition; warm, humid environments; immunosuppression; malnutrition; application of oily preparations; corticosteroid usage; and Cushing disease.
The reason why this organism causes tinea versicolor in some individuals while remains as normal flora in others is not entirely known. Several factors, such as the organism’s nutritional requirements and the host’s immune response to the organism, are significant.
The organism is lipophilic, and lipids are essential for growth in vitro and in vivo. Furthermore, the mycelial stage can be induced in vitro by the addition of cholesterol and cholesterol esters to the appropriate medium. Because the organism more rapidly colonizes humans during puberty when skin lipids are increased more than that of adolescent levels and tinea versicolor is manifested in sebum-rich areas (eg, chest, back), individual variations in skin surface lipids are hypothesized to play a major role in disease pathogenesis. However, patients with tinea versicolor and control subjects do not demonstrate any quantitative or qualitative differences in skin surface lipids. Skin surface lipids are significant for the normal presence of M furfur on human skin, but they probably play little role in the pathogenesis of tinea versicolor.
Evidence has been accumulating to suggest that amino acids, rather than lipids, are critical for the appearance of the diseased state. In vitro, the amino acid asparagine stimulates the growth of the organism, while another amino acid, glycine, induces hyphal formation. In vivo, the amino acid levels have been shown to be increased in the uninvolved skin of patients with tinea versicolor in 2 separate studies.
Another significant causative factor is the patient’s immune system. Although sensitization against M furfur antigens is routinely present in the general population (as proven by lymphocyte transformation studies), lymphocyte function on stimulation with the organism has been shown to be impaired in patients who are affected. This outcome is similar to the situation of sensitization with Candida albicans. In short, cell-mediated immunity plays some role in disease causation.
Oxidative stress as shown by expression of reduced glutathione contributes to the pathogenesis of this condition.
Differential Diagnoses
Laboratory Studies
The clinical presentation of tinea versicolor is distinctive, and the diagnosis is often made without any laboratory documentation.
The ultraviolet black (Wood) light can be used to demonstrate the coppery-orange fluorescence of tinea versicolor. However, in some cases, the lesions appear darker than the unaffected skin under the Wood light, but they do not fluoresce.
The diagnosis is usually confirmed by potassium hydroxide (KOH) examination, which demonstrates the characteristic short, cigar-butt hyphae that are present in the diseased state. The KOH finding of spores with short mycelium has been referred to as the spaghetti and meatballs or the bacon and eggs sign of tinea versicolor. For better visualization, ink blue stain, Parker ink, methylene blue stain, or Swartz-Medrik stain can be added to the KOH preparation. Contrast stain containing 1% Chicago sky blue 6B and 8% KOH (as the clearing agent) achieves the greatest sensitivity and specificity.
Special media are required for culture. Because the diagnosis is usually clinically suspected and can be confirmed with a KOH preparation, cultures are rarely obtained.
With blood examination, no definitive deficiencies of normal antibodies or complement are present in patients with tinea versicolor, but research continues in this area. For example, although individuals who are affected reveal no specific antibody levels above those of age-matched controls, M furfur antigens do elicit a specific immunoglobulin G response in patients with seborrheic dermatitis and tinea versicolor detected by enzyme-linked immunosorbent assay and Western blotting assays. M furfur does induce immunoglobulin A, immunoglobulin G, and immunoglobulin M antibodies, and it can activate complement via both the alternate pathway and the classical pathway.
Various studies have found defects in lymphokine production, natural killer T cells, decreased phytohemagglutinin and concanavalin A stimulation, interleukin 1, interleukin 10, and interferon gamma production by lymphocytes in patients.
Although these tests do not suggest an immunologic disorder, they do suggest a reduced body response to the specific fungal elements that produce tinea versicolor. Further assessment is warranted.
Tinea Versicolor Treatment
Medical Care
Patients should be informed that tinea versicolor is caused by a fungus that is normally present on the skin surface and is therefore not considered contagious. The condition does not leave any permanent scar or pigmentary changes, and any skin color alterations resolve within 1-2 months after treatment has been initiated. Recurrence is common, and prophylactic therapy may help reduce the high rate of recurrence.
Tinea versicolor can be successfully treated with various agents. Effective topical agents include selenium sulfide, sodium sulfacetamide, ciclopiroxolamine, as well as azole and allylamine antifungals. Various regimens can be used. Selenium sulfide lotion is liberally applied to affected areas of the skin daily for 2 weeks; each application is allowed to remain on the skin for at least 10 minutes prior to being washed off. In resistant cases, overnight application can be helpful. Topical azole antifungals can be applied every night for 2 weeks. Weekly applications of any of the topical agents for the following few months may help prevent recurrence. In patients with widespread disease, topical antifungal therapy can be expensive. Topical allylamines have been demonstrated to be clinically and mycologically effective.
Oral therapy is also effective for tinea versicolor and is often preferred by patients because it is more convenient and less time consuming. Of course, oral therapy can be used in consort with topical regimens. Ketoconazole, fluconazole, and itraconazole are the preferred oral agents. Various dosing regimens have been used. With ketoconazole, a 10-day 200-mg daily therapy and as a single-dose 400-mg treatment are popular, both with comparable results. Fluconazole has been offered as a single 150- to 300-mg weekly dose for 2-4 weeks. Itraconazole is usually given at 200 mg/d for 7 days. Pramiconazole and sertaconazole have also been used in the management of tinea versicolor.
Oral therapy does not prevent the high rate of recurrence, and treatment with oral ketoconazole or a topical agent may need to be repeated intermittently throughout the year. Because tinea versicolor is a benign condition and oral therapy is not without risk, the decision to treat with an oral agent should be made only after a complete discussion of the risks involved.In the case of oral terbinafine, some subgroups of M furfur apparently are not clinically responsive, although in vitro studies suggest fungistatic activity.Also, a regimen of 1 tablet a month of ketoconazole, fluconazole, and itraconazole has been used successfully to prophylactically prevent recurrences.
Medical Care
Patients should be informed that tinea versicolor is caused by a fungus that is normally present on the skin surface and is therefore not considered contagious. The condition does not leave any permanent scar or pigmentary changes, and any skin color alterations resolve within 1-2 months after treatment has been initiated. Recurrence is common, and prophylactic therapy may help reduce the high rate of recurrence.
Tinea versicolor can be successfully treated with various agents. Effective topical agents include selenium sulfide, sodium sulfacetamide, ciclopiroxolamine,as well as azole and allylamine antifungals.Various regimens can be used. Selenium sulfide lotion is liberally applied to affected areas of the skin daily for 2 weeks; each application is allowed to remain on the skin for at least 10 minutes prior to being washed off. In resistant cases, overnight application can be helpful. Topical azole antifungals can be applied every night for 2 weeks. Weekly applications of any of the topical agents for the following few months may help prevent recurrence. In patients with widespread disease, topical antifungal therapy can be expensive. Topical allylamines have been demonstrated to be clinically and mycologically effective.
Oral therapy is also effective for tinea versicolor and is often preferred by patients because it is more convenient and less time consuming. Of course, oral therapy can be used in consort with topical regimens. Ketoconazole, fluconazole, and itraconazole are the preferred oral agents. Various dosing regimens have been used. With ketoconazole, a 10-day 200-mg daily therapy and as a single-dose 400-mg treatment is popular, both with comparable results. Fluconazole have been offered as a single 150- to 300-mg weekly dose for 2-4 weeks. Itraconazole is usually given at 200 mg/d for 7 days. Pramiconazole and sertaconazole have also been used in the management of tinea versicolor.
Oral therapy does not prevent the high rate of recurrence, and treatment with oral ketoconazole or a topical agent may need to be repeated intermittently throughout the year. Because tinea versicolor is a benign condition and oral therapy is not without risk, the decision to treat with an oral agent should be made only after a complete discussion of the risks involved.In the case of oral terbinafine, some subgroups of M furfur apparently are not clinically responsive, although in vitro studies suggest fungistatic activity.Also, a regimen of 1 tablet a month of ketoconazole, fluconazole, and itraconazole has been used successfully to prophylactically prevent recurrences.
Antifungals
Terbinafine topical (Lamisil)
Clotrimazole topical (Mycelex, Lotrimin-AF)
Ketoconazole (Nizoral)
Ciclopirox (Loprox)
Butenafine (Mentax)
Naftifine (Naftin)
Econazole (Spectazole)
Oxiconazole (Oxistat)
References:
1. Krisanty RI, Bramono K, Made Wisnu I. Identification of Malassezia species from pityriasis versicolor in Indonesia and its relationship with clinical characteristics. Mycoses. May 2009;52(3):257-62. [Medline].
2. Blaes AH, Cavert WP, Morrison VA. Malassezia: is it a pulmonary pathogen in the stem cell transplant population?. Transplant Infectious Disease. August, 2009;11:313-317. [Medline].
3. Muhammad N, Kamal M, Islam T, Islam N, Shafiquzzaman M. A study to evaluate the efficacy and safety of oral fluconazole in the treatment of tinea versicolor. Mymensingh Med J. Jan 2009;18(1):31-5. [Medline].
4. Mendez-Tovar LJ. Pathogenesis of dermatophytosis and tinea versicolor. Clinics in Dermatology. 2010;28:185-188. [Medline].
5. Wahab MA, Ali ME, Rahman MH, Chowdhury SA, Monamie NS, Sultana N, et al. Single dose (400mg) versus 7 day (200mg) daily dose itraconazole in the treatment of tinea versicolor: a randomized clinical trial. Mymensingh Med J. Jan 2010;19(1):72-6. [Medline].
6. Kilic M, Oguztuzum S, Karadag S, Cakir E, Aydin M, Ozturk L. Expression of GSTM4 and GSTT1 in patients with Tinea versicolor, Tinea inguinalis, and Tinea pedis infections: a preliminary study. Clinical Dermatology. 2011;36:590-594. [Medline].
7. Gold M, Bridges T, Avakian E, Plaum S, Pappert EJ, Fleischer AB, et al. An open-label study of naftifine hydrochloride 1% gel in the treatment of tinea versicolor. Skin Med. Sept 2011;9:283-6. [Medline].
CUTANEOUS AND NAIL CANDIDIASIS
1. http://emedicine.medscape.com/article/1090632-overview
2. http://www.youtube.com/watch?v=x3zcpK_m-cM&feature=pyv
Background
Cutaneous candidiasis and other forms of candidosis are infections caused by the yeast Candida albicans or other Candida species. Yeasts are unicellular fungi that typically reproduce by budding, a process that entails a progeny pinching off of the mother cell. C albicans, the principal infectious agent in human infection, is an oval yeast 2-6 µm in diameter. C albicans (as well as most medically significant fungi) has the ability to exist in both hyphal and yeast forms (termed dimorphism). If pinched cells do not separate, a chain of cells is produced and is termed pseudohyphae.
Superficial infections of skin and mucous membranes are the most common types of candidal infections of the skin. Common types of candidal skin infection include intertrigo, diaper dermatitis, erosio interdigitalis blastomycetica, perianal dermatitis, and candidal balanitis. In certain subpopulations, candidal infection of the skin has increased in prevalence in recent years, principally because of the increased numbers of patients who are immunocompromised.
Esophagitis, septicemia, endocarditis, peritonitis, and urinary tract infections are less frequent types of candidosis. Although C albicans is the most common cause of human infection, the genus Candida includes more than 150 species. Candida tropicalis, Candida parapsilosis, Candida guilliermondi, Candida krusei, Candida kefyr, Candida zeylanoides, and Candida glabrata (formerly Torulopsis glabrata) are less common causes of human disease.
Humans carry yeast fungi, including candidal species, throughout the gastrointestinal tract (mouth through anus) as part of the normal commensal flora. The vagina also commonly is colonized by yeast (13% of women), most commonly by C albicans and C glabrata. The commensal oral isolation of candidal species ranges from 30-60% in healthy adults. Note that Candida species are not part of the normal flora of the skin; however, they may colonize fingers or body folds transiently.
Pathophysiology
Most candidal species are known to produce virulence factors including protease factors. Those strains lacking virulence factors have been shown to be less pathogenic. The ability of yeast forms to adhere to the underlying epithelium is an important step in the production of hyphae and tissue penetration. Removal of bacteria from the skin, mouth, and gastrointestinal tract by exposing to tissue with its endogenous flora results in inhibition of endogenous microflora, providing reduced environmental and nutritional competition that favors the growth of candidal organisms.
Additional research has been performed on the cytokines and interleukins that candidal organisms affect in keratinocytes. In keratinocytes, C albicans phospholipomannan triggers an inflammatory response through toll-like receptor 2. C albicans aborts the expression of interferon-gamma–inducible protein-10 in human keratinocytes. These factors probably explain how candidal infections occur in the skin, which has innate defenses against candidal organisms.
Clinical Presentation
History
Candidal vulvovaginitis: This common condition in women presents with itching, soreness, and a thick creamy white discharge (see the image below).
A moist, erosive, pruritic patch of the perianal skin and perineum (with satellite pustule formation) is demonstrated in this woman with extensive candidosis.
Although most candidal infections occur more frequently with advancing age, vulvovaginitis is unusual in older women. In the absence of estrogen stimulation, the vaginal mucosa becomes thin and atrophic, producing less glycogen. Candidal colonization of vaginal mucosa is estrogen dependent and subsequently decreases sharply after menopause (see the image below).
Discrete superficial pustules developed within hours of birth on the hand of an otherwise healthy newborn. A potassium hydroxide preparation revealed spores and pseudomycelium, and culture demonstrated the presence of Candida albicans.
In contrast, the likelihood of colonization increases during pregnancy (25-33%). The widespread use of hormone replacement for reduction of osteoporosis and heart disease may cause an increasing trend in candidal vulvovaginitis among older women. Cutaneous hypersensitivity to C albicans has been reported in persons with idiopathic vulvodynia.
Candidal balanitis: Signs and symptoms of this candidal infection vary but may include tiny papules, pustules, vesicles, or persistent ulcerations on the glans penis (see the image below).
Exacerbations following intercourse are common. Dry, red, superficially scaly, pruritic macules and patches on the penis represent candidal balanitis.
Congenital candidosis: This rarely reported candidal infection (70 cases during the 1990s) may be acquired by the infant in utero or during delivery. Presumably, congenital candidosis is an ascending intrauterine infection with cutaneous or systemic manifestations that typically present within 12 hours after birth. Although the congenital systemic form typically is fatal, congenital cutaneous infections usually have a more benign course. Prematurity and the presence of an intrauterine foreign body (intrauterine device) are associated with this condition. Untreated, infants are at higher risk for systemic infection, which is associated with a high mortality rate (70%). Some infants have respiratory distress and pneumonia secondary to in utero aspiration of infected amniotic fluid.
Oropharyngeal candidiasis : This form is known more commonly as oral thrush and is considered by many to be a minor problem of little significance that may clear spontaneously. However, without appropriate treatment this can lead to a chronic condition that can result in discomfort and anorexia. Rarely, oropharyngeal infection leads to systemic candidiasis.
Oropharyngeal candidiasis in the neonate most commonly is acquired from the infected maternal mucosa during passage of the infant through the birth canal. Oropharyngeal candidiasis is 35 times more common ieonates of infected mothers compared to uninfected mothers.
Oropharyngeal candidiasis is the most common type of clinical presentation in infants and children. Immaturity of host defenses and incomplete establishment of the normal orointestinal flora are likely reasons why C albicans often acts as a pathogen in the neonate compared to a child aged several months who is not nearly as susceptible. Beyond the neonatal age, C albicans is considered a normal constituent of the oral and intestinal florae.
Candidosis of the nipple in the nursing mother is associated with infantile oropharyngeal candidiasis. Nipple candidosis almost always is bilateral, with the nipples appearing bright red and inflamed, with the look and feel of being sunburned or on fire. Unlike a painful-with-nursing cut or abrasion from local trauma by the infant (incorrect latch-on), nipple candidosis hurts between feedings. Merely having the clothing brush against the nipples is painful.
Candidal diaper dermatitis: Infants with oropharyngeal candidiasis invariably harbor C albicans in the intestine and feces (85-90%). In most patients, candidal diaper dermatitis is the result of progressive colonization from oral and gastrointestinal candidiasis. Infected stools represent the most important focus for cutaneous infection. Moist macerated skin is particularly susceptible to invasion by C albicans. Additional factors that predispose infants to candidal diaper dermatitis include local irritation of the skin by friction; ammonia from bacterial breakdown of urea, intestinal enzymes, and stool; detergents; and disinfectants.
Oral candidiasis in adults: Use of broad-spectrum antibiotics and inhaled corticosteroids, diminished cell-mediated immunity, and xerostomia are all risk factors for candidiasis (see the image below).
White plaques are present on the buccal mucosa and the undersurface of the tongue and represent thrush. When wiped off, the plaques leave red erosive areas.
Xerostomia may be either primary resulting from the natural aging process or secondary resulting from the anticholinergic effect of certain drugs including psychoactive drugs such as phenothiazines and tricyclic antidepressants. A decrease in salivary production decreases both the amount of available mucosal secretory antibody (immunoglobulin A [IgA]) and the natural cleansing action provided by saliva.
In older adults, the development of oral thrush in the absence of a known etiology should raise the clinician’s index of suspicion for an underlying cause of immunosuppression, such as malignancy or AIDS. Superficial mycoses may be the presenting sign in immunodepressed patients (especially AIDS).
With denture stomatitis, the areas of erythema may be painful and may affect up to 65% of patients who wear dentures, especially those who wear full sets. Despite popular belief, denture stomatitis is not associated with smokers or patients who are immunosuppressed.
Intertrigo: Most cases of cutaneous candidosis occur in skin folds where occlusion (by clothing or shoes) produces abnormally moist conditions. Sites such as the perineum, mouth, and anus, in which Candida organisms normally may be carried, are at further risk of infection. Candidal infection of the skin under the breasts or pannus occurs when those areas become macerated (see the image below).
Erythema, maceration, and satellite pustules in the axilla, accompanied by soreness and pruritus result in a form of intertrigo.
Decubital candidosis: This is a particular form of cutaneous candidosis that occurs on the dorsal skin of chronically bedridden patients.
Paronychia: Candida organisms occasionally cause infection in the periungual area and underneath the nailbed (see the image below). Candida species (not always C albicans) can be isolated from most patients with chronic paronychia. The yeast is believed to play an etiologic role in this condition, but bacteria also may act as co-pathogens. Immediate contact dermatitis to food allergens may play a role in the pathogenesis of the condition as well. Progression to total nail dystrophy has been associated specifically with C albicans and usually has been limited to women with 2 important predisposing conditions, ie, Cushing syndrome and Raynaud disease. Disease is more common in people who frequently submerge their hands in water and usually is not associated with the elderly population. One important exception to this generalization is the population of patients with diabetes.
A nailfold with candidal infection becomes erythematous, swollen, and tender with an occasional discharge
Candidosis and HIV: Epidemiologic studies indicate that a very high percentage of patients infected with HIV contract some type of skin disorder during the course of the disease. More specifically, most patients with HIV infection have some form of candidal infection during the illness. Recurrent episodes of oral candidiasis typically occur in patients in whom CD4 counts are less than 300/µL, an important marker of disease progression. Additionally, Yanagisawa et al, in 2007, reported on a case of disseminated candidiasis as an initial presentation of AIDS. Such cases often manifest with purpuric eruptions.
Chronic mucocutaneous candidiasis: See Candidiasis, Chronic Mucocutaneous for discussion of that form of candidiasis.
Breast pain: Andrews et al studied 98 breastfeeding women, 20 who reported breastfeeding associated pain and 78 who were asymptomatic. Cultures were obtained from breast milk, areolae, and the infants’ oropharynx. Six of the 20 symptomatic women returned breast milk cultures positive for yeast, compared with 6 of 78 controls (11 of 12 samples showed C albicans). The researchers suggested that Candida might play an etiologic role in breastfeeding-associated pain.
Ecthyma gangrenosum: In 2007, Agarwal et al reported on a solitary ecthyma gangrenosum–like lesion that resulted from C albicans infection in a neonate.
Ulcers: Xi et al, in 2007, reported a 51-year-old Cantonese woman who had a 1-year history of a large, deep-seated subcutaneous ulcer on her right shoulder for more than a year whose discharge showed C albicans and C parapsilosis. The researchers isolated C parapsilosis from the biopsy specimen.
Cutaneous candidiasis has manifested as an interdigital ulcer.
Cutaneous candidiasis was noted to occur under a ruby ring in a patient who was immunocompromised.
Physical
· Candidal vulvovaginitis: Clinical examination reveals erythema of the vaginal mucosa and vulval skin with curdy white flecks within the discharge. Erythema may spread to include the perineum and groin, with satellite pustules. Alternatively, the vaginal mucosa may appear red and glazed. A patient presenting with symptoms of vulvovaginitis with identification of yeasts in the vaginal discharge has a diagnosis of candidosis.
· Congenital candidosis: In 2004, Diana et alreported that cutaneous congenital candidiasis is a rare disease of term or premature infants. It typically manifests as an erythematous maculopapular eruption affecting the trunk and extremities; it resolves after extensive desquamation. Pustules and vesicles usually are superficial and resolve spontaneously or with topical treatment (see the image below). The presence of white microabscesses on the placenta and umbilical cord of an infant with such an eruption must suggest the diagnosis of cutaneous congenital candidiasis. It is always secondary to candidal chorioamnionitis, but it may pass unrecognized.
Fine superficial pustules on an erythematous patchy base are suggestive of candidosis.
· Oropharyngeal candidiasis in the infant: Lesions become visible as pearly white patches on the mucosal surfaces. Buccal epithelium, gums, and the palate commonly are involved with extension to the tongue, pharynx, or esophagus in more severe cases. If the lesions are scraped away, an erythematous base is exposed. Lesions may progress to symptomatic erosion and ulceration.
· Candidal diaper dermatitis: The eruption of candidal diaper dermatitis usually starts in the perianal area, spreading to involve the perineum and, in severe cases, the upper thighs, lower abdomen, and lower back. Maceration of the anal mucosa and the perianal skin often is the first clinical manifestation. The typical eruption begins with scaly papules that merge to form well-defined, weeping, eroded lesions with a scalloped border. A collar of overhanging scales and an erythematous base may be demonstrated. Satellite flaccid vesicopustules around the primary intertriginous plaque also are characteristic of candidal diaper dermatitis and represent the primary lesions. Candidiasis may be a presenting feature of diabetic ketoacidosis.
· Oral candidiasis in elderly persons: The most common clinical appearance of oropharyngeal candidiasis (pseudomembranous candidosis or oral thrush) in the adult population occurs as white plaques that are present on the buccal, palatal, or oropharyngeal mucosa overlying areas of mucosal erythema. Typically, the lesions are removed easily and may demonstrate areas with tiny ulcerations (see the image below). In addition, some patients may develop soreness and cracks at the lateral angles of the mouth (angular cheilitis). Denture stomatitis presents as chronic mucosal erythema typically beneath the site of a denture.
Soreness and cracks at the lateral angles of the mouth (angular cheilitis) is a frequent expression of candidosis in elderly individuals.
· Intertrigo: Intertrigo typically presents with erythema, cracking, and maceration with soreness and pruritic symptoms. Lesions typically have an irregular margin with surrounding satellite papules and pustules. Web spaces of affected fingers or toes are macerated and have the appearance of soft white skin, which is a condition termed erosio interdigitalis blastomycetica (interdigital candidosis).
· Paronychia: The nailfold becomes erythematous, swollen, and tender, with an occasional discharge. Loss of the cuticle occurs, along with nail dystrophy and onycholysis with discoloration around the lateral nailfold (see the image below). A greenish color with hyponychial fluid accumulation may occur that results entirely from Candida, and not Pseudomonas, infection. A potassium hydroxide (KOH) preparation is helpful and is likely to show yeast organisms.
Candida infection should be in the differential diagnosis when one or more nails become discolored, has subungual discoloration, nailplate separation from the nailbed, and lack evidence of a dermatophyte.
Causes
- Host factors that predispose patients to infections are numerous. Local factors such as tissue damage resulting from trauma, xerostomia, radiation-induced mucositis, ulcerations, skin maceration, or occlusion enhances adhesion and predisposes patients to increased infection rates.
- Endocrine diseases such as diabetes mellitus, Cushing syndrome, hypoparathyroidism, hypothyroidism, and polyendocrinopathy are associated with increased susceptibility to infection. The mechanism by which diabetes mellitus is believed to raise infection rates is through increased tissue glucose, altered yeast adhesion, and decreased phagocytosis.
- Nutritional deficiencies may alter host defense mechanisms or epithelial barrier integrity, allowing increased adherence or penetration. Iron deficiency anemia and deficiencies including vitamins B1, B2, B6, C, and folic acid are associated with heightened infection rates.
- T-lymphocyte–mediated immunity plays an important immunologic role against infection through phagocytosis and killing by polymorphonuclear cells and macrophages. Individuals with deficient T-lymphocyte function, such as patients with AIDS, appear to be particularly vulnerable to mucosal or cutaneous candidiasis but not to systemic infection. Patients with primary immune deficiencies, such as lymphocytic abnormalities, phagocytic dysfunction, IgA deficiency, viral-induced immune paralysis, and severe congenital immunodeficiencies, often are affected by oropharyngeal candidiasis and other fungal mycoses.
Differential Diagnoses
Laboratory Studies
1. http://thunderhouse4-yuri.blogspot.com/2009/12/candida-albicans.html
2. http://www.youtube.com/watch?v=thuWQB2ZxBQ
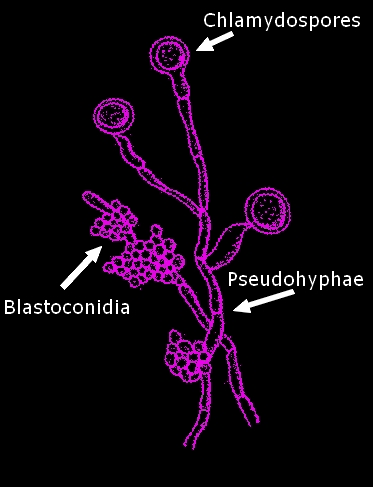
- KOH preparation is the easiest and most cost-effective method for diagnosing cutaneous congenital candidiasis, but its use is not sufficient in the absence of other supporting clinical evidence.
- Culture from an intact pustule, skin biopsy tissue, or desquamated skin can help to support the diagnosis.
- Microscopic examination of skin scrapings prepared with calcofluor white stain is a simple way of detecting yeasts and pseudohyphae of Candida albicans. C albicans binds nonspecifically to polysaccharides found in fungal cell walls and produces a distinct bright color in a pattern characteristic for the organism when viewed under a fluorescence microscope.
Candida albicans on Sabouraud-Dextrose Agar at 48 hours at 30C
Microscopic:
A smear made from colonies taken from Sabouraud-Dextrose Agar, or blood agar will appear as round to oval cells about 4 to 8 µm. Though the cell wall structure differs from that of gram positive bacteria, yeast cells retain the crystal-violet stain of the routine gram stain and therefore appear purple. The yeast cell divides by budding. On primary media (reduced nutritionally) the budding can create elongated cells which when lined up along the dividing plane, mimic the appearance of a hyphae however these inline individual cells are referred to as a pseudohyphae (false hyphae). Some true hyphae may also be formed.
Along side of the pseudohyphae, Candida albicans develops blastoconidia around the area of the ‘septa’ (division). These appear as smaller round ‘grape-like’ clusters.
Candida albicans retaining crystal violet stain from routine gram stain taken from SAB Agar
Below are a few photos of Candida albicans as seen in actual specimens;

Candida albicans in a vaginal swab seen in the form of a pseudohyphae and a few individual oval cells. (Gram Stain X1000)
When a greenish hyponychial fluid accumulates, material may be obtained by heating a pin and painlessly puncturing the intact overlying nail. The fluid release provides symptomatic relief to the patient, and fluid may demonstrate multiple yeast organisms when viewed using KOH preparation.
- Lim and Lim report on a new contrast stain, trypan blue, for rapid diagnosis of candidal dermatomycoses.
Histologic Findings
A skin biopsy specimen stained with a periodic acid-Schiff stain reveals nonseptated hyphae. The presence of nonseptated hyphae allows cutaneous candidiasis to be distinguished from tinea.
Of all the types of Candida, the electron microscope shows that C albicans is the most confluent in its adherence to the skin.
Medical Care
- Candidal vulvovaginitis: Topical antifungal agents including miconazole nitrate (Micatin, Monistat-Derm) or clotrimazole (Lotrimin, Mycelex) creams are curative. One-time oral therapy with fluconazole (150 mg) or itraconazole (600 mg) is effective and may be a more attractive alternative to some patients, but it is more costly.
- Candidal balanitis: Topical therapy is sufficient in most patients. Evaluate asymptomatic sexual partners and treat them if they are affected. If persistent lesions spread beyond the genitalia, consider the possibility of diabetes, and assess for the disease.
- Congenital candidosis: Topical preparations usually are effective. Some authors recommend the use of oral nystatin in conjunction with topical agents to lower the risk of systemic infection.
- Oropharyngeal candidiasis in the infant: Most patients can be treated with nystatin oral suspension. Treat for 10-14 days or until 48-72 hours after resolution of symptoms. Dosage for preterm infants is 0.5 mL (50,000 U) to each side of mouth 4 times/day; dosage for infants is 1 mL (100,000 U) to each side of the mouth 4 times/d.
- Candidosis of the nipple: Treat nipple candidosis for 2 weeks using an antifungal cream after each feeding. The baby must be treated simultaneously with nystatin swabbed on all 4 gum lines and in the oral cavity, along with a few ingested drops, for 2 weeks. Babies may have no symptoms of oropharyngeal candidiasis and still be reinfecting their mothers. Careful hygiene is also important. Frequent changing and washing of bras in boiling water (along with anything the baby puts in its mouth, eg, pacifiers) is necessary. Gentian violet is not used because it stains badly and may irritate the infant’s mouth. If candidosis of the nipple goes untreated, it may extend, and oral treatment for the mother may be necessary. Cultures often are not pure and usually are not helpful.
- Candidal diaper dermatitis: Treatment for candidal diaper dermatitis includes practical measures that reduce the amount of time the diaper area is exposed to hot and humid conditions. Air drying, frequent diaper changes, and generous use of baby powders and zinc oxide paste are adequate preventive measures. For topical therapy of candidal diaper dermatitis, nystatin, amphotericin B, miconazole, and clotrimazole are effective and almost equivalent in efficacy.
- Oral candidiasis in adults
- Treatment with a topical agent such as nystatin (1:100,000 U/mL, 5 mL oral rinse and swallow qid) or clotrimazole troches (10 mg 5 times/d) usually is effective. In most patients, extend the duration of antifungal therapy at least twice as long as the termination of clinical signs and symptoms of candidosis. Reserve oral fluconazole, 100 mg once daily for 2 weeks, for patients with more severe disease.
- With denture stomatitis, improved oral hygiene with removal of dentures at night, vigorous brushing to remove plaque, and disinfecting (swish and spit) with chlorhexidine gluconate (Peridex) usually is adequate treatment. Topical therapy with clotrimazole troches or nystatin may be used for lesions that do not respond to the above measures. For more resistant cases oral fluconazole, 100 mg/day for several weeks, in addition to the above measures, may prove effective.
- Intertrigo
- Treatment is targeted to keeping the skin dry, with the addition of topical nystatin powder, clotrimazole, or miconazole twice daily, often in conjunction with a midpotency corticosteroid. Patients with extensive infection may require the addition of fluconazole (100 mg PO qd for 1-2 wk) or itraconazole (100 mg PO qd for 1-2 wk). Many anecdotally based remedies exist for intertrigo that have been used in dermatology offices for years with success. The remedies have focused on both drying the moist inflamed area and treating the candidosis. The treatments are adjusted based on whether the inflammation is acute (wet and red), subacute (red +/- maceration), or chronic (red and dry)
- For acute intertrigo, Domeboro solution, Castellani paint, or vinegar/water (1 tbsp vinegar per qt room-temperature water) may be applied twice per day for 5-10 minutes for 3-5 days as needed. Dry the area with a hair dryer (no heat). Apply a shake lotion twice per day (mixture: 40 g USP talc, 40 g zinc oxide, 10 g glycerin; mix into slurry or milkshake consistency, add distilled water up to 120 mL, dispense in 180-mL [6 oz] bottle). Place a large bath towel under breasts or in pendulous areas twice per day. Castellani paint (carbol fuchsin) is messy, but nightly painting may help wheothing else does. Some patients respond well to triamcinolone-nystatin cream.
- For subacute intertrigo, benzoyl peroxide wash may be used to cleanse the area instead of application of vinegar or Castellani paint. A topical anticandidal cream of choice is applied twice per day, with or without a mild hydrocortisone cream (no refills for the latter).
- For chronic intertrigo, the zinc-talc shake lotion may be used once or twice daily, and the hydrocortisone cream/antifungal mixture may be applied at night. Local hyperhidrosis may be treated with antiperspirants (ie, Arrid Extra Dry Unscented, Dry Idea) on a long-term basis. These products, along with the more concentrated Drysol (aluminum chloride 20%), may sting macerated skin. Nystatin in talc (100,000 U/g or 15 g) may be applied twice per day for a few days, then tapered and replaced with unscented baby powder as a powder-approach alternative.
- Sundaram et alnoted that candidal intertrigo can be treated with filter paper soaked in Castellani paint.
- Paronychia: Treatment with topical agents usually is not effective but should be tried for chronic candidal paronychia. Drying solutions or antifungal solutions are used. Oral therapy with either itraconazole (pulse dosing with 200 mg bid for 1 wk of each of 3 consecutive mo) or terbinafine (250 mg qd for 3 mo) is recommended.
- Candidosis and HIV: Topical therapy with agents such as nystatin and clotrimazole require a minimum of 20-30 minutes of drug contact with the oral mucosa. Treatment with topical therapies may be effective in the early stages of HIV infection, and it becomes less effective with disease progression. Oral treatment with a 2-week course of antifungal therapy (itraconazole, fluconazole, ketoconazole) is indicated in more refractory cases. In patients who are significantly immunocompromised, maintenance therapy on an intermittent (alternate days to twice weekly dosing of ketoconazole 200 mg or fluconazole 100 mg) or continuous basis may be required to provide symptomatic relief. In general, the goal is the cessation of therapy once clinical symptoms have subsided, since prolonged therapy increases the likelihood of the development of drug-resistant organisms.
Medication Summary
The azoles are a group of synthetic antimycotic agents with a broad spectrum of activity. The primary drugs available include ketoconazole, miconazole, fluconazole, itraconazole, and econazole. The mechanism of action of azoles is blocking the synthesis of ergosterol, the primary sterol in the fungal cell membrane. The depletion of ergosterol alters the fluidity of the cell membrane and alters the action of the membrane-associated enzymes. This results in inhibition of replication and inhibition of the transformation of candidal yeast forms into hyphae, which is the invasive and pathogenic form of the parasite.
Nystatin and amphotericin are polyenes, which are active against some fungi but have little action on mammalian cells and no action on bacteria. They bind to cell membranes and interfere with permeability and transport functions. These antibiotics act as ionophores and causes leakage of cations.
Terbinafine is an allylamine that is fungicidal for a wide range of skin pathogens. It inhibits squalene epoxidase, which is involved in the synthesis of ergosterol from squalene in the fungal cell wall. The accumulation of squalene within the cell is toxic to the organism.
A case of chronic mucocutaneous candidosis that was cured with micafungin has been reported.
Voriconazole is another third-line treatment.
A stable nitric oxide (NO)–releasing nanoparticle (NO-np) system for treating cutaneous candidiasis has been proposed as a new treatment for extensive cutaneous candidiasis in burn patients.
Antifungal agents
Class Summary
Exert fungicidal effect by altering permeability of fungal cell membrane. Mechanism of action also may involve an alteration of RNA and DNA metabolism or an intracellular accumulation of peroxide toxic to the fungal cell.
Nystatin (Mycostatin)
Miconazole topical (Micatin, Monistat-Derm, Monistat)
Clotrimazole (Lotrimin, Mycelex, Gyne-Lotrimin)
Fluconazole (Diflucan)
Itraconazole (Sporanox)
Terbinafine (Lamisil)
References:
1. Williams MD, Sallee D, Robinson M. Diabetic ketoacidosis in toddler with a diaper rash. Am J Emerg Med. Sep 2008;26(7):834.e1-2. [Medline].
2. Lim CS, Lim SL. New contrast stain for the rapid diagnosis of dermatophytic and candidal dermatomycoses. Arch Dermatol. Sep 2008;144(9):1228-9. [Medline].
3. Pappas PG, Kauffman CA, Andes D, et al. Clinical practice guidelines for the management of candidiasis: 2009 update by the Infectious Diseases Society of America. Clin Infect Dis. Mar 1 2009;48(5):503-35. [Medline].
4. Li M, Chen Q, Shen Y, Liu W. Candida albicans phospholipomannan triggers inflammatory responses of human keratinocytes through Toll-like receptor 2. Exp Dermatol. Jul 2009;18(7):603-10. [Medline].
5. Ramos-E-Silva M, Lima CM, Schechtman RC, Trope BM, Carneiro S. Superficial mycoses in immunodepressed patients (AIDS). Clin Dermatol. Mar 4 2010;28(2):217-25. [Medline]. [Full Text].
6. Geddes ER, Polder K, Cutlan JE, Torres-Cabala CA, Hymes SR. Ulcerated plaque under a ruby ring in an immunosuppressed patient. Dermatol Online J. Aug 15 2010;16(8):4. [Medline].
7. Luo DQ, Yang W, Wu LC, Liu JH, Chen WN. Interdigital ulcer: an unusual presentation of Candida infection. Mycoses. May 25 2011;[Medline].
8. Raz-Pasteur A, Ullmann Y, Berdicevsky I. The pathogenesis of Candida infections in a human skin model: scanning electron microscope observations. ISRN Dermatol. 2011;2011:150642. [Medline]. [Full Text].
9. Macherla C, Sanchez DA, Ahmadi MS, et al. Nitric oxide releasing nanoparticles for treatment of Candida albicans burn infections. Front Microbiol. 2012;3:193. [Medline]. [Full Text].
|

