Management of patients with the syndrome of pituitary – Cushing . Obesity and metabolic syndrome in family practice doctor. The organization of follow-up and rehabilitation. Employment expertise.
Cushing’s Syndrome
Synonym: hypercortisolism
Cushing’s syndrome is caused by prolonged exposure to elevated levels of either endogenous or exogenous glucocorticoids. The degree of cortisol overproduction is very variable. When presentation is florid, diagnosis is usually straightforward.1 But the presentation may be subtle and the combination of non-specific clinical manifestations and variable cyclical biochemical parameters often makes the diagnosis difficult.
video
Causes of Cushing’s syndrome can be divided into 2 groups:
· ACTH-dependent disease: excessive ACTH from the pituitary (Cushing’s disease), ectopic ACTH-producing tumours or excess ACTH administration
· Non-ACTH-dependent: adrenal adenomas, adrenal carcinomas, excess glucocorticoid administration

Epidemiology
· Incidence of Cushing’s syndrome excluding those cases caused by steroid or ACTH administration ranges from 0.7 to 2.4 per million population per year. However new data suggest that Cushing’s syndrome is more common than previously thought.
· In obese patients with type 2 diabetes, especially those with poor blood glucose control and hypertension, the reported prevalence of Cushing’s syndrome is between 2% and 5%.
Risk factors
· Cushing’s syndrome due to an adrenal or pituitary tumour is more common in females (ratio 5:1).
· The peak incidence of Cushing’s syndrome caused by an adrenal or pituitary adenoma is between the ages of 25 and 40 years.
· Ectopic ACTH production due to lung cancer occurs later in life.
Common causes
Most common cause of Cushing’s syndrome is the use of exogenous glucocorticoids. Endogenous Cushing’s syndrome is divided into corticotropin-dependent and corticotropin-independent causes:
· Corticotropin-dependent causes account for about 80-85% of cases:
o 80% are due to pituitary adenomas (Cushing’s disease).
o The remaining 20% are due to ectopic corticotropin syndrome, which is usually due to small-cellcarcinoma
of the lung
and bronchial carcinoid tumours, but may occur with almost any endocrine tumour, e.g. phaeochromocytoma, pancreatic neuroendocrine tumours, medullary thyroid cancer, gut carcinoids.
· Corticotropin-independent Cushing’s syndrome:
o Is most often due to a unilateral tumour: adrenal adenoma in 60% and adrenal carcinoma in 40% of cases.
o Very rare adrenal causes of Cushing’s syndrome are corticotropin-dependent macronodularadrenal hyperplasia
, primary pigmented nodular adrenal disease and McCune-Albright syndrome.
Presentation
· Truncal obesity, supraclavicular fat pads, buffalo hump, weight gain
· Facial fullness, moon facies
· Proximal muscle wasting and weakness
· Diabetes or glucose intolerance
· Gonadal dysfunction
· Hypertension
· Skin: skin atrophy, purple striae, easy bruising, hirsutism, acne; pigmentation occurs with ACTH-dependent causes
· Psychological problems: depression, cognitive dysfunction, and emotional lability
· Osteopenia or osteoporosis
· Oedema
· Women may complain of irregular menses
· Thirst, polydipsia, polyuria
· Impaired immune function: increased infections, difficulty with wound healing
· Child: growth retardation
· Patients with an ACTH-producing pituitary tumour may develop headaches, visual problems, andgalactorrhoea
· Destruction of the anterior pituitary may cause hypothyroidism and amenorrhoea
Differential diagnosis
Pseudo-Cushing’s syndrome: all or some of the clinical features of Cushing’s syndrome, combined with biochemical evidence of hypercortisolism (but not caused by pituitary-adrenal axis problems). Causes include:
· Chronic severe anxiety and/or depression
· Prolonged excess alcohol consumption can cause a cushingoid appearance
· Obesity
· Poorly controlled diabetes
· HIV infection
Investigations
No single test is perfect and several different tests are usually needed.
· Investigations are usually carried out following referral; it is often easier to coordinate the investigations in secondary care and ensure earlier diagnosis and effective management.
· Investigations should be performed when there is no acute concurrent illness (e.g. infection or heart failure) as these can cause false-positive results.
· Full blood count: raised white cell count.
· Electrolytes and acid-base balance: hypokalemia (common with ectopic ACTH secretion as a result of mineralocorticoid activity), metabolic alkalosis.
· 24 hour urinary free cortisol:
o Ideally three collections. Measure creatinine excretion at the same time.
o Cushing’s syndrome can be confidently diagnosed if two or more collections measure cortisol excretion as more than three time the laboratory upper limit of normal.
o Need to repeat the test if creatinine excretion varies by more than 10% between collections.
o False positives may occur with pregnancy, anorexia, exercise, psychoses, alcohol andalcohol withdrawal. Strenuous exercise and illness raise cortisol secretion.
· Low dose dexamethasone suppression test:
o Useful screening test in those who are unable to reliably collect a 24 hour urine sample.
o 1 mg of dexamethasone is ingested at 11 pm, and serum cortisol is measured at 8 am the next morning.
o Mild Cushing’s syndrome is often difficult to distinguish from normal cortisol secretion or pseudo-Cushing’s syndrome, and both false-positive and false-negative test results occur.
· Midnight cortisol levels:
o Taken between 11 pm and 1 am. Demonstrate loss of normal diurnal variation of reduced cortisol production in the evening compared to the morning.
o Need to take blood from indwelling cannula with patient in a relaxed state.
o Inconvenient but reliable test for Cushing’s syndrome.
o Late-night salivary cortisol measurement is a simple and reliable screening test for Cushing’s syndrome.3
· Dexamethasone suppressed CRH test:
o Modification of the low dose dexamethasone suppression test.
o Intravenous CRH is given 2 hours after 48 hours (eight doses) of 0.5 mg dexamethasone. Serum cortisol is measured 15 minutes after ovine CRH administration.
o Very reliable test for Cushing’s syndrome.
· Plasma ACTH:
o Secretion is pulsatile and shows a diurnal variation, with the plasma concentrations highest at 8 a.m. and lowest at midnight. The secretion of ACTH is increased by stress.
o An undetectable plasma ACTH with an elevated serum cortisol level is diagnostic of ACTH-independent Cushing syndrome, which is due to a primary cortisol-producing adrenal adenoma or carcinoma, or exogenous glucocorticoid use.4 This should then be followed by an abdominal CT or MRI scan if exogenous glucocorticoids are excluded as the cause.
o An elevated ACTH level is consistent with ACTH-dependent Cushing’s syndrome.4
o If the plasma ACTH level is detectable then the following tests are indicated:
· High dose dexamethasone suppression test:
o The 8 mg overnight dexamethasone suppression test and the 48-hour high-dose dexamethasone test may be useful when baseline ACTH levels are equivocal. They also help in determining whether a patient has pituitary or ectopic ACTH production.
o Greater than 90% reduction in basal urinary free cortisol levels supports the diagnosis of a pituitary adenoma; ectopic ACTH causes lesser degrees of suppression.
· Inferior petrosal sinus sampling (IPS):
o Performed with CRH stimulation to aid in determining the source of excess ACTH.
o A baseline and stimulated ratio of IPS to peripheral ACTH of less than 1.8 is suggestive of ectopic ACTH, while a ratio of IPS to peripheral ACTH of greater than 2 is consistent with a pituitary adenoma.
· MRI of the pituitary.
· Chest and abdominal CT scans: for patients with suspected adrenal tumours or ectopic ACTH.
· Plasma CRH: ectopic CRH production is a very rare cause of Cushing’s syndrome.
Management
· The treatment of choice in most patients is surgical,5 but the metabolic consequences, including increased tissue fragility, poor wound healing, hypertension, and diabetes mellitus, increase the risks of surgery.6
· Drug therapy remains very important for normalising cortisol levels while awaiting the impact of more definitive treatment.7
· Cortisol hypersecretion must be controlled prior to surgery or radiotherapy if at all possible.
· Metyrapone, ketoconazole, and mitotane can all be used to lower cortisol by directly inhibiting synthesis and secretion in the adrenal gland.
· Metyrapone and ketoconazole are enzyme inhibitors and have rapid onset of action, but control of hypercortisolism is often lost with corticotropin oversecretion in Cushing’s disease. These drugs are not usually effective as long-term treatment and are used mainly for preparation for surgery or as adjunctive treatment after surgery or pituitary radiotherapy.
· Mitotane acts as an adrenolytic drug with delayed onset but long-lasting action, but control of corticotropin oversecretion in Cushing’s disease is maintained.
· Medical treatment can also be used in patients who are unwilling or unfit for surgery. Treatment can be used long term for patients with ectopic corticotropin secretion, but adrenalectomy may be preferred.
· Etomidate can be used for acute control of severe hypercortisolaemia.
Is the treatment of choice for the following conditions:
· Pituitary tumours: trans-sphenoidal microsurgery.8 Radiation therapy may be used as an adjunct for patients who are not cured.9 Bilateral adrenalectomy may be necessary to control toxic cortisol levels.
· Adrenocortical tumours: require surgical removal. Laparoscopic surgery is now the treatment of choice for unilateral adrenal adenomas.1
· Removal of neoplastic tissue is indicated for ectopic ACTH production. Metastatic spread makes a surgical cure unlikely or impossible. Bilateral adrenalectomy is indicated if necessary to control toxic cortisol levels.
· Persisting hypercortisolaemia after trans-sphenoidal surgery can be treated with pituitary radiotherapy.
· Conventional fractionated radiotherapy is very effective but is associated with long-termhypopituitarism and can be very delayed in effectiveness.
Complications
Patients with Cushing’s syndrome often develop:
· Metabolic syndrome
· Hypertension
· Impaired glucose tolerance and diabetes
· Obesity
· Hyperlipidaemia: raised LDL cholesterol and triglycerides
· Coagulopathy: thrombophilia
· Osteoporosis
· Perforated viscera
· Impaired immunity, including opportunistic fungal infections
· Nelson’s syndrome: may follow bilateral adrenalectomy for Cushing’s disease
· A primary pituitary tumour may cause pan-hypopituitarism and visual loss
Prognosis
· Patients with incompletely controlled Cushing’s syndrome have a five-fold excess mortality.1
· The most common causes of Cushing’s-associated mortality are hypertension, myocardial infarction, infection and heart failure.
· The usual course is chronic, with cyclic exacerbations and rare remissions.
· The prognosis is guardedly favorable with surgery.
· The rare adrenocortical carcinomas have a 5-year survival rate of 30% or less.
What is Cushing’s Syndrome? Cushing’s syndrome is an endocrine or hormonal disorder. It occurs when the adrenal glands release too much of the hormone cortisol into the body for long periods of time.
Cortisol is essential to many of the body’s cardiovascular and metabolic functions. But perhaps its most important job is to help the body respond to stress.
Normally the adrenal gland releases the exact amount necessary to meet our daily needs. However, sometimes the process goes wrong and an excess of cortisol is produced.
The malfunction may be caused by:
There is no single symptom shared by everyone with Cushing’s Syndrome, however, some symptoms occur more frequently than others.
Introduction
Cushing’s syndrome is a hormonal disorder caused by prolonged exposure of the body’s tissues to high levels of the hormone cortisol. Sometimes called “hypercortisolism,” it is relatively rare and most commonly affects adults aged 20 to 50. An estimated 10 to 15 of every million people are affected each year.
What Are the Symptoms?
Symptoms vary, but most people have upper body obesity, rounded face, increased fat around the neck, and thinning arms and legs. Children tend to be obese with slowed growth rates.
Other symptoms appear in the skin, which becomes fragile and thin. It bruises easily and heals poorly. Purplish pink stretch marks may appear on the abdomen, thighs, buttocks, arms and breasts. The bones are weakened, and routine activities such as bending, lifting or rising from a chair may lead to backaches, rib and spinal column fractures.
Most people have severe fatigue, weak muscles, high blood pressure and high blood sugar. Irritability, anxiety and depression are common.
Women usually have excess hair growth on their faces, necks, chests, abdomens, and thighs. Their menstrual periods may become irregular or stop. Men have decreased fertility with diminished or absent desire for sex.
What Causes Cushing’s Syndrome?
Cushing’s syndrome occurs when the body’s tissues are exposed to excessive levels of cortisol for long periods of time. Many people suffer the symptoms of Cushing’s syndrome because they take glucocorticoid hormones such as prednisone for asthma, rheumatoid arthritis, lupus and other inflammatory diseases, or for immunosuppression after transplantation.
Others develop Cushing’s syndrome because of overproduction of cortisol by the body. Normally, the production of cortisol follows a precise chain of events. First, the hypothalamus, a part of the brain which is about the size of a small sugar cube, sends corticotropin releasing hormone (CRH) to the pituitary gland. CRH causes the pituitary to secrete ACTH (adrenocorticotropin), a hormone that stimulates the adrenal glands. When the adrenals, which are located just above the kidneys, receive the ACTH, they respond by releasing cortisol into the bloodstream.
Cortisol performs vital tasks in the body. It helps maintain blood pressure and cardiovascular function, reduces the immune system’s inflammatory response, balances the effects of insulin in breaking down sugar for energy, and regulates the metabolism of proteins, carbohydrates, and fats. One of cortisol’s most important jobs is to help the body respond to stress. For this reason, women in their last 3 months of pregnancy and highly trained athletes normally have high levels of the hormone. People suffering from depression, alcoholism, malnutrition and panic disorders also have increased cortisol levels.
When the amount of cortisol in the blood is adequate, the hypothalamus and pituitary release less CRH and ACTH. This ensures that the amount of cortisol released by the adrenal glands is precisely balanced to meet the body’s daily needs. However, if something goes wrong with the adrenals or their regulating switches in the pituitary gland or the hypothalamus, cortisol production can go awry.
Pituitary Adenomas
Pituitary adenomas cause most cases of Cushing’s syndrome. They are benign, or non-cancerous, tumors of the pituitary gland which secrete increased amounts of ACTH. Most patients have a single adenoma. This form of the syndrome, known as “Cushing’s disease,” affects women five times more frequently than men.
Ectopic ACTH Syndrome
Some benign or malignant (cancerous) tumors that arise outside the pituitary can produce ACTH. This condition is known as ectopic ACTH syndrome. Lung tumors cause over 50 percent of these cases. Men are affected 3 times more frequently than women. The most common forms of ACTH-producing tumors are oat cell, or small cell lung cancer, which accounts for about 25 percent of all lung cancer cases, and carcinoid tumors. Other less common types of tumors that can produce ACTH are thymomas, pancreatic islet cell tumors, and medullary carcinomas of the thyroid.
Adrenal Tumors
Sometimes, an abnormality of the adrenal glands, most often an adrenal tumor, causes Cushing’s syndrome. The average age of onset is about 40 years. Most of these cases involve non-cancerous tumors of adrenal tissue, called adrenal adenomas, which release excess cortisol into the blood.
Adrenocortical carcinomas, or adrenal cancers, are the least common cause of Cushing’s syndrome. Cancer cells secrete excess levels of several adrenal cortical hormones, including cortisol and adrenal androgens. Adrenocortical carcinomas usually cause very high hormone levels and rapid development of symptoms.
Familial Cushing’s Syndrome
Most cases of Cushing’s syndrome are not inherited. Rarely, however, some individuals have special causes of Cushing’s syndrome due to an inherited tendency to develop tumors of one or more endocrine glands. In Primary Pigmented Micronodular Adrenal Disease, children or young adults develop small cortisol-producing tumors of the adrenal glands. In Multiple Endocrine Neoplasia Type I (MEN I), hormone secreting tumors of the parathyroid glands, pancreas and pituitary occur. Cushing’s syndrome in MEN I may be due to pituitary, ectopic or adrenal tumors.
How Is Cushing’s Syndrome Diagnosed?
Diagnosis is based on a review of the patient’s medical history, physical examination and laboratory tests. Often x-ray exams of the adrenal or pituitary glands are useful for locating tumors. These tests help to determine if excess levels of cortisol are present and why.
24-Hour UrinaryFree Cortisol Level
This is the most specific diagnostic test. The patient’s urine is collected over a 24-hour period and tested for the amount of cortisol. Levels higher than 50-100 micrograms a day for an adult suggest Cushing’s syndrome. The normal upper limit varies in different laboratories, depending on which measurement technique is used.
Once Cushing’s syndrome has been diagnosed, other tests are used to find the exact location of the abnormality that leads to excess cortisol production. The choice of test depends, in part, on the preference of the endocrinologist or the center where the test is performed.
Dexamethasone Suppression Test
This test helps to distinguish patients with excess production of ACTH due to pituitary adenomas from those with ectopic ACTH-producing tumors. Patients are given dexamethasone, a synthetic glucocorticoid, by mouth every 6 hours for 4 days. For the first 2 days, low doses of dexamethasone are given, and for the last 2 days, higher doses are given. Twenty-four hour urine collections are made before dexamethasone is administered and on each day of the test. Since cortisol and other glucocorticoids signal the pituitary to lower secretion of ACTH, the normal response after taking dexamethasone is a drop in blood and urine cortisol levels. Different responses of cortisol to dexamethasone are obtained depending on whether the cause of Cushing’s syndrome is a pituitary adenoma or an ectopic ACTH-producing tumor.
The dexamethasone suppression test can produce false-positive results in patients with depression, alcohol abuse, high estrogen levels, acute illness, and stress. Conversely, drugs such as phenytoin and phenobarbital may cause false-negative results in response to dexamethasone suppression. For this reason, patients are usually advised by their physicians to stop taking these drugs at least one week before the test.
CRH Stimulation Test
This test helps to distinguish between patients with pituitary adenomas and those with ectopic ACTH syndrome or cortisol-secreting adrenal tumors. Patients are given an injection of CRH, the corticotropin-releasing hormone which causes the pituitary to secrete ACTH. Patients with pituitary adenomas usually experience a rise in blood levels of ACTH and cortisol. This response is rarely seen in patients with ectopic ACTH syndrome and practically never in patients with cortisol-secreting adrenal tumors.
Direct Visualization of the Endocrine Glands (Radiologic Imaging)
Imaging tests reveal the size and shape of the pituitary and adrenal glands and help determine if a tumor is present. The most common are the CT (computerized tomography) scan and MRI (magnetic resonance imaging). A CT scan produces a series of x-ray pictures giving a cross-sectional image of a body part. MRI also produces images of the internal organs of the body but without exposing the patient to ionizing radiation.
Imaging procedures are used to find a tumor after a diagnosis has been established. Imaging is not used to make the diagnosis of Cushing’s syndrome because benign tumors, sometimes called “incidentalomas,” are commonly found in the pituitary and adrenal glands. These tumors do not produce hormones detrimental to health and are not removed unless blood tests show they are a cause of symptoms or they are unusually large. Conversely, pituitary tumors are not detected by imaging in almost 50 percent of patients who ultimately require pituitary surgery for Cushing’s syndrome.
Petrosal Sinus Sampling
This test is not always required, but in many cases, it is the best way to separate pituitary from ectopic causes of Cushing’s syndrome. Samples of blood are drawn from the petrosal sinuses, veins which drain the pituitary, by introducing catheters through a vein in the upper thigh/groin region, with local anesthesia and mild sedation. X-rays are used to confirm the correct position of the catheters. Often CRH, the hormone which causes the pituitary to secrete ACTH, is given during this test to improve diagnostic accuracy. Levels of ACTH in the petrosal sinuses are measured and compared with ACTH levels in a forearm vein. ACTH levels higher in the petrosal sinuses than in the forearm vein indicate the presence of a pituitary adenoma; similar levels suggest ectopic ACTH syndrome.
The Dexamethasone-CRH Test
Some individuals have high cortisol levels, but do not develop the progressive effects of Cushing’s syndrome, such as muscle weakness, fractures and thinning of the skin. These individuals may have Pseudo Cushing’s syndrome, which was originally described in people who were depressed or drank excess alcohol, but is now known to be more common. Pseudo Cushing’s does not have the same long-term effects on health as Cushing’s syndrome and does not require treatment directed at the endocrine glands. Although observation over months to years will distinguish Pseudo Cushing’s from Cushing’s, the dexamethasone-CRH test was developed to distinguish between the conditions rapidly, so that Cushing’s patients can receive prompt treatment. This test combines the dexamethasone suppression and the CRH stimulation tests. Elevations of cortisol during this test suggest Cushing’s syndrome.
Some patients may have sustained high cortisol levels without the effects of Cushing’s syndrome. These high cortisol levels may be compensating for the body’s resistance to cortisol’s effects. This rare syndrome of cortisol resistance is a genetic condition that causes hypertension and chronic androgen excess.
Sometimes other conditions may be associated with many of the symptoms of Cushing’s syndrome. These include polycystic ovarian syndrome, which may cause menstrual disturbances, weight gain from adolescence, excess hair growth and sometimes impaired insulin action and diabetes. Commonly, weight gain, high blood pressure and abnormal levels of cholesterol and triglycerides in the blood are associated with resistance to insulin action and diabetes; this has been described as the “Metabolic Syndrome-X.” Patients with these disorders do not have abnormally elevated cortisol levels.
How Is Cushing’s Syndrome Treated?
Treatment depends on the specific reason for cortisol excess and may include surgery, radiation, chemotherapy or the use of cortisol-inhibiting drugs. If the cause is long-term use of glucocorticoid hormones to treat another disorder, the doctor will gradually reduce the dosage to the lowest dose adequate for control of that disorder. Once control is established, the daily dose of glucocorticoid hormones may be doubled and given on alternate days to lessen side effects.
Pituitary Adenomas
Several therapies are available to treat the ACTH-secreting pituitary adenomas of Cushing’s disease. The most widely used treatment is surgical removal of the tumor, known as transsphenoidal adenomectomy. Using a special microscope and very fine instruments, the surgeon approaches the pituitary gland through a nostril or an opening made below the upper lip. Because this is an extremely delicate procedure, patients are often referred to centers specializing in this type of surgery. The success, or cure, rate of this procedure is over 80 percent when performed by a surgeon with extensive experience. If surgery fails, or only produces a temporary cure, surgery can be repeated, often with good results. After curative pituitary surgery, the production of ACTH drops two levels below normal. This is a natural, but temporary, drop in ACTH production, and patients are given a synthetic form of cortisol (such as hydrocortisone or prednisone). Most patients can stop this replacement therapy in less than a year.
For patients in whom transsphenoidal surgery has failed or who are not suitable candidates for surgery, radiotherapy is another possible treatment. Radiation to the pituitary gland is given over a 6-week period, with improvement occurring in 40 to 50 percent of adults and up to 80 percent of children. It may take several months or years before patients feel better from radiation treatment alone. However, the combination of radiation and the drug mitotane (Lysodren®) can help speed recovery. Mitotane suppresses cortisol production and lowers plasma and urine hormone levels. Treatment with mitotane alone can be successful in 30 to 40 percent of patients. Other drugs used alone or in combination to control the production of excess cortisol are aminoglutethimide, metyrapone, trilostane and ketoconazole. Each has its own side effects that doctors consider when prescribing therapy for individual patients.
Ectopic ACTH Syndrome
To cure the overproduction of cortisol caused by ectopic ACTH syndrome, it is necessary to eliminate all of the cancerous tissue that is secreting ACTH. The choice of cancer treatment–surgery, radiotherapy, chemotherapy, immunotherapy, or a combination of these treatments–depends on the type of cancer and how far it has spread. Since ACTH-secreting tumors (for example, small cell lung cancer) may be very small or widespread at the time of diagnosis, cortisol-inhibiting drugs, like mitotane, are an important part of treatment. In some cases, if pituitary surgery is not successful, surgical removal of the adrenal glands (bilateral adrenalectomy) may take the place of drug therapy.
Adrenal Tumors
Surgery is the mainstay of treatment for benign as well as cancerous tumors of the adrenal glands. In Primary Pigmented Micronodular Adrenal Disease and the familial Carney’s complex, surgical removal of the adrenal glands is required.
Cushing’s syndrome is a hormonal disorder caused by prolonged exposure of the body’s tissues to high levels of the hormone cortisol. Sometimes called hypercortisolism, Cushing’s syndrome is relatively rare and most commonly affects adults aged 20 to 50. People who are obese and have type 2 diabetes, along with poorly controlled blood glucose—also called blood sugar—and high blood pressure, have an increased risk of developing the disorder.
Signs and symptoms of Cushing’s syndrome vary, but most people with the disorder have upper body obesity, a rounded face, increased fat around the neck, and relatively slender arms and legs. Children tend to be obese with slowed growth rates.
Other signs appear in the skin, which becomes fragile and thin, bruises easily, and heals poorly. Purple or pink stretch marks may appear on the abdomen, thighs, buttocks, arms, and breasts. The bones are weakened, and routine activities such as bending, lifting, or rising from a chair may lead to backaches and rib or spinal column fractures.
Women with Cushing’s syndrome usually have excess hair growth on their face, neck, chest, abdomen, and thighs. Their menstrual periods may become irregular or stop. Men may have decreased fertility with diminished or absent desire for sex and, sometimes, erectile dysfunction.
Other common signs and symptoms include
Sometimes other conditions have many of the same signs as Cushing’s syndrome, even though people with these disorders do not have abnormally elevated cortisol levels. For example, polycystic ovary syndrome can cause menstrual disturbances, weight gain beginning in adolescence, excess hair growth, and impaired insulin action and diabetes. Metabolic syndrome—a combination of problems that includes excess weight around the waist, high blood pressure, abnormal levels of cholesterol and triglycerides in the blood, and insulin resistance—also mimics the symptoms of Cushing’s syndrome.
Cushing’s syndrome occurs when the body’s tissues are exposed to high levels of cortisol for too long. Many people develop Cushing’s syndrome because they take glucocorticoids—steroid hormones that are chemically similar to naturally produced cortisol—such as prednisone for asthma, rheumatoid arthritis, lupus, and other inflammatory diseases. Glucocorticoids are also used to suppress the immune system after transplantation to keep the body from rejecting the new organ or tissue.
Other people develop Cushing’s syndrome because their bodies produce too much cortisol. Normally, the production of cortisol follows a precise chain of events. First, the hypothalamus, a part of the brain about the size of a small sugar cube, sends corticotropin-releasing hormone (CRH) to the pituitary gland. CRH causes the pituitary to secrete adrenocorticotropin hormone (ACTH), which stimulates the adrenal glands. When the adrenals, which are located just above the kidneys, receive the ACTH, they respond by releasing cortisol into the bloodstream.
Cortisol performs vital tasks in the body including
The hypothalamus sends CRH to the pituitary, which responds by secreting ACTH. ACTH then causes the adrenals to release cortisol into the bloodstream.
One of cortisol’s most important jobs is to help the body respond to stress. For this reason, women in their last 3 months of pregnancy and highly trained athletes normally have high levels of the hormone. People suffering from depression, alcoholism, malnutrition, or panic disorders also have increased cortisol levels.
When the amount of cortisol in the blood is adequate, the hypothalamus and pituitary release less CRH and ACTH. This process ensures the amount of cortisol released by the adrenal glands is precisely balanced to meet the body’s daily needs. However, if something goes wrong with the adrenals or the regulating switches in the pituitary gland or hypothalamus, cortisol production can go awry.
Pituitary adenomas cause 70 percent of Cushing’s syndrome cases,1 excluding those caused by glucocorticoid use. These benign, or noncancerous, tumors of the pituitary gland secrete extra ACTH. Most people with the disorder have a single adenoma. This form of the syndrome, known as Cushing’s disease, affects women five times more often than men.
Some benign or, more often, cancerous tumors that arise outside the pituitary can produce ACTH. This condition is known as ectopic ACTH syndrome. Lung tumors cause more than half of these cases, and men are affected three times more often than women. The most common forms of ACTH-producing tumors are small cell lung cancer, which accounts for about 13 percent of all lung cancer cases,2 and carcinoid tumors—small, slow-growing tumors that arise from hormone-producing cells in various parts of the body. Other less common types of tumors that can produce ACTH are thymomas, pancreatic islet cell tumors, and medullary carcinomas of the thyroid.
In rare cases, an abnormality of the adrenal glands, most often an adrenal tumor, causes Cushing’s syndrome. Adrenal tumors are four to five times more common in women than men, and the average age of onset is about 40. Most of these cases involve noncancerous tumors of adrenal tissue called adrenal adenomas, which release excess cortisol into the blood.
Adrenocortical carcinomas—adrenal cancers—are the least common cause of Cushing’s syndrome. With adrenocortical carcinomas, cancer cells secrete excess levels of several adrenocortical hormones, including cortisol and adrenal androgens, a type of male hormone. Adrenocortical carcinomas usually cause very high hormone levels and rapid development of symptoms.
Most cases of Cushing’s syndrome are not inherited. Rarely, however, Cushing’s syndrome results from an inherited tendency to develop tumors of one or more endocrine glands. Endocrine glands release hormones into the bloodstream. With primary pigmented micronodular adrenal disease, children or young adults develop small cortisol-producing tumors of the adrenal glands. With multiple endocrine neoplasia type 1 (MEN1), hormone-secreting tumors of the parathyroid glands, pancreas, and pituitary develop; Cushing’s syndrome in MEN1 may be due to pituitary, ectopic, or adrenal tumors.
Diagnosis is based on a review of a person’s medical history, a physical examination, and laboratory tests. X rays of the adrenal or pituitary glands can be useful in locating tumors.
No single lab test is perfect and usually several are needed. The three most common tests used to diagnose Cushing’s syndrome are the 24-hour urinary free cortisol test, measurement of midnight plasma cortisol or late-night salivary cortisol, and the low-dose dexamethasone suppression test. Another test, the dexamethasone–corticotropin-releasing hormone test, may be needed to distinguish Cushing’s syndrome from other causes of excess cortisol.
· 24-hour urinary free cortisol level. In this test, a person’s urine is collected several times over a 24-hour period and tested for cortisol. Levels higher than 50 to 100 micrograms a day for an adult suggest Cushing’s syndrome. The normal upper limit varies in different laboratories, depending on which measurement technique is used.
· Midnight plasma cortisol and late-night salivary cortisol measurements. The midnight plasma cortisol test measures cortisol concentrations in the blood. Cortisol production is normally suppressed at night, but in Cushing’s syndrome, this suppression doesn’t occur. If the cortisol level is more than 50 nanomoles per liter (nmol/L), Cushing’s syndrome is suspected. The test generally requires a 48-hour hospital stay to avoid falsely elevated cortisol levels due to stress.
However, a late-night or bedtime saliva sample can be obtained at home, then tested to determine the cortisol level. Diagnostic ranges vary, depending on the measurement technique used.
· Low-dose dexamethasone suppression test (LDDST). In the LDDST, a person is given a low dose of dexamethasone, a synthetic glucocorticoid, by mouth every 6 hours for 2 days. Urine is collected before dexamethasone is administered and several times on each day of the test. A modified LDDST uses a onetime overnight dose.
Cortisol and other glucocorticoids signal the pituitary to release less ACTH, so the normal response after taking dexamethasone is a drop in blood and urine cortisol levels. If cortisol levels do not drop, Cushing’s syndrome is suspected.
The LDDST may not show a drop in cortisol levels in people with depression, alcoholism, high estrogen levels, acute illness, or stress, falsely indicating Cushing’s syndrome. On the other hand, drugs such as phenytoin and phenobarbital may cause cortisol levels to drop, falsely indicating that Cushing’s is not present in people who actually have the syndrome. For this reason, physicians usually advise their patients to stop taking these drugs at least 1 week before the test.
· Dexamethasone–corticotropin-releasing hormone (CRH) test. Some people have high cortisol levels but do not develop the progressive effects of Cushing’s syndrome, such as muscle weakness, fractures, and thinning of the skin. These people may have pseudo-Cushing’s syndrome, a condition sometimes found in people who have depression or anxiety disorders, drink excess alcohol, have poorly controlled diabetes, or are severely obese. Pseudo-Cushing’s does not have the same long-term effects on health as Cushing’s syndrome and does not require treatment directed at the endocrine glands.
The dexamethasone-CRH test rapidly distinguishes pseudo-Cushing’s from mild cases of Cushing’s. This test combines the LDDST and a CRH stimulation test. In the CRH stimulation test, an injection of CRH causes the pituitary to secrete ACTH. Pretreatment with dexamethasone prevents CRH from causing an increase in cortisol in people with pseudo-Cushing’s. Elevations of cortisol during this test suggest Cushing’s syndrome.
Once Cushing’s syndrome has been diagnosed, other tests are used to find the exact location of the abnormality that leads to excess cortisol production. The choice of test depends, in part, on the preference of the endocrinologist or the center where the test is performed.
· CRH stimulation test. The CRH test, without pretreatment with dexamethasone, helps separate people with pituitary adenomas from those with ectopic ACTH syndrome or adrenal tumors. As a result of the CRH injection, people with pituitary adenomas usually experience a rise in blood levels of ACTH and cortisol because CRH acts directly on the pituitary. This response is rarely seen in people with ectopic ACTH syndrome and practically never in those with adrenal tumors.
· high-dose dexamethasone suppression test (HDDST). The HDDST is the same as the LDDST, except it uses higher doses of dexamethasone. This test helps separate people with excess production of ACTH due to pituitary adenomas from those with ectopic ACTH-producing tumors. High doses of dexamethasone usually suppress cortisol levels in people with pituitary adenomas but not in those with ectopic ACTH-producing tumors.
· Radiologic imaging: direct visualization of the endocrine glands. Imaging tests reveal the size and shape of the pituitary and adrenal glands and help determine if a tumor is present. The most common imaging tests are the computerized tomography (CT) scan and magnetic resonance imaging (MRI). A CT scan produces a series of x-ray pictures giving a cross-sectional image of a body part. MRI also produces images of internal organs but without exposing patients to ionizing radiation.
Imaging procedures are used to find a tumor after a diagnosis has been made. Imaging is not used to make the diagnosis of Cushing’s syndrome because benign tumors are commonly found in the pituitary and adrenal glands. These tumors, sometimes called incidentalomas, do not produce hormones in quantities that are harmful. They are not removed unless blood tests show they are a cause of symptoms or they are unusually large. Conversely, pituitary tumors may not be detectable by imaging in almost half of people who ultimately need pituitary surgery for Cushing’s syndrome.
· Petrosal sinus sampling. This test is not always required, but in many cases, it is the best way to distinguish pituitary from ectopic causes of Cushing’s syndrome. Samples of blood are drawn from the petrosal sinuses—veins that drain the pituitary—by inserting tiny tubes through a vein in the upper thigh or groin region. A local anesthetic and mild sedation are given, and x rays are taken to confirm the correct position of the tubes. Often CRH, the hormone that causes the pituitary to release ACTH, is given during this test to improve diagnostic accuracy.
Levels of ACTH in the petrosal sinuses are measured and compared with ACTH levels in a forearm vein. Higher levels of ACTH in the sinuses than in the forearm vein indicate a pituitary adenoma. Similar levels of ACTH in the petrosal sinuses and the forearm suggest ectopic ACTH syndrome.
Treatment depends on the specific reason for excess cortisol and may include surgery, radiation, chemotherapy, or the use of cortisol-inhibiting drugs. If the cause is long-term use of glucocorticoid hormones to treat another disorder, the doctor will gradually reduce the dosage to the lowest dose adequate for control of that disorder. Once control is established, the daily dose of glucocorticoid hormones may be doubled and given on alternate days to lessen side effects. In some cases, noncorticosteroid drugs can be prescribed.
Several therapies are available to treat the ACTH-secreting pituitary adenomas of Cushing’s disease. The most widely used treatment is surgical removal of the tumor, known as transsphenoidal adenomectomy. Using a special microscope and fine instruments, the surgeon approaches the pituitary gland through a nostril or an opening made below the upper lip. Because this procedure is extremely delicate, patients are often referred to centers specializing in this type of surgery. The success, or cure, rate of this procedure is more than 80 percent when performed by a surgeon with extensive experience. If surgery fails or only produces a temporary cure, surgery can be repeated, often with good results.
After curative pituitary surgery, the production of ACTH drops two levels below normal. This drop is natural and temporary, and patients are given a synthetic form of cortisol such as hydrocortisone or prednisone to compensate. Most people can stop this replacement therapy in less than 1 or 2 years, but some must be on it for life.
If transsphenoidal surgery fails or a patient is not a suitable candidate for surgery, radiation therapy is another possible treatment. Radiation to the pituitary gland is given over a 6-week period, with improvement occurring in 40 to 50 percent of adults and up to 85 percent of children. Another technique, called stereotactic radiosurgery or gamma knife radiation, can be given in a single high-dose treatment. It may take several months or years before people feel better from radiation treatment alone. Combining radiation with cortisol-inhibiting drugs can help speed recovery.
Drugs used alone or in combination to control the production of excess cortisol are ketoconazole, mitotane, aminoglutethimide, and metyrapone. Each drug has its own side effects that doctors consider when prescribing medical therapy for individual patients.
To cure the overproduction of cortisol caused by ectopic ACTH syndrome, all of the cancerous tissue that is secreting ACTH must be eliminated. The choice of cancer treatment—surgery, radiation, chemotherapy, immunotherapy, or a combination of these treatments—depends on the type of cancer and how far it has spread. Because ACTH-secreting tumors may be small or widespread at the time of diagnosis, making them difficult to locate and treat directly, cortisol-inhibiting drugs are an important part of treatment. In some cases, if other treatments fail, surgical removal of the adrenal glands, called bilateral adrenalectomy, may replace drug therapy.
Surgery is the mainstay of treatment for benign and cancerous tumors of the adrenal glands. Primary pigmented micronodular adrenal disease and the inherited Carney complex—primary tumors of the heart that can lead to endocrine overactivity and Cushing’s syndrome—require surgical removal of the adrenal glands.
· Cushing’s syndrome is a disorder caused by prolonged exposure of the body’s tissues to high levels of the hormone cortisol.
· Typical signs and symptoms of Cushing’s syndrome include upper body obesity, a rounded face, skin that bruises easily and heals poorly, weakened bones, excess body hair growth and menstrual irregularities in women, and decreased fertility in men.
· Cushing’s syndrome is caused by exposure to glucocorticoids, which are used to treat inflammatory diseases, or by the body’s overproduction of cortisol, most often due to tumors of the pituitary gland or lung.
· Several tests are usually needed to diagnosis Cushing’s syndrome, including urine, blood, and saliva tests. Other tests help find the cause of the syndrome.
· Treatment depends on the specific reason for excess cortisol and may include surgery, radiation, chemotherapy, or the use of cortisol-inhibiting drugs.
A screening evaluation for the possibility of Cushing’s syndrome should be considered in any patient with signs and symptoms of excessive cortisol secretion. Abnormal weight gain, particularly in the central location accompanied by hypertension, diabetes, or hyperlipidemia should always signal the possibility of Cushing’s syndrome. Many patients with this disorder will also have facial rounding with the so-called “moon facies.” Accumulation of fat above the clavicles or behind the neck are also common features of excessive cortisol secretion. Some patients will also present with osteoporosis (particularly rib fractures) and some have muscle weakness. The presence of wide purplish striae (stretch marks) in the abdomen or elsewhere can also be a symptom of Cushing’s syndrome. The majority of patients with Cushing’s syndrome have some type of neuropsychiatric problem (particularly depression) or even some cognitive impairment. Fatigue is almost always present in patients with Cushing’s. In addition, women with the polycystic ovary syndrome should also all be screened for the possibility of Cushing’s syndrome.
The most appropriate diagnostic approach to patients with suspected Cushing’s syndrome is somewhat controversial; however, four diagnostic studies are currently used: late-night salivary cortisol, 24 hour urine free cortisol, low-dose dexamethasone suppression, and the dexamethasone-CRH test. These are summarized in Figure 1. (Print Figure 1 and bring to your doctor.)
Late-Night Salivary Cortisol
Late-night salivary cortisol is emerging as the most sensitive diagnostic test for Cushing’s syndrome. Elevated cortisol between 11:00 p.m. and midnight appears to be the earliest detectable abnormality in patients with this disorder. Cortisol secretion is usually very low at this time of the day, but in patients with Cushing’s syndrome, the value is virtually always elevated. Although this is a relatively new test, it is currently the most widely studied single test for the diagnosis of Cushing’s syndrome with at least eight independent studies from all over the world demonstrating sensitivity of 93-100% for the diagnosis of Cushing’s syndrome. In the United States, there is only one FDA-approved assay for the measurement of salivary cortisol in the diagnosis of Cushing’s syndrome. Collection of saliva requires special sampling tubes; however, this is a very easy test for patients to perform and can be done on multiple occasions. Salivary cortisol is very stable at room temperature and the samples can actually be mailed to a reference laboratory. Normal levels of late-night salivary cortisol virtually exclude the diagnosis of Cushing’s syndrome.
Urine Free Cortisol
24 hour urine free cortisol has, until recently, been considered the gold standard for the diagnosis of cortisol excess. A 24 hour urine free cortisol level does reflect the cortisol secretion throughout an entire day. Although the majority of patients with Cushing’s have elevated levels of urine free cortisol, it is becoming increasingly evident that many patients with mild Cushing’s syndrome will actually have normal levels of urine free cortisol. In other words, a normal 24 hour urine free cortisol does not exclude the diagnosis of Cushing’s syndrome and additional testing is always needed. In addition, there are many conditions which may increase urine free cortisol that are not Cushing’s syndrome, specifically depression, chronic alcoholism, and eating disorders.
Low-Dose Dexamethasone Suppression Testing
The low-dose dexamethasone suppression testing has been used for four decades as a diagnostic tool in the evaluation of patients with suspected Cushing’s syndrome. Dexamethasone is a synthetic steroid that should suppress the cortisol production iormal subjects to a very low level. Currently, the most widely used test is the administration of a small dose of dexamethasone (1 mg) at 11:00 p.m. followed by a measurement of serum cortisol early the following morning. It is now clear that normal subjects should suppress their cortisol level to a very low level (<1.8 mg/dl). This test using this strict criterion will provide approximately 95-97% sensitivity in the diagnosis of Cushing’s syndrome; however, some patients with mild Cushing’s syndrome will suppress their serum cortisol to levels even lower than this. This test is still widely employed and certainly can be useful in combination with the other tests previously mentioned.
Dexamethasone CRH Test
In patients with equivocal results, combination of dexamethasone suppression in combination with a stimulation test using a hormone called CRH can be useful in making the diagnosis of Cushing’s syndrome. CRH is a hypothalamic hormone which normally stimulates ACTH from the pituitary and subsequently cortisol from the adrenal gland. This study should only be performed in a setting where there are endocrinologists who have had experience with the test and ensure it is performed properly.
Once the diagnosis of Cushing’s syndrome has been established, its cause must be identified. The majority of patients with Cushing’s syndrome have an ACTH-secreting tumor usually from the pituitary gland (Cushing’s disease) or a non-pituitary tumor (ectopic ACTH syndrome). Some patients with Cushing’s syndrome may have a tumor in their adrenal glands secreting excessive cortisol or occasionally may have nodules in both adrenal glands that are hypersecreting.
ACTH Levels
The first step in distinguishing the type of Cushing’s syndrome is the measurement of ACTH. Patients with ACTH-secreting tumors will either have a normal or elevated level of ACTH. In contrast, patients with adrenal Cushing’s will have a subnormal level.
MRI Pituitary – Inferior Petrosal Sinus Sampling
Distinguishing a pituitary from a non-pituitary ACTH-secreting tumor may be a diagnostic challenge. Since the majority of patients with ACTH-secreting tumors have a pituitary lesion (often very small), a MRI of the pituitary gland with gadolinium enhancement is always the initial approach. When an unequivocal pituitary tumor (>5 mm) is identified with MRI, further diagnostic evaluation may not be needed depending on the clinical presentation. In such a case, referral to a skilled pituitary neurosurgeon may be recommended; however, it should be noted that at least 10% of the population have incidental tumors in the pituitary gland demonstrated on MRI. This means that at least 10-15% of patients with the ectopic ACTH syndrome also have an abnormal MRI of the pituitary gland.
In patients in whom the diagnosis is not certain based on pituitary imaging, the single best test to confirm the presence or absence of an ACTH-secreting pituitary tumor is a procedure called inferior petrosal sinus sampling. This procedure requires a skilled invasive radiologist who can sample blood from the veins (inferior petrosal sinuses) that drain the pituitary. ACTH as well as other pituitary hormones reach the systemic circulation through veins called the inferior petrosal sinuses. A catheter can be placed in both of these veins at the same time and blood sampled for ACTH before and after the administration of CRH (which stimulates ACTH) and at 2, 5, and 10 minutes. This invasive study should be performed at a center with extensive experience in the procedure and has a diagnostic accuracy of 95-98%.
High-Dose Dexamethasone Suppression Testing
Endocrinologists continue to perform high-dose dexamethasone suppression testing to distinguish a pituitary from a non-pituitary ACTH-secreting tumor. Unfortunately, this test is not helpful in this regard and should be abandoned.
Computed Tomography of the Adrenal Glands
In patients who do not have an ACTH-secreting tumor and thereby low ACTH levels, the problem usually resides within the adrenal gland. CT scanning of the adrenal glands will be helpful in identifying whether this represents a solitary cortisol-producing tumor from the adrenal gland or whether there are large nodules in each adrenal gland resulting in cortisol excess.
An association between certain metabolic disorders and cardiovascular disease has been known since the 1940s. In the 1980s this association became more clearly defined and the term metabolic syndrome (also known as syndrome X or the dysmetabolic syndrome) was coined to designate a cluster of metabolic risk factors that come together in a single individual. In more current times, the term metabolic syndrome is found throughout medical literature and in the lay press as well. There are slight differences in the criteria of diagnosis – depending on which authority is quoted. Regardless, the concept of a clustering of risks factors leading tocardiovascular disease is well accepted.
The main features of metabolic syndrome include insulin resistance, hypertension (high blood pressure),cholesterol abnormalities, and an increased risk for clotting. Patients are most often overweight or obese.
Insulin resistance refers to the diminished ability of cells to respond to the action of insulin in promoting the transport of the sugar glucose, from blood into muscles and other tissues. Because of the central role that insulin resistance plays in the metabolic syndrome, a separate article is devoted to insulin resistance.
The definition of metabolic syndrome depends on which group of experts is doing the defining. Based on the guidelines from the 2001 National Cholesterol Education Program Adult Treatment Panel (ATP III), any three of the following traits in the same individual meet the criteria for the metabolic syndrome:
1. Abdominal obesity: a waist circumference over 102 cm (40 in) in men and over 88 cm (35 inches) in women.
2. Serum triglycerides 150 mg/dl or above.
3. HDL cholesterol 40mg/dl or lower in men and 50mg/dl or lower in women.
4. Blood pressure of 130/85 or more.
5. Fasting blood glucose of 110 mg/dl or above. (Some groups say 100mg/dl)
The World Health Organization (WHO) has slightly different criteria for the metabolic syndrome:
1. High insulin levels, an elevated fasting blood glucose or an elevated post meal glucose alone with at least 2 of the following criteria:
2. Abdominal obesity as defined by a waist to hip ratio of greater than 0.9, abody mass index of at least 30 kg/m2 or a waist measurement over 37 inches.
3. Cholesterol panel showing a triglyceride level of at least 150 mg/dl or an HDL cholesterol lower than 35 mg/dl.
4. Blood pressure of 140/90 or above (or on treatment for high blood pressure).
Metabolic syndrome is quite common. Approximately 20%-30% of the population in industrialized countries have metabolic syndrome. By the year 2010, the metabolic syndrome is expected to affect 50-75 million people in the US alone.
As is true with many medical conditions, genetics and the environment both play important roles in the development of the metabolic syndrome.
Genetic factors influence each individual component of the syndrome, and the syndrome itself. A family history that includes type 2 diabetes, hypertension, and early heart disease greatly increases the chance that an individual will develop the metabolic syndrome.
Environmental issues such as low activity level, sedentary lifestyle, and progressiveweight gain also contribute significantly to the risk of developing the metabolic syndrome.
Metabolic syndrome is present in about 5% of people with normal body weight, 22% of those who are overweight and 60% of those considered obese. Adults who continue to gain five or more pounds per year raise their risk of developing metabolic syndrome by up to 45%.
While obesity itself is likely the greatest risk factor, others factors of concern include:
· women who are post-menopausal,
· smoking,
· eating an excessively high carbohydrate diet,
· lack of activity (even without weight change), and
· consuming an alcohol-free diet.
Metabolic syndrome is worth caring about because it is a condition that can pave the way to both diabetes and heart disease, two of the most common and important chronic diseases today.
Metabolic syndrome increases the risk of type 2 diabetes (the common type of diabetes) anywhere from 9-30 times over the normal population. That’s a huge increase. As to the risk of heart disease, studies vary, but the metabolic syndrome appears to increase the risk 2-4 times that of the normal population.
There are other concerns as well that should be mentioned. Metabolic syndrome is associated with fat accumulation in the liver (fatty liver), resulting in inflammation and the potential for cirrhosis. The kidneys can also be affected, as there is an association with microalbuminuria — the leaking of protein into the urine, a subtle but clear indication of kidney damage.
Other problems associated with metabolic syndrome include obstructive sleep apnea, polycystic ovary syndrome , increased risk of dementia with aging, and cognitive decline in the elderly.
The major goals are to treat both the underlying cause of the syndrome, and also to treat the cardiovascular risk factors if they persist. As has been discussed, the majority of people with metabolic syndrome are overweight and lead a sedentary lifestyle.
Lifestyle modification is the preferred treatment of metabolic syndrome. Weight reduction usually requires a specifically tailored multifaceted program that includes diet and exercise. Sometimes medications may be useful.
Diet
A detailed discussion of diet therapies, pros and cons of various diets etc. is beyond the scope of this article. However, there is now a trend toward the use of aMediterranean diet — one that is rich in “good” fats (olive oil) and contains a reasonable amount of carbohydrates and proteins (such as from fish and chicken).
The Mediterranean diet is palatable and easily sustained. In addition, recent studies have shown that when compared to a low fat diet, people on the Mediterranean diet have a greater decrease in body weight, and also had greater improvements in blood pressure, cholesterol levels, and other markers of heart disease — all of which are important in evaluating and treating metabolic syndrome.
Exercise
A sustainable exercise program, fore example 30 minutes five days a week is reasonable to start, providing there is no medical contraindication. (If you have any special concerns in this regard, check with your doctor first.) There is a beneficial effect of exercise on blood pressure, cholesterol levels, and insulin sensitivity, regardless of whether weight loss is achieved or not. Thus, exercise in itself is a helpful tool in treating metabolic syndrome.
Cosmetic surgery to remove fat
Some people may ask: Why not just have liposuction of the abdomen and remove the large amount abdominal fat, which is a big part of the problem? Data thus far shows no benefit in liposuction on insulin sensitivity, blood pressure, or cholesterol. As the saying goes, “If it’s too good to be true, it probably is.” Diet and exercise are still the preferred primary treatment of metabolic syndrome.
What if lifestyle changes are not enough to treat metabolic syndrome?
What if changes in lifestyle do not do the trick, what then? Drugs to control cholesterol levels, lipids, and high blood pressure may be considered.
If someone has already had a heart attack, their LDL (“bad”) cholesterol should be reduced below 100mg/dl. (Some experts now say it should be under 70mg/dl.) A person who has diabetes has a heart attack risk equivalent to that of someone who has already one and so should be treated in the same way. What remains controversial is whether metabolic syndrome should be considered a coronary equivalent or not. If you have metabolic syndrome, a detailed discussion about lipid therapy is needed between you and your doctor, as each individual is unique.
Blood pressure goals are generally set lower than 130/80. Some blood pressure medications offer more than simply lowering blood pressure. For example, a class of blood pressure drugs called ACE inhibitors has been found to also reduce the levels of insulin resistance and actually deter the development of type 2 diabetes. This is an important consideration when discussing the choice blood pressure drugs in the metabolic syndrome.
The discovery that a drug prescribed for one condition, and has other beneficial effects is not new. Drugs used to treat high blood sugar and insulin resistance may have beneficial effects on blood pressure and cholesterol profiles. A class of drugs called thiazolidinediones (pioglitazone [Actos] and rosiglitazone [Avandia]) also reduce the thickness of the walls of the carotid arteries; although restrictions have been placed by the US FDA on the use of rosiglitazone (Avandia) due to a reported increase in heart attack and other cardiovascular events in patients taking this drug.
Metformin (Glucophage), usually used to treat type 2 diabetes, also has been found to help prevent the onset of diabetes in people with metabolic syndrome. Indeed, in my practice, I routinely discuss metformin with my patients who have metabolic syndrome. Many of my patients who have insulin resistance associated with metabolic syndrome opt for metformin therapy. However, there are currently no established guidelines on treating metabolic syndrome patients with metformin if they do not have overt diabetes.
The term “metabolic syndrome” is a way of identifying individuals at high risk for the development of heart disease and diabetes. Intuitively we all know that obesity, high cholesterol, and hypertension are bad omens. We also know that insulin resistance precedes type 2 diabetes, and can itself be an important condition meriting treatment. Everyone reading this article knows someone who is overweight, hypertensive, or has cholesterol levels that are “a little high.” It may be a brother, sister, parent, neighbor, or even yourself.
For the physician, while the actual definition of “metabolic syndrome” may vary, the known clustering that occurs means that adults with any major cardiovascular risk should be evaluated for the presence of other risk factors. Patients at risk should receive education and counseling on lifestyle modification, and all risk factors for heart disease should be treated aggressively.
For the patient, the main point to understand is that it is important to treat the risk factors as bad things, before worse things happen. And while these changes can be addressed at a doctor’s office, the other 99.999% of the time, they need to be addressed in the real world. We need to start having healthier food options readily available. We need to have time during the day to take a walk.
The final take home message is:
· Find a walk buddy.
· Take a walk during your work break, even if it is just around the building.
· Go to a health food store.
· Evaluate what you feed your kids.
· Urge children to go outside and play.
It all adds up. Preventing metabolic syndrome really means having a healthy lifestyle.
video
Obesity is a major public health problem that is becoming more common among adults and increasing rapidly in children and adolescents. Obesity has been linked to a broad range of physical, emotional and socioeconomic problems. Importantly, in some people excess body fat causes an increased risk for vascular disease, including heart disease and stroke. Increased fat stored in intra-abdominal deposits is associated with, and may cause, an increase in risk factors for atherosclerotic cardiovascular disease (ASCVD).
There are a number of well established factors that when present increase an individual’s risk for atherosclerosis involving the blood vessels to the heart and other vital organs. These risk factors include: Hypertension, elevated levels of cholesterol, particularly LDL-cholesterol, in the blood, diabetes and hyperglycemia, and cigarette smoking. Another important risk factor is a family history of heart disease. To these 5 first order risk factors have been added a number of newer measures that may explain a tendency to get heart disease. High levels of triglyceride and low levels of HDL-cholesterol are a combination that can have as bad an effect on blood vessels as elevated cholesterol. Markers of inflammation such as C-reactive protein and tumor necrosis factor also seem to be linked with increased occurrence of ASCVD. Finally, increased levels of proteins involved in blood clotting such as fibrinogen and PAI may play a role in promoting atherosclerosis.
It has long been known that cardiovascular risk factors are not distributed randomly among members in a population but seem to cluster together in the same individuals. That is to say, people at risk to get diabetes are also more likely to have problems with high blood pressure and abnormalities in their blood triglyceride and cholesterol levels. Similarly, individuals with hypertension are more likely to develop impaired glucose tolerance, a type of pre-diabetes. This clustering, or development of several risk factors at once, leads to a greatly increased risk for ASCVD. At the other end of the spectrum, there are many individuals who never develop any risk factors for ASCVD. The designation of Metabolic Syndrome recognizes the fact that risk factors cluster and the diagnosis is based on the presence of specific abnormalities predisposing to cardiovascular disease. There are currently two sets of criteria for Metabolic Syndrome, one put forth by the World Health Organization (WHO) and the other by the National Institutes of Health (NIH). These working definitions are similar and include some element of abnormalities in glucose/insulin, blood pressure and lipids, and obesity. In general a person who is classified with Metabolic Syndrome by the WHO criteria is also diagnosed using the NIH criteria. The fact that two sets of standards exist indicates that the understanding and use of the term Metabolic Syndrome is new and evolving.
The clustering of risk factors in some individuals and complete sparing in others suggests that a common abnormality is involved in causing these problems. In fact, it is generally agreed on that increased body weight and particularly central obesity is at the core of Metabolic Syndrome. It has been known for many years that body fat tends to be distributed in different patterns. That is, some people tend to store a larger amount of fat in their hips and buttocks, while others have more of their body fat in their abdomen. These patterns have in the past been termed gynoid and android obesity because of the general tendency of women to have more fat in peripheral sites (hips and buttocks) and men to store fat centrally (in their abdomen). Interestingly, some of the distribution of body fat seems to be driven by sex hormones since men who make low levels of testosterone often have a gynoid distribution of body fat, and women tend to shift to a more android pattern after menopause when their estrogen levels decline. However, it is clear that the distribution of body fat is much more complex than the rules of gender since the patterns of body fat distribution overlap considerably among men and women.
Central, or abdominal, fat is more metabolically active than peripheral fat. This is to say that rates of fat storage and fat release are greater in central fat deposits than fat collections in the hips. On the one hand central fat is the site that decreases first when people embark on physical training sufficient to lose weight. On the other hand, in societies where food consumption is high and people are sedentary, central obesity seems to be a prominent problem. Interestingly, the weight gain or change in body composition that is commonly seen as people age often involves a relative increase in central fat stores.
It is now established that obesity is associated with the various components of Metabolic Syndrome and that central obesity is even more predictive than total body weight of a predisposition to ASCVD. Obesity, especially central obesity, causes insulin resistance, a decrease of the typical responses of tissues to the hormone insulin. Insulin resistance is primarily measured as the ability of insulin to decrease blood glucose levels because this is one of the primary actions of insulin. Since the normal response to decreased insulin action is to secrete more insulin, people with insulin resistance often times have higher thaormal insulin levels; this is termed hyperinsulinemia. Insulin resistance is probably the most common feature of Metabolic Syndrome and may be the link that causes the other factors to cluster together. For example, it has been proposed that hyperinsulinemia causes increased triglyceride production by the liver and salt retention by the kidney, effects that could lead to increases in circulating lipids and blood pressure.
There are two points about hyperinsulinemia that are important for understanding the diagnosis and treatment of Metabolic Syndrome. First, insulin levels in the blood vary considerably between different people and within a given individual throughout the day. Thus, there are no clear standards to use in clinical practice that absolutely define a high from an appropriate insulin level in a given person. Second, insulin resistance and hyperinsulinemia are intermediary features of Metabolic Syndrome- more markers than root cause. Central obesity causes insulin resistance, and while hyperinsulinemia may bring out other features of Metabolic Syndrome, lowering blood insulin levels alone is not a useful treatment approach (and in fact would cause high blood glucose levels or diabetes).
The causative link between central body fat and insulin resistance has not been proven. However, a number of possibilities to explain this connection are now under study including: increased levels of fatty acids in the blood, fat derived hormones andcytokines, and abnormalities in the brain’s interpretation and coordination of metabolic cues.
One of the most important consequences of insulin resistance is the development of diabetes. Normally blood glucose is controlled in a tight range through a balance of insulin secretion and insulin sensitivity. In persons who are very sensitive to insulin (generally lean, young and physically fit people) the amount of insulin that must be secreted to keep blood glucose controlled is low. Conversely in persons who are relatively insensitive to the action of insulin (generally heavy, older, inactive people) more insulin must be secreted to overcome resistance and maintaiormal blood glucose. As long as the pancreas can produce sufficient insulin even very insulin resistant individuals will maintaiormal blood glucose levels. However, defects in insulin secretion are fairly common in the population and tend to develop as people age. The combination of suboptimal insulin release with insulin resistance is the major cause of impaired glucose intolerance or type 2 diabetes. Diabetic patients also very frequently fit the classification of Metabolic Syndrome, a fact best explained by the key role of insulin resistance in both diagnoses. The clustering of risk factors in persons with diabetes accounts for why they have 2-4 times the risk of ASCVD as most nondiabetic persons. However, many persons without diabetes also fit the criteria for Metabolic Syndrome, and the clustered risk factors in these people identifies them as high risk for heart disease and related problems. This is the primary value of defining Metabolic Syndrome as a clinical entity.
Heart disease and other components of ASCVD like stroke, remain the major cause of death in the United States. In the last 10-20 years advances in treatment of cardiac risk factors have been shown to prevent clinical events. For example, effective treatment of hypertension or elevations in blood cholesterol or triglycerides decreases the incidence of myocardial infarction(heart attacks) and death. Furthermore rigorous treatment of diabetes also decreases vascular complications. These findings have coalesced into the clinical practice of preventive cardiology, which is the strategy of trying to prevent heart disease by minimizing or correcting risk factors.
Current estimates are that approximately 25% of American adults, and an increasing percentage of children and adolescents, can be classified as having Metabolic Syndrome. The wide prevalence of Metabolic Syndrome makes this condition a major contributor to cardiovascular risk. First and foremost these individuals are best served by identifying and trying to minimize risk factors. Thus, elevations in blood pressure should be detected, treated and monitored. Blood levels of cholesterol and triglyceride should be determined and diet and medications instituted if they are high. Blood glucose should be measured after a 10-12 hour fast (usually overnight) to detect diabetes or suggestions of glucose intolerance. These patients should receive special encouragement to stop smoking if they do so, and a clear warning not to start if they do not smoke.
Probably the single most effective approach to the abnormalities comprising Metabolic Syndrome is weight loss. A decrease of about 10% of body weight is often sufficient to have a major impact on blood pressure, plasma lipids and glucose, insulin resistance and the other abnormalities of Metabolic Syndrome. However, losing weight is very challenging for most people in our society and none of the currently available approaches- diet, exercise, or medications- are effective for the long term maintenance of weight loss. Some combination of caloric restriction and exercise should be suggested for most patients with Metabolic Syndrome, but given the limited response in most patients, should not replace treatment of specific risk factors.
The metabolic syndrome is not a disease. Rather, it is a group of risk factors that predisposes a patient to coronary heart disease, stroke, and renal and peripheral vascular disease as well as type 2 diabetes. Patients who have these factors also have increased mortality from all causes. These factors, according to the National Cholesterol Education Program – Adult Treatment Panel III (NCEP-ATP III), include:
(At least two other institutions have attempted to define the metabolic syndrome: the World Health Organization and the European Group for the Study of Insulin Resistance. The most widely used definition by NCEP-ATP III is adopted here.)
o Central obesity (also called abdominal obesity)
The hallmark of central obesity is excessive deposit of fat in and around the abdomen. The index of central obesity is the waist circumference, measured midway between the lowest point of the costal margin and the highest point of the iliac crest. It is not the circumference at the level of the umbilicus, nor is it the belt size in men and the narrowest waistline in women. Chinese men and women have central obesity if their waist circumference is > 90 cm and > 80 cm respectively. (The equivalent limits in Japanese men and women are > 85 cm and > 90 cm respectively; in Caucasian males and females, they are > 102 cm and > 88 cm respectively.)
o Dyslipidemia
Both a high fasting plasma triglyceride concentration and a low fasting plasma high density lipoprotein- (HDL-) cholesterol concentration are risk factors of the metabolic syndrome. For triglycerides, a fasting plasma concentration > 1.7 mmol/L (> 150 mg/dL) is abnormal for both men and women. For HDL-cholesterol (the so-called good or protective cholesterol) a fasting plasma concentration less than 1.0 mmol/L (< 40 mg/dL) for men and less than 1.3 mmol/L (< 50 mg/dL) for women is abnormal.
Elevated blood pressure
Although the World Health Organization (WHO) International Society of Hypertension defines hypertension as a blood pressure > 140/90 mmHg, elevated blood pressure in the context of the metabolic syndrome is a blood pressure > 130/85 mmHg. If a patient’s blood pressure is below this defining level but is on antihypertensive medication, he is still regarded as being positive for this risk factor.
nsulin resistance
Insulin is a peptide hormone that regulates glucose metabolism. It is produced and secreted into the portal circulation by b cells in the pancreatic islets. In the post-prandial state, it facilitates the uptake of glucose into the liver, muscle, and fat. In the fasting state, it regulates the release of glucose by the liver. As a result, blood glucose level is maintained within a range of 3.9—6.1 mmol/L (70—110 mg/dL) in good health. Peripheral tissues of patients with the metabolic syndrome are resistant to the action of insulin, which is determined genetically and by environmental factors. Although the defining limit of frank diabetes mellitus is a fasting plasma glucose concentration > 7.0 mmol/L (> 126 mg/dL), insulin resistance manifests itself as a pre-diabetic state in which fasting plasma glucose concentration is > 5.6 mmol/L (> 100 mg/dL). (While the NCEP-ATP III defined insulin resistance originally as a fasting plasma glucose concentration > 6.1 mmol/L or > 110 mg/dL, the level of > 5.6 mmol/L or > 100 mg/dL proposed by the American Diabetes Association has become the current defining limit of this risk factor.)
The limits of these risk factors that define the metabolic syndrome are summarized below:
1. Central obesity: Waist circumference > 90 cm (Chinese men); > 80 cm (Chinese women); > 85 cm (Japanese men); > 90 cm (Japanese women); > 102 cm (Caucasian men); > 88 cm (Caucasian women).
2. Hypertriglyceridemia: Fasting plasma triglycerides > 1.7 mmol/L or 150 mg/dL.
3. Low fasting plasma HDL-cholesterol concentration: < 1.0 mmol/L or 40 mg/dL (men); < 1.3 mmol/L or 50 mg/dL (women).
4. Elevated blood pressure: Blood pressure > 130/85 mmHg.
5. Insulin resistance: Fasting plasma glucose > 5.6 mmol/L or 100 mg/dL.
The interaction of risk factors in the metabolic syndrome
A patient with 3 or more of the risk factors mentioned above has the metabolic syndrome. While each of these 5 factors is by itself an independent predictor of risk, they are also interrelated and enhance each other’s role in the development of the syndrome. The presence of more than 1 factor in an individual amplifies his risk of developing cardiovascular diseases, stroke, and type 2 diabetes so that the whole is larger than the sum. Evolution of the syndrome is represented schematically below:
(1) Tissue resistance to the action of insulin is partially inherited but obesity, particularly central obesity, and sedentary lifestyle enhance insulin resistance.
(2) Insulin resistance means impaired glycemic control: Glucose is not taken up by tissues efficiently and remains in the blood stream, leading to hyperglycemia.
(3) Impaired glycemic control interferes with lipid metabolism, resulting in dyslipidemia.
(4) With dyslipidemia, fatty plaques and calcium are deposited on arterial walls. The condition is called atherosclerosis.
(5) Widespread atherosclerosis results in coronary heart disease and cerebral, renal, and peripheral vascular disease.
(6) Increase in blood glucose concentration from insulin resistance stimulates pancreatic b cells to secrete more insulin into the portal circulation. Increase in the blood level of insulin is called hyperinsulinemia. This occurs even before glucose concentration reaches diabetic level.
(7) Hyperinsulinemia increases sodium retention by the kidneys.
(8) Renal sodium retention contributes to elevation of blood pressure and development of hypertension.
(9) At the early stages of insulin resistance, hyper-secretion of insulin by pancreatic b cells can overcome this resistance somewhat and maintain blood glucose level relatively normal. With time the pancreas fails to compensate and full blown type 2 diabetes mellitus develops.
(10) Both diabetes and hypertension are major risk factors in the genesis of atherosclerosis.
Other risk factors associated with the metabolic syndrome
Since the entity of metabolic syndrome was first proposed by the World Health Organization (WHO) in 1999 and by the National Cholesterol Education Program in 2001, research has led to a clearer understanding of the role of lipid molecules in the genesis of atherosclerosis and the characterization of other risk factors in the metabolic syndrome:
Further fractionation of lipid molecules have helped to set new diagnostic and therapeutic goals. Small and dense LDL-cholesterol particles are more atherogenic than larger fluffy and buoyant particles. Elevated concentrations of lipoprotein-a and apolipoprotein-B are also associated with increased atherogenicity. As well, higher levels of very low density lipoprotein- (VLDL-) cholesterol and oxidized LDL-cholesterol are associated with worse cardiovascular outcome. HDL-cholesterol type 2, on the other hand, endows cardioprotection.
The prothrombotic state and the proinflammatory state are 2 other known risk factors that predispose a patient to atherosclerotic cardiovascular diseases and have not been included as risk factors in any of the definitions. While elevated levels of fibrinogen, homocystine, and type 1 plasminogen activator inhibitor in blood are markers of the prothrombotic state, elevated high-sensitivity C-reactive protein is marker for the proinflammatory state.
Cigarette smoking, by enhancing insulin resistance, is another lifestyle factor that has a negative impact on the metabolic syndrome.
Extent of the problem
In the United States, prevalence of the metabolic syndrome is 20% of the adult population older than 20 years and 40% among older citizens whose age is over 50 years. Similar data on Hong Kong citizens are not available, but the prevalence of 3 major metabolic-syndrome risk factors is considerable
Type 2 diabetes affects 1 in 10 adults with the majority not aware they have the disease.
Arterial hypertension in more than 10% of the population.
Overweight in 43% of the male population and 27% of the female.
It can be surmised that the metabolic syndrome is a growing health problem in the territory. Similar trends can be expected in other affluent cities of the Asia Pacific Region.
Treatment of the metabolic syndrome
Etiology of the metabolic syndrome is multifactorial and treatment should likewise be multifaceted. Attention should be directed towards lifestyle modification, improvement of plasma lipid profile, treatment of elevated blood pressure, prevention of diabetes, and reduction of other risk factors.
Modify lifestyle
Nearly all patients who have the metabolic syndrome are overweight and lead a sedentary lifestyle; many of them are smokers. Lifestyle modification in these patients should include:
Cessation of cigarette smoking. Smoking enhances insulin resistance, which is a major factor in the genesis of the metabolic syndrome.
Weight reduction of 5 – 10%, ideally through caloric restriction. Obese patients who are refractory to dieting may have to resort to pharmacotherapy and even bariatric surgery.
Physical exercise. It has been shown that exercise of 30 minute duration, 5 days a week, can improve all 5 of the NCEP-ATP III risk factors. The daily activity can even be broken into packages of 10 – 15 minutes each to reap the benefit. The intensity of exercise only needs to be moderate, with the subject exerting himself to a point when he is aware of his breathing but still can speak in un-interrupted sentences. See 2005-12-15 New and Revisited article “Exercise and Health” for more information on the benefits of exercise.
Treat dyslipidemia
The target lipid profile in treatment should be:
LDL-cholesterol < 2.6 mmol/L (< 100 mg/dL) in patients without vascular disease and < 1.8 mmol/L (< 70 mg/dL) in patients with known vascular disease;
triglyceride level < 1.7 mmol/L (< 150 mg/dL); and
HDL-cholesterol > 1.0 mmol/L (> 40 mg/dL) in men and > 1.3 mmol/L (> 50 mg/dL) in women.
Treatment modality should include:
A non-atherogenic diet that is low in cholesterol and saturated fat. The NCEP-ATP III guidelines mandate that cholesterol should be < 8 mmol (< 300 mg) per day, saturated fat < 7% of calories, and total fat no more than 25 – 35% of calories.
Elevated LDL-cholesterol levels require therapy with statins alone or combined with ezetimibe and resins.
Elevated triglyceride levels require therapy with niacin or fibrates with or without the addition of fish oil (omega-3 polyunsaturated fatty acids).
Low HDL-cholesterol can be treated with niacin or fibrates. While niacin is more effective than the fibrates in raising HDL-cholesterol, the fibrates are more effective thaiacin in lowering triglyceride levels.
Treat elevated blood pressure
Elevated blood pressure should be treated aggressively and a target blood pressure of 130/80 mmHg has been suggested. Standard antihypertensive drugs can be used but there is some indication that angiotensin converting enzyme inhibitors (ACEI) and angiotensin receptor blockers can delay the onset of type 2 diabetes, a major risk factor in the metabolic syndrome.
Delay and prevent the onset of type 2 diabetes
Insulin resistance is at the core of both the metabolic syndrome and type 2 diabetes. Diabetes by itself is an atherogenic disease. Therefore, there is a common goal in the treatment and prevention of the metabolic syndrome and type 2 diabetes. Adoption of the modified lifestyle mentioned above has been shown to be the most successful strategy in delaying and preventing the onset of type 2 diabetes and is advocated by all authorities. Treatment with oral hypoglycemic agents is another, though less effective, approach. A consensus opinion on this pharmacological strategy has not been reached. See 2006-01-15 New and Revisited article “Prevention of Diabetes Mellitus” for more information on the prevention of type 2 diabetes.
Treat other risk factors
It is an attractive idea to be able to lower the concentration of the more atherogenic lipid molecules (small and dense LDL-cholesterol particles, VLDL-cholesterol, oxidized LDL-cholesterol, lipoprotein-a and apolipoprotein-B) and to increase the level of the cardioprotective HDL-cholesterol type 2, but data on the effectiveness of these manipulations are still lacking. Data on treating the prothrombotic and proinflammatory sates are equally missing although most doctors will prescribe aspirin for its anti-platelet action.
video
Endocrine hypertension includes the following disorders.
Primary aldosteronism
The most common form of endocrine hypertension. It has been estimated to affect 5 percent to 10 percent of all patients with hypertension and is often underdiagnosed. Excessive aldosterone production by the adrenal glands leads to fluid retention, loss of potassium and hypertension. Eventually, hyperaldosteronism may cause enlargement of the heart (left ventricular hypertrophy). The two most common forms of primary aldosteronism are Conn’s syndrome whereby a single adrenal tumor produces excessive aldosterone versus bilateral adrenal hyperplasia, in which both adrenal glands are enlarged and cause hyperaldosteronism. Blood tests, including an aldosterone, plasma renin activity (PRA) and electrolytes should be ordered first. Further urine or blood testing should be done to confirm the diagnosis. A CT scan of the adrenal glands is then completed. In some cases, adrenal vein sampling may be necessary to help differentiate the cause of the primary aldosteronism. Conn’s syndrome can potentially be cured by surgical removal of the affected adrenal tumor. Bilateral adrenal hyperplasia is best treated with medications such as spironolactone or eplerenone.
Cushing’s syndrome
A hormonal disorder of excess cortisol production by the adrenal glands. ACTH is the hormone signal from the pituitary gland that stimulates cortisol production by the adrenal glands. Excess cortisol levels lead to Cushing’s syndrome. This can be due to direct adrenal involvement (adrenal Cushing’s) which is independent of ACTH secretion (i.e., ACTH-independent). ACTH-dependent Cushing’s disease is either due to a pituitary tumor (common) or to ectopic ACTH syndrome (uncommon). ACTH-dependent Cushing’s syndrome accounts for about 80 percent of all cases of Cushing’s. People with Cushing’s syndrome often have other endocrine-related disorders including diabetes, obesity, hypertension, kidney stones and osteoporosis. Many patients also suffer from depression. Testing for Cushing’s syndrome includes blood, urine and salivary testing. An MRI of the pituitary or a CT scan of the adrenal glands will then be done. If the patient has ACTH-dependent Cushing’s syndrome, inferior petrosal sinus sampling (IPSS) is ofteeeded to differentiate the pituitary from the ectopic form. Cushing’s syndrome can often be quite challenging to diagnose. Cushing’s syndrome is potentially cured by surgery but can also be treated with certain types of medications. Even after surgical cure, the disease can recur, so careful follow-up of all patients is needed.
A syndrome caused by tumors of the adrenal glands. This syndrome is rare but should always be excluded in patients who have adrenal tumors. These tumors produce excessive amounts of adrenaline, noradrenaline or other catecholamines. While symptoms often include sweating, palpitations and headache, patients can also have many other symptoms. Patients with a pheochromocytoma have episodic or sustained hypertension. Some patients present with markedly elevated blood pressure readings known as hypertensive crisis, which is a medical emergency. About 10 percent of these tumors are located outside the adrenal glands (extra-adrenal) in various locations in the body. Extra-adrenal pheochromocytomas are also known as paragangliomas. About 10 percent of the tumors are malignant. Another 10 percent of pheochromocytomas are part of multiple endocrine neoplasia syndromes (MEN syndrome I or II) which are genetic conditions that run in families. MEN syndromes can involve other endocrine organs such as the parathyroid glands, the pituitary, thyroid as well as other organs such as the kidney, pancreas or stomach.
Acromegaly
A tumor of the pituitary gland that leads to excess growth hormone (GH) and IGF-1 levels. Symptoms include joint and muscle problems, headache and vision problems. Patients tend to have very large hands, feet and tongue, and a prominent jaw. They can develop hypertension and diabetes as well.
Severe untreated hyperthyroidism or hypothyroidism
These disorders, if severe enough, can be associated with elevated blood pressure. Treatment of the thyroid disorder usually lowers the blood pressure to normal.
Other types of endocrine hypertension:
Primary adrenal hyperplasia — a subtype of primary aldosteronism. Surgery may cure this disorder.
· Glucocorticoid remediable aldosteronism (GRA) — a rare form of primary aldosteronism caused by a genetic mutation; it occurs in many family members.
· Familial hyperaldosteronism — rare form of primary aldosteronism in which about half of each generation develops hyperaldosteronism.
· Pseudohypoaldosteronism type 2 (Gordon’s syndrome) — patients develop hypertension and have high potassium levels (hyperkalemia).
· Liddle’s syndrome — another rare genetic form of hypertension in which patients have very low levels of aldosterone (pseudoaldosteronism)
· Apparent mineralocorticoid excess (AME) — another rare genetic form of hypertension.
· Licorice ingestion — pseudoaldosteronism due to ingestion of certain types of licorice (usually black licorice). This leads to high blood pressure and low potassium levels.
Other syndromes of low potassium (hypokalemia) without associated hypertension:
· Bartter’s syndrome — detected in infancy or childhood with symptoms of severe hypokalemia and other birth defects.
· Gitelman’s syndrome — a milder form of hypokalemia that occurs in young adults. Patients usually have low magnesium levels as well. These patients do not have hypertension.
Although initially considered a rarity, primary aldosteronism now is considered one of the more common causes of secondary hypertension (HTN). Litynski reported the first cases, but Conn was the first to well characterize the disorder, in 1956. Conn syndrome, as originally described, refers specifically to aldosteronism secondary to an adrenal aldosteronoma. (See Etiology.)
Based on older data, it was originally estimated that aldosteronism accounted for less than 1% of all patients with HTN. Subsequent data, however, indicated that it may actually occur in as many as 5-15% of patients with HTN. Sldosteronism may occur in an even greater percentage of patients with treatment-resistant HTN. (See Epidemiology.)
Although aldosteronism is still a considerable diagnostic challenge, recognizing the condition is critical because aldosteronism-associated HTN can often be cured with the proper surgical intervention. The diagnosis is generally 3-tiered, involving an initial screening, a confirmation of the diagnosis, and a determination of the specific subtype of aldosteronism. (See Presentation, Workup, Treatment, and Medication.)
Although prior studies suggested that aldosteronomas were the most common cause of aldosteronism (70-80% of cases), later epidemiologic work indicated that the prevalence of aldosteronism due to bilateral idiopathic adrenal hyperplasia (IAH) is higher than had previously been believed. These reports suggested that IAH may be responsible for as many as 75% of aldosteronism cases. Moreover, reports have described a rare syndrome of aldosteronism characterized by histologic features intermediate between adrenal adenoma and adrenal hyperplasia (see Etiology). (See the images below.)
Magnetic resonance imaging (MRI) scan in a patient with Conn syndrome showing a left adrenal adenoma
.
Scintigram obtained by using iodine-131-beta-iodomethyl-norcholesterol (NP-59) in a 59-year-old man with hypertension shows fairly intense radionuclide uptake in the right adrenal tumor. At surgery, a Conn tumor was confirmed.
Clinically, the distinction between the 2 major causes of aldosteronism is vital because the treatment of choice for each is different. While the treatment of choice for aldosteronomas is surgical extirpation, the treatment of choice for IAH is medical therapy with aldosterone antagonists. (See Treatment and Medication.)
Entities known to cause aldosteronism include the following (see the image below):
· Aldosterone-producing adenomas (APAs)
· Aldosterone-producing renin-responsive adenomas (AP-RAs)
· Bilateral adrenal (glomerulosa) hyperplasia or IAH
· Primary adrenal hyperplasia (PAH)
· Familial forms of aldosteronism
· Scintigram obtained by using iodine-131-beta-iodomethyl-norcholesterol (NP-59) in a 59-year-old man with hypertension shows fairly intense radionuclide uptake in the right adrenal tumor. At surgery, a Conn tumor was confirmed.
The ovaries and kidneys are the 2 organs described in the literature that, in the setting of neoplastic disease, can be ectopic sources of aldosterone, but this is a rare occurrence.
Approach Considerations
Among the major goals of therapy for primary aldosteronism are (1) normalization of blood pressure, (2) normalization of levels of serum potassium and other electrolytes, and (3) normalization of serum aldosterone levels.
The appropriate treatment for aldosteronism depends on its cause. Although hypertension (HTN) is frequently cured after unilateral adrenalectomy in patients with aldosteronism secondary to an adrenal aldosteronoma, the mean cure rate is only 19% after unilateral or bilateral adrenalectomy in patients with idiopathic adrenal hyperplasia (IAH). Therefore, medical management is the treatment of choice for the IAH variant of aldosteronism. (See the chart below.)
Effects of main antihypertensives on the renin-angiotensin system.
In patients with an adrenal aldosteronoma, medical therapy is used preoperatively to control blood pressure and correct hypokalemia, thus decreasing surgical risk. Medical therapy is also administered to patients with persistent HTN postoperatively, poor surgical candidates, and patients who refuse surgery.
In patients with heart failure who have secondary aldosteronism, aldosterone antagonism by spironolactone and eplerenone has been demonstrated to confer survival benefit.
Diet
A low-salt diet, although helpful in achieving blood pressure control in aldosteronism, may be associated with false-negative results on biochemical testing.
A high-salt diet makes the achievement of blood pressure control more difficult and may cause false-positive results on biochemical testing.
Pharmacologic Therapy
Calcium channel blockers
By inhibiting the intracellular calcium flux in the adrenocortical cells, the dihydropyridine calcium channel blockers reduce the production of aldosterone in response to a variety of stimulants, including potassium, corticotropin, and angiotensin-II.
Nifedipine is the most extensively studied of these medications; however, although nifedipine causes a significant improvement in patients with hypertension (HTN), it does not address the pathophysiology of the condition. The plasma renin activity (PRA), aldosterone levels, plasma volume, and serum potassium concentrations remain essentially unchanged while using nifedipine.
Mineralocorticoid antagonists
Mineralocorticoid antagonists, such as spironolactone, achieve remarkable blood pressure control and normalization of the above-mentioned parameters, particularly in patients with aldosteronomas.
The salutary effects of spironolactone appear to be due mainly to its impact on salt and water balance rather than to its antagonism of aldosterone in the kidney. The combination of spironolactone and thiazides often provides even better blood pressure control than does spironolactone alone.
Because of the estrogenlike adverse effects of spironolactone, including impotence and gynecomastia, the incentive to develop a similarly effective antialdosterone agent without these adverse effects is considerable. Eplerenone is a selective antialdosterone agent that may fulfill this promise, because it is a specific aldosterone receptor antagonist that does not have the additional antiandrogen effects associated with spironolactone.
Glucocorticoids
In the subgroup of patients with glucocorticoid-remediable aldosteronism (GRA), the treatment of choice is the administration of the lowest possible dose of glucocorticoid that can be used to achieve adequate blood pressure control. Because of the potential adverse effects that can result from even subtle glucocorticoid excess, using short-acting glucocorticoids, such as prednisone and hydrocortisone (rather than dexamethasone), is generally best.
Other
ACE inhibitors and angiotensin receptor blockers are also potential treatment options. Less ideal medical treatment options include potassium-sparing diuretics, such as triamterene and amiloride, that are not mineralocorticoid antagonists. Amiloride acts at the level of the distal convoluted tubule but does not bind to mineralocorticoid receptors.
A few reports of the use of percutaneous injection of ethanol or acetic acid into aldosteronomas as a treatment modality exist; in these cases, the treatment was usually administered to patients for whom surgery was contraindicated. This technique is neither popular nor well validated. Furthermore, it requires the technical expertise of a highly skilled interventional radiologist.
Considerations
Nonsurgical therapy is also a viable treatment option in patients who have lateralizable disease but who are poor surgical candidates because of other coexisting comorbidities. It is also a viable treatment option in the rare setting of bilateral functional adrenal adenomas that would otherwise require bilateral adrenalectomy.
Adrenal Surgery
Surgery is the treatment of choice for the lateralizable variants of primary aldosteronism, including typical aldosteronomas, renin-responsive adenomas (RRAs), and primary adrenal hyperplasia (PAH).
Preoperatively, once the biochemical and anatomic diagnoses are made and confirmed, the patient should be started on a 3- to 5-week course of spironolactone. This serves as an additional diagnostic tool (in confirming the diagnosis of aldosteronism) and as a means of predicting the blood pressure response that can be expected postsurgery.
An adrenalectomy can be performed via a formal laparotomy or by using a laparoscopic technique (with performance of the latter becoming increasingly common). The laparoscopic optioow makes it possible to offer surgical therapy to relatively frail patients who would be unable to withstand a formal laparotomy. Ongoing studies are systematically evaluating the place of adrenal-conserving operations versus total unilateral adrenalectomy in these patients.
Among the options being studied are (1) partial adrenalectomy, in which a wedge resection of the gland with the adenoma is performed along with aldosteronoma enucleation, and (2) medulla-sparing adrenalectomy, in which an attempt is made to retain the adrenal medullary tissue while removing the cortex.
Outcomes
About 60-70% of patients are rendered normotensive following curative surgery for aldosteronomas when evaluated 1 year postoperatively. Hypertension (HTN) typically does not resolve immediately postoperatively but, rather, over 3-6 months. (Although following surgery, virtually all patients with an aldosteronoma have significant reductions in aldosterone secretion and blood pressure and also demonstrate a correction of hypokalemia.)
A retrospective study of 168 patients with primary aldosteronism who underwent an adrenalectomy found that HTN was cured or controlled in 77% of patients with a unilateral adenoma and in 68% of patients with aldosteronism who had no adenoma, but whose aldosterone-to-cortisol ratio was at least 5 times higher on the dominant side than on the nondominant side.
The percentage of patients who remain normotensive 5 years postoperatively is about 53%. The resolution of HTN following adrenalectomy invariably occurs in the setting of a family history in which HTN is absent and/or when there has been preoperative use of 2 or fewer antihypertensives by the patient.
Adrenalectomy has very little utility in the setting of idiopathic adrenal hyperplasia (IAH). In reported cases in which surgery has unintentionally been performed on patients with IAH, the effects on blood pressure, hypokalemia, and aldosterone hypersecretion have been minimal, further underpinning the necessity of making a correct diagnosis before making a case for adrenalectomy.
Persistence of HTN following apparent surgical treatment of lateralizable disease is most common in patients older than 45 years, in those who had HTN for more than 5 years prior to surgery, and in persons who did not respond preoperatively to spironolactone.
Persistent HTN may be related to resetting of baroreceptors, established hemodynamic changes, structural changes in the blood vessels, or coincidental essential HTN.
Another possibility to consider in persistent HTN is an incomplete resection of the adenoma, with remaining remnant hyperplastic tissue. The coexistence of hypertensive nephrosclerosis in some patients with persistent HTN is also a distinct possibility. The coexistence of other secondary causes of HTN needs to be considered as well; renal artery stenosis is an important consideration.
Preoperative and postoperative care
Prior to surgery, patients should receive at least 8-10 weeks of medical therapy in order to decrease blood pressure and to correct the metabolic syndromes that are often associated with aldosteronism.
Postoperatively, metabolic profiles should be closely monitored. Most patients do not develop permanent hypomineralocorticoidism and therefore do not require fludrocortisone replacement.
For patients who develop hypoaldosteronism, the symptoms may persist for a long time and may be akin to the delay observed in adrenal glucocorticoid recovery following chronic corticotropin suppression by exogenous steroids. However, if significant hyperkalemia develops, potassium supplements should be discontinued, and the patient can be started on furosemide at doses of 80-160 mg daily




{kind=link}
{kind=link}
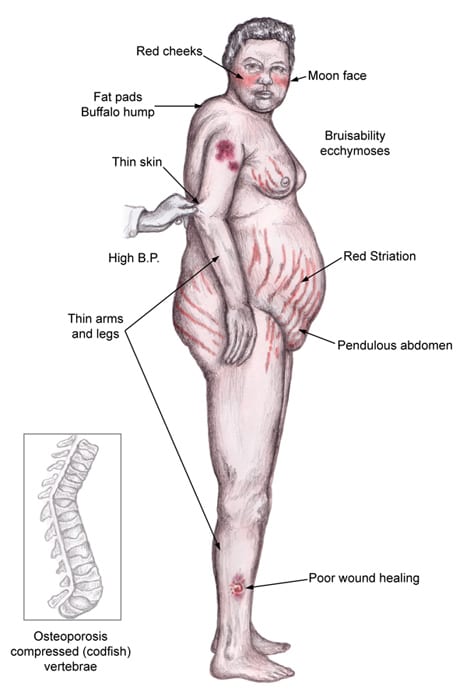{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}