THE MAIN METHODS OF FUNCTIONAL DIAGNOSTICS
OF PULMONARY DISEASES
Number of bronchopulmonary diseases has increased dramatically in recent decades. This requires a wider application of functional diagnostics of appropriate nosology. Early detection of violations biomechanics of breathing, dynamic monitoring of patients, choice of options treatment that best match by the detected violations, will provide modern, efficient therapy.
The widespread introduction of computerized devices, rejection of the use of conventional mechanical devices, are not only a positive value. Misunderstanding doctor that and how it explores, necessarily devalues the investigation, leading to serious diagnostic and tactical errors.
Modern medicine requires an understanding of the pathophysiological processes as a basis for diagnosis and treatment. The formation of a correct clinical thinking is impossible without knowledge of the mechanisms of development and course of disease at the molecular level. Namely the modern view of the pathophysiology of the respiratory system is the basis of a correct diagnostic search.
Overview of function

External respiration
- Ventilation — keeping fresh air in the alveoli
- Gas exchange — moving air into and out of blood
Transport of gases — in the blood (to / from pulmonary tissues / systemic tissues)
Internal respiration
- Systemic gas exchange
- Cellular respiration— use of oxygen and production of carbon dioxide by cells in order to transfer energy to ATP
-
Overall regulation of respiration
The “big picture” of respiratory function
Ventilation
Primary principle of ventilation
- Air moves down a pressure gradient (high pressure to low pressure)
Boyle’s Law — air pressure is inversely proportional to air volume
- That is, if volume goes up then pressure goes down and if volume goes down then pressure goes up
The respiratory cycle
- Inspiration
- Expand thorax/lungs, increasing the volume
- Decreases alveolar pressure (PA) below atmospheric pressure (PB), causing air to move from atmosphere into lung
- Inspiration: PA < PB
- Mostly the diaphragm that does this
- In deep breathing (as in exercising or as in sighing during A&P class [of course I hear you!]), external intercostal (“between the rib”) muscles raise ribs up and out (further expanding thorax / lungs)
- Compliance
- Ease of stretch
- Allows tissues of lungs/thorax to expand easily during inspiration
- Expiration
- Relax thorax/lungs, decreasing the volume
- Increases alveolar pressure (PA) above atmospheric pressure (PB), causing air to move from lung to atmosphere
- Expiration: PA > PB
- Mostly the elastic recoil of the diaphragm that does this
- In deep breathing, internal intercostals pull ribs downward and inward (further reducing volume of thorax / lungs)
SPIROMETRY
Spirometry (meaning the measuring of breath) is the most common of the Pulmonary Function Tests (PFTs), measuring lung function, specifically the measurement of the amount (volume) and/or speed (flow) of air that can be inhaled and exhaled. Spirometry is an important tool used for generating pneumotachograph to assessing conditions such as asthma, pulmonary fibrosis, cystic fibrosis, and COPD.
Spirometry testing
The spirometry test is performed using a device called a spirometer, which comes in several different varieties. Most spirometers display the following graphs:
- a volume-time curve, showing volume (liters) along the Y-axis and time (seconds) along the X-axis
- a flow-volume loop, which graphically depicts the rate of airflow on the Y-axis and the total volume inspired or expired on the X-axis
The most commonly used guidelines for spirometric testing and interpretation are set by the American Thoracic Society (ATS) and the European Respiratory Society (ERS).
Flow-Volume loop showing successful FVC maneuver. Positive values represent expiration, negative values represent inspiration. The trace moves clockwise for expiration followed by inspiration. (Note the FEV1, FEV1/2 and FEV3 values are arbitrary in this graph and just shown for illustrative purposes, they must be recorded as part of the experiment).
Procedure
The basic FVC test varies slightly depending on the equipment used.
Generally, the patient is asked to take the deepest breath they can, and then exhale into the sensor as hard as possible, for as long as possible. It is sometimes directly followed by a rapid inhalation (inspiration), in particular when assessing possible upper airway obstruction. Sometimes, the test will be preceded by a period of quiet breathing in and out from the sensor (tidal volume), or the rapid breath in (forced inspiratory part) will come before the forced exhalation.
During the test, soft nose clips may be used to prevent air escaping through the nose. Filter mouthpieces may be used to prevent the spread of microorganisms, particularly for inspiratory maneuvers.
Limitations of test
The maneuver is highly dependent on patient cooperation and effort, and is normally repeated at least three times to ensure reproducibility. Since results are dependent on patient cooperation, FEV1 and FVC can only be underestimated, never overestimated.Due to the patient cooperation required, spirometry can only be used on children old enough to comprehend and follow the instructions given (typically about 4-5 years old), and only on patients who are able to understand and follow instructions – thus, this test is not suitable for patients who are unconscious, heavily sedated, or have limitations that would interfere with vigorous respiratory efforts. Other types of lung function tests are available for infants and unconscious persons.
Ventilation is characterised by different volumes and capacities, which are measures of combined volume values:
1. Tidal volume – volume inhaled and exhaled during normal breathing
2. Inspiratory reserve volume – volume which can be inhaled additionally after normal inspiration
3. Expiratory reserve volume – volume which can be exhaled additionally after normal expiration
4. Residual volume – volume remaining in the lungs after maximal expiration
5. Vital capacity – volume which can be exhaled after maximal inspiration (sum of 1, 2 and 3)
6. Inspiratory capacity – volume that can be inhaled additionally after normal expiration (sum of 1 and 2)
7. Functional residual capacity – volume remaining in the lung after the end of a normal expiration (sum of 3 and 4)
8. Total capacity – volume filling the lung after maximal inspiration (sum of 1, 2, 3 and 4)
All pulmonary volumes and capacities are about 20 to 25 percent smaller in women than in men. In large and athletic people the values obtained exceed those of small and asthenic subjects.
The flow-volume curve during a normal inspiration and expiration (‘tidal loop’), and subsequently recorded during forced in- and expirations serve to demonstrate the considerable ventilatory reserves available to a healthy subject. During exercise the level of ventilation can be increased by greater inspiratory and expiratory flows, as well as by increasing tidal volume and respiratory rate. In general in exercising healthy subjects the end-expiratory lung volume remains by and large the same.
Lung volumes and capacities
Explanation of common test values in FVC tests
|
Abbreviation |
Name |
Normal value |
Description |
|
FVC |
Forced Vital Capacity |
80–120%
|
This is the total amount of air that can forcibly be blown out after full inspiration, measured in liters. |
|
FEV1 |
Forced Expiratory Volume in 1 Second |
70-120% |
This is the amount of air that you can forcibly blow out in one second, measured in litres. Along with FVC it is considered one of the primary indicators of lung function. |
|
FEV1 / FVC |
FEV1% |
Within 5% of the predicted ratio |
This is the ratio of FEV 1 to FVC. In healthy adults this should be approximately 75 – 80%. |
|
PEF |
Peak Expiratory Flow |
70-90% |
This is the speed of the air moving out of your lungs at the beginning of the expiration, measured in liters per second. |
|
FEF 25-75% or 25-50% |
Forced Expiratory Flow 25-75% or 25-50% |
60-90 % |
This is the average flow (or speed) of air coming out of the lung during the middle portion of the expiration (also sometimes referred to as the MMEF, for maximal mid-expiratory flow). |
|
FIF 25-75% or 25-50% |
Forced Inspiratory Flow 25%-75% or 25%-50% |
|
This is similar to FEF 25%-75% or 25%-50% except the measurement is taken during inspiration. |
|
TV |
Tidal Volume |
390– 500mL |
During the respiratory cycle, a specific volume of air is drawn into and then expired out of the lungs. This volume is tidal volume. |
|
MVV |
Maximum Voluntary Ventilation |
|
A measure of the maximum amount of air that can be inhaled and exhaled in one minute, measured in liters/minute. |
|
RV |
Residual volume |
75–120% |
|
|
TLC |
Total Lung Capacity |
80–120%
|
This is the maximum volume of air present in the lungs |
|
DLCO |
Diffusing capacity of lung for carbon monoxide |
60–120% |
Diffusing Capacity (DLCO) is the carbon monoxide uptake from a single inspiration in a standard time (usually 10 sec). Since air consists of very minute or traces of CO, so 10 second is considered to be the standard time, then rapidly blow it out (exhale). The exhaled gas is tested to determine how much of the tracer gas was absorbed during the breath. |
Changes of common test values in FVC tests
|
Pulmonary Parameter |
Obstructive Disease |
Restrictive Disease |
|
VC (vital capacity) |
normal or decreased |
decreased |
|
TLC (total lung capacity) |
normal or increased |
decreased |
|
RV (residual volume) |
increased |
decreased |
|
FEV1/FVC |
decreased |
normal or increased |
|
FEF25%-75% |
decreased |
Normal |
|
MBC (maximum breathing capacity) |
decreased |
normal |
|
|
|
|
Restrictive respiratory insufficiency. This form of respiratory insufficiency arises, when the extensibility lung is reduced, that is when they be not capable easily to be straightened. To carry out a breath, it is necessary to increase transpulmonary pressure, and it can be made at the expense of increase of respiratory muscles action.
restrictive insufficiency arises in case inflammation and edema lung. Owing to arterial both venous hyperemia and swelling of interstitial tissue the alveoles is compressed from the outside and completely are not straightened.
By often cause is fibrose lung, that is grow up rough fibrose connective tissue on place perished elements of parenhima, elastic fibres and capillaries. By fibrose are finished such illnesses, as emphysema, silicosis, anthracosis and other. To decreasing of extensibility lung may lead disturbance of surfactant system. Under surfactant is understood surface-active substances, which reduce a surface tension in an alveole. influencing on a surface tension, surfactant regulates elastic recoil of lung. as the major function it is necessary to consider prevention of alveolares collapse. It acts as the antistick factor, providing stability of alveole.
The deficiency of surfactant can arise in case of insufficient synthesis it or excessive remove from a surface of alveoles. The insufficient synthesis is characterized for illness of hyaline membranes iewborn, for want of which destroy intraalveolares septum and in alveoles is stored hyaline with epithelial cells and form elements of blood. Ecquired decrease of surfactant is observed for want of asphyxia, acidosis, pneumonia, pollution of air. The defect of surfactant predetermines high surface tension of alveoles and high resistance lung for want of expansion by their inhaled air.
Besides, by cause of restrictive insufficency may be аthelectasis ( fall of alveoles and stopping of their ventilation), рneumothorax, deformation of thorax, paralysis of respiratory muscles.
Obstructive insufficiency. Obstruction of respiratory ways is narrowing their lumen and increase of resistance to movement of air. The damage can be located as in upper respiratory ways (with diameter of 2 mm and more), and in lower respiratory ways (diameter – up to 2 mm).
Upper respiratory paths is understood cavity of mouth, nasal meatuses, pharynx, larynx, trachea, large bronchus.
Obstruction it may be is caused internal and externals mechanical trauma. Internal trauma most frequently it arises as complication of trachea-intubation, less often – after operation on larynx. External mechanical trauma – fractures of lower jaw, cervical cartilages, larynx cartilages, epiglossus, trachea, damage of language basis, mouth, neck. The mechanism of obstruction is spasm, edema also paralysis of voice slot, damage or off set of larynx cartilages, hematoma, edema of mucous membrane or serrounding tissues. Variety of an internal trauma – burns and inhalating of poisoning gases. In these cases develops edema of mucous upper respiratory paths.
Bleeding in respiratory ways is observed after operating interferences on head and neck, after tonsilectomy, tracheostomy. Sometimes bleeding happens spontaneous, for example from nose. The bleeding especially is dangerous when the patient is in coma or under narcosis, that is when the drainage of respiratory paths is impossible. Aspiration of foreign body is observed in children in the age from 6 months to 4 years more often. In the adult aspiration of foreign body occurs, usually, during reception of food, especially in state of alcoholic intoxication. Ather causes of ebstruction lower respiratory ways – necrotic ludvig`s angina (suprogenis necrotic flegmona of oral bottom cavity of an infectious origin), subpharynx abscess, which cause is aerobic and anaerobic microflora, аngioneurotic edema, which develops as response on allergen and is accompanied of nettle-rash, asthma, rhinitis.
To obstruction of lower respiratory ways results aspiration of the liquid environments – of vomit mass, of blood, of water, and allergy response mainly on medical preparations – antibiotics and protein substitutes. It develops immediately, during 30 mines and appears hardly expressed laryngo- and bronchospasm.
Obstructive respiratory insufficiency arises also for want of chronic unspecific diseases lung – chronic bronchitis, emphysema, bronchoectasis, bronchial astma.
Emphysema is an illness, in which rupture interalveolar septums and lungs capillaries. By basis it is considered degraded collagen and elastic fibres of proteolytic enzymes, which thrown out from phagocytes under influences of the external factors – microorganisms, dust particles, tobacco smoke. In etiology of emphysema some role is allocated of hereditary predisposition, which essence consists in synthesis of defective collagen and elasthyne, insufficient synthesis of proteolytic enzymes inhibitors.
The mechanism of obstruction for want of emphysema explain so. Walls of bronchioles very thin and pliable. The lumen them is supported transpulmonaris more pressure. The more elasticity lung, the should be transpulmonaris more pressure to overcome elastic recoil. Bronchioles for want of it will be in an extended state. When the elasticity lung is reduced, it is enough for their stretch low transpulmonaris pressure. The force, which acts on walls bronchioles from within, decreases and also their lumen is narrowed. The decrease of lumen conducts to sharp increase of resistance to movement of air. As a result of it the breath is difficulty. But even more exhalation is difficulty. For want of emphysema it becomes active. the pressure in pleurae cavity increases, and bronchioles are compressed from the outside of lungs fabric. With the cource of time bronchioles compress completely, and the exhalation becomes impossible. Air becomes isolated in alveoles, which remain is blowed up.
The mechanism of obstruction for want of bronchial asthma is multicomponent. At the first place is аccumulation of viscous glasslike mucus in bronchus. It is connected with hypertrophy of mucous glands and hyperproductions by them mucus (hypercrinia). The viscous mucus is difficultly discharge and congest (mucostasis). The important role in the mechanism of mucostasis plays hyperplasia of goblet cells, which supersede cells of ciliata epithelium. Besides, arises edema mucous, spasm of circular and longitudinal smooth bronchus muscules. In the patients with bronchial asthma develops increased reactivity of bronchial muscles on specific and unspecific stimulus. The highest degree hyperreactivity is observed at once time or after an attack. Strong stimulus, which provokes bronchoconstriction in the patients of bronchial asthma, is the physical load.
PNEUMOTACHOMETRY
This measures the flow rate of gases during breathing. The breath is passed through a short tube (Fleisch tube) in which there is a fine mesh which presents a small resistance to the flow. The resulting pressure drop across the mesh is in proportion to the flow rate. The pressure drop is very small (e.g. 2 mmHg) and so the measuring circuit must be of high quality and produce very little drift with time. A differential pressure transducer is normally used.
- in the first exercise, air flow and tidal volume signals are recorded during normal respiration and the vital capacity manoeuvre.
- in the second exercise, the Forced Vital Capacity manoeuvre is recorded. The rate of the expired air flow will depend on the elastic recoil properties of the lung and the resistance to air flow as well as on the voluntary expiratory effort.
- the third exercise will show the expiratory flow vs. volume changes with increased expiratory resistance.
- CO2 and O2 concentrations will be recorded during different breathing patterns.
|
Lung volume and capacities |
|
|||||
|
|
Forced Vital Capacity manoeuvre
The Forced Vital Capacity (FVC) manoeuvre is based on the Vital Capacity manoeuvre with an added element of speed; an individual exhales with a maximal force and speed. The rate of the expired air flow will depend on the elastic recoil properties of the lung and the resistance to airflow as well as on the voluntary expiratory effort. A healthy individual is able to expel at least 80% of his/her vital capacity during the first second of forced expiration.
The start of the forced expiration is obtained by linear extrapolation of the steepest part of the volume-time diagram.
FVC is the volume change of the lung between a full inspiration to total lung capacity and a maximal expiration to residual volume. The measurement is performed during forceful expiration; the preceding maximal inspiration does not need to be done forcefully . The manoeuvre is performed together with the assessment of the FEV1 and of maximum expiratory flow-volume curves.
Flow-volume curve
It is the graph produced by plotting the instantaneous flow of respiratory gas against the simultaneous lung volume. The principal advantage of the flow-volume curve is that it can show whether flows are appropriate for a particular lung volume.
Study the shape of the expiratory flow trace (top part of diagram A above): after a rapid rise, there is a slow decline unlike the round inspiratory flow. Why? As you forcefully expire, the small airways are closing (pressure outside the small airways is greater than inside the small airways), therefore there is a further restriction to air flow (slow decline of last part of expiratory flow).
During inspiration, the airways are patent (unobstructed) because intrathoracic pressure opens the airways.
Can you identify the volume quantities (1, 2 and 3) on the flow-volume curve below constructed while the tidal volume and maximal inspiration/expiration were recorded?
Flow-volume plot changes with different airway conditions
Obstructive disease: Although all flow rates are diminished, expiratory prolongation predominates. What are examples of obstructive lung disease?
Restrictive disease: the flow-volume curve is narrowed because of diminished lung volumes, but the shape is generally the same as iormal volume. Flow rates are greater than normal at comparable lung volumes because the elastic recoil of lungs holds the airways open. What are examples of restrictive lung disease?
Fixed obstruction: the flow is equally limited during expiration and inspiration.
Breathing patterns and O2/CO2 analysis
Technical detail of the apparatus used to measure O2/CO2 : it operates with an infra-red transducer to measure CO2 concentration and a visible spectrum transducer to measure O2 concentration. It also consists of a variable pump which draws sample gas through the two transducers. The pump can be set to any flow rate in the range 35 ml/min to 200 ml/min. The analyzer has a response time of about 0.2 s (at ~200 ml/min).
The detail above shows the delay between respiratory phases and the rate of gas sampling: at the end of maximal expiration, a maximal CO2 content would be recorded.
Notice and explain differences in the gas concentrations in relation to the following breathing patterns:
- during normal breathing
- during a shallow and rapid respiration
- following the VC manoeuvre
- during and following inspiratory apnea
Peak Expiratory Flow Meter
Peak flow measurement is a procedure in which air flowing out of the lungs is measured. The measurement obtained is called the peak expiratory flow rate (PEFR), or peak expiratory flow (PEF).
Peak flow measurement may be obtained using a spirometer, an instrument with a mouth piece that measures the amount of air breathed in and/or out and the rate at which the air is inhaled and expelled from the lungs. Peak flow may also be measured with a peak flow meter (PFM), a portable, hand-held device. Both devices take the measurement as an individual forcefully blows into the mouthpiece of the device.
Spirometry is usually performed in a doctor’s office, clinic, or a hospital. A peak flow meter is small and light enough to be used almost anywhere.
There are several types of PFMs available. However, it is important that one continues to use the same type of PFM on a consistent basis, as the PEFR can vary among different brands and types of meters.
Peak flow measurement using a peak flow meter is particularly useful for individuals with asthma. During an asthma flare-up, the large airways in the lungs slowly begin to narrow. This slows the speed of air leaving the lungs. A peak flow meter, when used properly, can reveal narrowing of the airways well in advanced of an asthma attack. Peak flow meters can help determine:
· When to seek emergency medical care
· The effectiveness of an asthma management and treatment plan
· When to stop or add medication as directed by a doctor what triggers the asthma attack (such as exercise-induced asthma)
Other related procedures that may be used to diagnose problems of the lungs and respiratory tract include chest X-rays, bronchoscopy, bronchography, chest fluoroscopy, chest ultrasound, lung biopsy, lung scan, mediastinoscopy, oximetry, positron emission tomography (PET scan), pleural biopsy, pulmonary angiogram, pulmonary function tests, sinus X-ray, and thoracentesis. Please see these procedures for additional information.
Reasons for the procedure
A peak flow meter (PFM) can assist with the management of asthma. It can provide you and your doctor with information about how open the airways are in your lungs. The PFM can detect small changes in the large airways before you start to wheeze.
Using a PFM every day will let you know when your peak flows are starting to drop. This allows you to make early changes in your medication or routine to help prevent asthma symptoms from worsening. The PFM can also identify the value at which you will need to call your doctor or go to the emergency room.
Peak flow meters are primarily used for individuals who have asthma. Your doctor may not recommend that a PFM be used unless your asthma is considered moderate or severe and you are managed with medication(s). Peak flow meters are also useful in children who have asthma.
The measurements obtained by PFMs may also be useful in evaluating other conditions such as:
· Emphysema–a chronic lung condition that affects the alveoli, the smallest air sacks in the lungs
· Chronic bronchitis–a long-term inflammation of the bronchi, which results in the increased production of mucous, and other change
Risks of the procedure
Because obtaining peak flow measurement is a noninvasive procedure, it is safe for most individuals. It is quick and inexpensive. However, the individual must be able to follow clear, simple directions.
Having to take in deep breaths to perform the procedure may cause you to feel dizzy, light-headed, or short of breath.
The procedure may trigger coughing and/or wheezing.
There may be risks depending on your specific medical condition. Be sure to discuss any concerns with your doctor prior to the procedure.
Certain factors or conditions may interfere with the accuracy of peak flow measurement. These factors may include, but are not limited to, the following:
· Coughing during the procedure
· Poor seal around the mouthpiece while performing the procedure
· A dirty meter
· Blocking the mouthpiece with the tongue
· Use of bronchodilator (opens the airways) medication
· Use of a different type or brand of PFM, as the measurements may vary among brands and types of meters
Before the procedure:
· Your doctor will explain the procedure to you and offer you the opportunity to ask any questions that you might have about the procedure.
· Generally, no prior preparation, such as fasting, fluid restriction, or sedation is required. However, you may be asked to avoid eating a heavy meal before the test.
· Notify your doctor of all medications (prescription and over-the-counter) and herbal supplements that you are taking.
· Prior to beginning routine daily PFM monitoring, your doctor may instruct you to perform PFM on a more detailed schedule over two to three weeks in order to establish your “personal best” peak flow measurement. This personal best value will be used as a baseline for your routine measurements.
· Based on your medical condition, your doctor may request other specific preparation.
During the procedure
Peak flow measurement may be performed one or more times daily at the same time of day, whenever you are experiencing early warning signs of an asthma attack, or as otherwise directed by your doctor. You should always use the PFM before taking asthma medication. Your doctor may recommend other times when using a PFM is useful.
Generally, peak flow measurement follows this process:
1. Before each use, make sure the sliding pointer on the PFM is reset to the zero mark.
2. Hold the PFM by the handle.
3. Stand up straight.
4. Remove chewing gum or any food from your mouth.
5. Take a deep breath and put the mouthpiece in your mouth. Seal your lips and teeth tightly around the mouthpiece.
6. Blow out as hard and as fast as you can. Remember, a “fast blast” is better than a “slow blow.”
7. Note the number where the sliding pointer has stopped on the scale.
8. Reset the pointer to zero.
9. Repeat this routine three times. You will know you have done the technique correctly when the three readings are close together.
10. If you cough during a measurement, you should repeat it.
11. Record the highest of the three readings on a graph or in a notebook. Do not average these numbers together. This is called your “peak flow.”
12. Use the peak flow meter once a day, or as directed by your doctor. Measure peak flows about the same time each day. A good time might be when you first wake up or at bedtime.
After the procedure
Any type of care after the procedure will be based on the results of the procedure. Your doctor will instruct you about your peak flow zones and how you should respond when your peak flow measurement indicates a particular zone.
What are peak flow zones?
Peak flow zones are based on the traffic light concept: red means danger, yellow means caution, and green means safe. These zones are different for each person. Your doctor will help determine your peak flow zones. The three peak flow zones include:
· Green: This is the GO zone. The green zone is from 80 to 100 percent of your highest peak flow reading, or personal best. This is the zone you should be in every day. Measurements in this zone signal that air moves well through the large airways and that you can do the usual activities and go to sleep without trouble. You should continue to follow your asthma plan as directed by your doctor.
· Yellow: This is the CAUTION or SLOW DOWN zone. The yellow zone is from 50 to 80 percent of your personal best. Measurements in this zone are a clue that the large airways are starting to narrow. You may begin to have mild symptoms, such as coughing, feeling tired, feeling short of breath, or feeling like your chest is tightening. These symptoms may keep you from your usual activities or from sleeping well. You should notify your doctor at this time. He or she may instruct you to increase or change your medications and give you additional instructions to help prevent your symptoms from worsening.
· Red: This is the STOP zone. The red zone is less than 50 percent of your personal best. Readings in this zone mean severe narrowing of the large airways has occurred. This is a medical emergency and you should get help right away. You may now be coughing, very short of breath, wheezing both when breathing in and out, or having retractions. You may also have problems walking and talking. You should take your reliever medicatioow and call your doctor.
The goal of the peak flow zones is to recognize early symptoms of uncontrolled asthma.
Normal value of peakfloumetry:
Male
|
height |
15 |
20 |
25 |
30 |
35 |
40 |
45 |
50 |
55 |
60 |
65 |
70 |
|
160 sm |
518 |
568 |
598 |
612 |
613 |
606 |
592 |
578 |
565 |
555 |
544 |
534 |
|
168 sm |
530 |
580 |
610 |
623 |
623 |
617 |
603 |
589 |
577 |
566 |
556 |
546 |
|
175 sm |
540 |
590 |
622 |
636 |
635 |
627 |
615 |
601 |
588 |
578 |
568 |
558 |
|
183 sm |
552 |
601 |
632 |
645 |
646 |
638 |
626 |
612 |
600 |
589 |
578 |
568 |
|
190 sm |
562 |
612 |
643 |
656 |
656 |
649 |
637 |
623 |
611 |
599 |
589 |
579 |
Female
|
height |
15 |
20 |
25 |
30 |
35 |
40 |
45 |
50 |
55 |
60 |
65 |
70 |
|
145 sm |
438 |
445 |
450 |
452 |
452 |
449 |
444 |
436 |
426 |
415 |
400 |
385 |
|
152 sm |
450 |
456 |
461 |
463 |
463 |
480 |
456 |
448 |
437 |
425 |
410 |
396 |
|
160 sm |
461 |
467 |
471 |
474 |
473 |
470 |
467 |
458 |
449 |
437 |
422 |
407 |
|
168 sm |
471 |
478 |
482 |
485 |
484 |
482 |
478 |
470 |
460 |
448 |
434 |
418 |
|
175 sm |
481 |
488 |
493 |
496 |
496 |
493 |
488 |
480 |
471 |
458 |
445 |
428 |
Children
|
height |
91 |
99 |
107 |
114 |
122 |
130 |
137 |
145 |
152 |
160 |
168 |
175 |
|
|
100 |
120 |
140 |
170 |
210 |
250 |
265 |
325 |
380 |
400 |
440 |
480 |
BODY PLETHYSMOGRAPHY
Spirometry is the standard method for measuring most relative lung volumes; however, it isincapable of providing information about absolute volumes of air in the lung. Thus a differentapproach is required to measure residual volume, functional residual capacity, and total lungcapacity. Two of the most common methods of obtaining information about these volumes are gasdilution tests and body plethysmography.
In body plethysmography, the patient sits inside an airtight box, inhales or exhales to aparticular volume (usually FRC), and then a shutter drops across their breathing tube. Thesubject makes respiratory efforts against the closed shutter (this looks, and feels, likepanting), causing their chest volume to expand and decompressing the air in their lungs. Theincrease in their chest volume slightly reduces the box volume (the non-person volume of the box)and thus slightly increases the pressure in the box.
Using the data from the plethysmography requires use of Boyles Law.![]()
To compute the original volume of air in thelungs, we first compute the change in volume of the chest.Using Boyle’s Law (P1V1=P2V2, atconstant temperature), we set the initial pressure in the box times the initial volume of the box(both of which we know), equal to the pressure times volume of the box at the end of a chestexpansion (of which we know only the pressure).
We solve for the volume of the box during the respiratory effort. The difference between thisvolume and the initial volume of the box, is the change in volume of the box, which is the same asthe change in volume of the chest. Armed with this piece of information, we use Boyle’s Lawagain, this time on the fixed amount of gas in the chest before and at the end of a respiratoryeffort. We set the initial volume of the chest (unknown) times the initial pressure at the mouth(known), equal to the inspiratory volume of the chest (the same unknown volume plus the change inthe volume of the chest, which we have just computed) times the pressure at the mouth during theinspiratory effort (known). Now we solve for the unknown volume, which will be the original volumeof gas present in the lungs when the shutter was closed. As mentioned before, the shutter isusually closed at the end of a normal exhalation, or at FRC.
Body plethysmography is particularly appropriate for patients who have air spaces within the lungthat do not communicate with the bronchial tree. In these individules, gas dilution methods ofmeasurement would give an erroneously low volume reading.
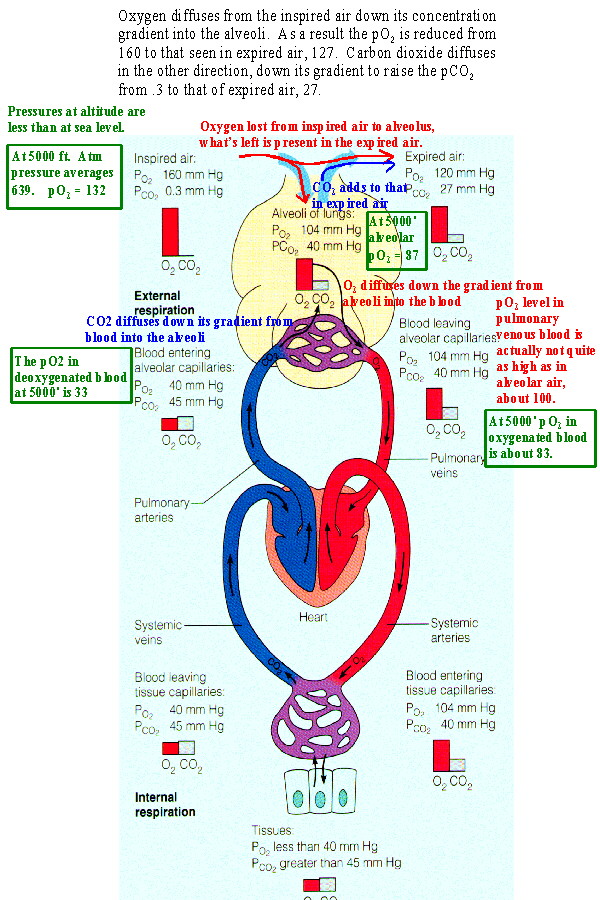
Movement of the respiratory gases is due to diffusion. Diffusion results from a concentration gradient which is expressed for gases as the difference in partial pressures.
Dalton’s Law of Partial Pressures states that The partial pressure of a gas in a mixture is calculated by multiplying the fraction occupied by the gas times the total pressure of the mixture.
The mixture of gases under consideration is the air shows the partial pressures of its gases at STP (standard temperature and pressure at sea level).
Oxygen is present at nearly 21% of ambient air. Multiplying .21 times 760 mmHg (standard pressure at sea level) yields a pO2 of about 160. Carbon dioxide is .04% of air and its partial pressure, pCO2, is .3.
As Figure shows there is a partial pressure gradient between inspired air and the alveolus with alveolar air having a pO2 of 104 and a pCO2 of 40. So oxygen diffuses into the alveoli from inspired air and carbon dioxide diffuses from the alveoli into air which will be expired. This causes the levels of oxygen and carbon dioxide to be intermediate in expired air when compared to inspired air and alveolar air. Some oxygen has been lost to the alveolus, lowering its level to 120, carbon dioxide has been gained from the alveolus raising its level to 27.
Likewise a concentration gradient causes oxygen to diffuse into the blood from the alveoli and carbon dioxide to leave the blood. This produces the levels seen in oxygenated blood in the body. When this blood reaches the systemic tissues the reverse process occurs restoring levels seen in deoxygenated blood.
Gas Exchange function
The primary function of the respiratory system is to exchange oxygen and carbon dioxide. Inhaled oxygen enters the lungs and reaches the alveoli. The layers of cells lining the alveoli and the surrounding capillaries are each only one cell thick and are in very close contact with each other. This barrier between air and blood averages about 1 micron (1/10,000 of a centimeter) in thickness. Oxygen passes quickly through this air-blood barrier into the blood in the capillaries. Similarly, carbon dioxide passes from the blood into the alveoli and is then exhaled.
Oxygenated blood travels from the lungs through the pulmonary veins and into the left side of the heart, which pumps the blood to the rest of the body. Oxygen-deficient, carbon dioxide-rich blood returns to the right side of the heart through two large veins, the superior vena cava and the inferior vena cava. Then the blood is pumped through the pulmonary artery to the lungs, where it picks up oxygen and releases carbon dioxide.
To support the exchange of oxygen and carbon dioxide, about 6 to 10 liters of air per minute are brought in and out of the lungs, and about three tenths of a liter of oxygen is transferred from the alveoli to the blood each minute, even when the person is at rest. At the same time, a similar volume of carbon dioxide moves from the blood to the alveoli and is exhaled. During exercise, it is possible to breathe in and out more than 100 liters of air per minute and extract 3 liters of oxygen from this air per minute. The rate at which oxygen is used by the body is one measure of the rate of energy expended by the body. Breathing in and out is accomplished by respiratory muscles.
Gas Exchange Between Alveolar Spaces and Capillaries
The function of the respiratory system is to exchange two gases: oxygen and carbon dioxide. The exchange takes place in the millions of alveoli in the lungs and the capillaries that envelop them. As shown below, inhaled oxygen moves from the alveoli to the blood in the capillaries, and carbon dioxide moves from the blood in the capillaries to the air in the alveoli.
Three processes are essential for the transfer of oxygen from the outside air to the blood flowing through the lungs: ventilation, diffusion, and perfusion. Ventilation is the process by which air moves in and out of the lungs. Diffusion is the spontaneous movement of gases, without the use of any energy or effort by the body, between the gas in the alveoli and the blood in the capillaries in the lungs. Perfusion is the process by which the cardiovascular system pumps blood throughout the lungs. The body’s circulation is an essential link between the atmosphere, which contains oxygen, and the cells of the body, which consume oxygen. For example, the delivery of oxygen to the muscle cells throughout the body depends not only on the lungs but also on the ability of the blood to carry oxygen and on the ability of the circulation to transport blood to muscle.
EXHALED BREATH ANALYSIS
Directly Determined Components of Exhaled BreathGases appearing in the exhaled breath as by-products of different metabolic pathways or after oral ingestion can be detected and quantitated. Thus, ethanol measurement has found wide application in the control of alcohol consumption by drivers. A recent application of interest is the installing of devices called Alcolocks or alcohol interlock systems in certain types of transportation vehicles in Sweden.
These are automatic control systems that are designed to prevent driving after excessive alcohol intake by requiring the driver to blow into an in-car breathalyzer before starting the ignition.
The alcohol interlock can be set at different levels and limits. Other interesting developments related to systemic bio-markers in exhaled breath are the attempts to directly assessgases associated with human morbidity, such as ammonia and acetone, with the latter being used also as a proxy forblood levels of glucose. The directly measured gases, which have been intensively investigated as biomarkers in lung morbidity, are nitric oxide (NO) and carbon monoxide.
Nitric Oxide
Gustafsson et al. were the first to detect NO, a highly reactive molecule, in the exhaled breath of animals and humans in 1991. Two years later, Alvin et al reported an increase of NO in the exhaled breath of asthmatic patients, which gave an impetus to research aimed at assessing the usefulness of this and other gases in different clinical situations. As a result, a much better insight was gained about the role NO plays in the regulation of the smooth muscle tone of the pulmonary blood vessels and the bronchi. The increase in NO during inflammation has been demonstrated to be due to activation of inducible NO synthase expressed by epithelial cells in response to proinflammatory cytokines and oxidants.
Because expectations were high, several companies engineered devices using the principle of chemiluminescence to measure the minimal amounts of NO in the exhaled air (in the range of parts per billion), with which many dozens of studies were conducted, bringing the method to the stage of clinical use. The role of different extraneous factors, such as inspiration maneuvers, breath holding, exhalation flow rate, exhalation time, and oral pressure, with possible bearing on exhaled NO (eNO) measurement, has been elucidated.
Fractional eNO (FeNO) levels were shown to correlate with sputum eosinophil count, airway hyperresponsiveness, bronchodilator response, serum IgE levels, allergen skin prick testing, asthma symptoms, and lung function.
This led to the general belief that atopy is associated with higher levels of eNO. However, the analysis of different subgroups of atopic individuals now suggests that it is the active inflammation in atopic individuals with clinical manifestations of airway disease, rather than atopy itself, that accounts for the increased production of eNO.
Other patient characteristics, such as age, height, weight, body mass index, sex, and race, may affect the measurements to a lesser degree, as well as activities such as smoking, alcohol use, spirometric testing, sputum induction, and environmental exposures.
The currently available equipment and dedicated software allow accounting for different confounding factors. These ground studies paved the way for standardization of the method, and subsequently the American Thoracic Society and the European Respiratory Society published recommendations for measuring FeNO, as it was officially denoted.
To increase the reproducibility, it was proposed that measurements were done in duplicate and a third measurement was to be made if the first two differed by more than 10%.
The present applications of NO measurement cover asthma diagnosis, monitoring, management, and treatment of asthma. Thus, the sensitivity of FeNO measurement at levels higher than 20 ppb in patients with symptoms suggestive of asthma has been shown to be 88%, with a negative predictive value of 92%.
With the appearance of cheaper portable handheld devices based on electrochemical sensing on the market, the possibility was contemplated to perform serial measurements to monitor disease activity and to steer asthma control, especially because it was demonstrated that the increase of FeNO precedes the decrease in peak expiratory flow rates.
Another lucrative possibility is to titrate the optimal maintenance dose of inhaled steroids.
Taken together, these applications held the promise to use FeNO to guide asthma management. However, a carefully designed study by Szefler and coworkers showed that the use of FeNO neither improved asthma control nor allowed reduction in the dose of inhaled glucocorticosteroid.
An important advantage of the method is related to the noninvasive nature and the simplicity of the FeNO measurement, which makes it applicable in children and even infants. The special promise in these youngest patients is held by the fact that there are virtually no objective measures to support the diagnosis and control of treatment in those younger than 5 years. Conclusive trials are still awaited to clearly demonstrate the benefit of FeNO measurements in the clinical setting.
Carbon Monoxide
Another gaseous constituent of exhaled breath is exhaled carbon monoxide (eCO), which has been initially suggested as a measure of oxidative stress. Its concentration in the exhaled breath derives from endogenous production by different tissues as a result of haem metabolism catalyzed by oxygenase enzymes.
It plays an important role as modulator of inflammation, cellular apoptosis, proliferation, and differentiation.
Carbon monoxide in the ambient air, which reflects air pollution from burning fossil fuels and tobacco smoking, influences its levels in the exhaled breath. It is measured with simple electrochemical methods by means of portable devices in the parts per million range. A recent meta-analysis assessing the value of eCO in asthma management concludes that eCO is elevated in asthmatic patients but that its levels only partially reflect disease severity and control.
Because of the confounding effect of tobacco smoking, eCO might be a potentially useful noninvasive biomarker of airway inflammation and oxidative stress ionsmoking asthmatic patients. A specifically designed study challenges its utility as one time point measurement but still assumes some benefit in longitudinal follow-up.
Indirect Measurements in Exhaled Breath Condensate
Most trace VOCs contained in exhaled breath currently cannot be directly measured because this requires the development of specific sensors with outstanding sensitivity and specificity. New opportunities have opened up by using ex haled breath condensate (EBC), obtained by cooling exhaled air, which contains water vapor and microdroplets. The composition of EBC is believed to reflect that of the airway epithelial lining fluid. The microdroplets are the actual carriers of the multitude of VOCs, but little is known about their formation and detachment from the airway walls during breathing. They are diluted in the resulting EBC between 5,000 and 25,000 times.
The condensation of the water vapors in exhaled breath is achieved by exhalation through simple cooling devices, making EBC collection totally noninvasive and consequently particularly easy to perform even in children with severe disease.
A technique has been developed to safely obtain EBC even from infants using a face mask connected to a cooling device. Influences confounding the accuracy of the measurements, such as smoking, alcohol consumption, equipment, exercise, mode and rate of breathing, nasal and salivary contamination, environmental temperature and humidity, and the nature of determination assays used, have been identified.
New techniques for diversifying the number of known biomarkers with increased detection threshold are already on the way. Recommendations have been recently published on how to collect EBC in an attempt to minimize differences due to sampling devices and collection protocols.
A large number of mediators have been measured in EBC, among which few have proven clinically useful. These can be grouped into biomarkers of oxidative stress, arachidonic acid metabolites, NO-related products, pH of the EBC, cytokines and chemokines, and proteins. A detailed overview of all the different components investigated in EBC has been recently published (Table 1). Some of these EBC biomarkers correlate with asthma severity, lung function impairment, and airway remodeling, and others hold promise as identifiers of specific asthma phenotypes, such as aspirin-sensitive asthma and exercise-induced asthma.
Despite the encouraging positive results to date, the introduction of EBC in everyday clinical practice requires the resolution of some methodologic pitfalls, the standardization of EBC collection, and finally the identification of the reliable biomarkers that are reproducible, have normal values, and provide information about the underlying inflammatory process and the response to treatment. An important issue to be resolved is finding a reliable approach to account for the dilution of the microdroplets by the water vapor in the exhaled air. Three candidate markers of dilution (urea, total cations, and conductivity of vacuum-treated EBC) have been introduced, with the assumption that concentrations of each indicator in the epithelial lining fluid are similar to those in the plasma. Accounting for the level of dilution of the EBC may help our judgment about the usability of certain markers of inflammation. Thus, measuring conductivity of vacuum-treated EBC samples to account for dilution resulted in a disappointing lack of differences between asthmatic patients and healthy controls for the potential candidates for airway inflammation biomarkers: adenosine and adenosine triphosphate.
The conclusion was that the relation between EBC mediator concentration and EBC conductivity highlights the importance of further standardization of the EBC method and the need for more studies to understand airway droplet formation. Drawbacks of EBC analysis derive from the fact that the concentrations of mediators in EBC are low, nearing the detection limit of currently available techniques, so more sensitive methods, such as high-performance liquid chromatography, negative ion chemical ionization mass spectrometry, gas chromatography–mass spectrometry, nuclear magnetic resonance–based spectroscopy, and field asymmetric ion mobility spectrometry, should be considered for this assay.
Furthermore, the anatomical sources of the compounds measured in EBC are not well defined, and most of the measurements are not done in real time.
INTEGRAL ASSESSMENT OF AIRWAY INFLAMMATION BY MEANS OF EXHALED BREATH
Exhaled Breath Temperature
The deep structures of the lung typically have temperatures representative of the body core. The temperatures are determined by the blood flowing along the rich vascular network of the alveoli. The temperature of the inhaled air is tempered during its flow in and out of the branching airways, which have a separate system of blood supply. Because blood is the main carrier of thermal energy maintaining the core body temperature, processes that would modify its flow within the airway walls might reflect on the exhaled breath temperature.
Several research teams have investigated the assumption that inflammation of the airways would influence the temperature of the air coming from the alveoli of the lungs and that this added signal could be picked by appropriate means.
In previous experiments it was demonstrated that in asthmatic adults and children there was correlation between the temperature of the exhaled breath and the bronchial blood flow, the FeNO levels, and the number of sputum eosinophils.
Although the first experiments were made in sealed chambers with sophisticated equipment requiring extensive training of the patients to take the measurements, a specially designed, handheld instrument was built that allowed measurements to be taken in regular indoor environments without special requirements from the tested patients. It proved successful in differentiating asthmatic from nonasthmatic patients and picked the improvement in the condition of patients treated with inhaled anti-inflammatory drugsand outlined the possibility of using this portable instrument for daily monitoring of airway correlating with parallel peak expiratory flow measurements.
Software improvements would make the device still friendlier to patients and physicians and would render the time for measurement minimal.
CAPNOGRAPHY
Capnography is the monitoring of the concentration or partial pressure of carbon dioxide (CO2) in the respiratory gases. Its main development has been as a monitoring tool for use during anaesthesia and intensive care. It is usually presented as a graph of expiratory CO2 plotted against time, or, less commonly, but more usefully, expired volume. The plot may also show the inspired CO2, which is of interest when rebreathing systems are being used.
The capnogram is a direct monitor of the inhaled and exhaled concentration or partial pressure of CO2, and an indirect monitor of the CO2 partial pressure in the arterial blood. In healthy individuals, the difference between arterial blood and expired gas CO2 partial pressures is very small. In the presence of most forms of lung disease, and some forms of congenital heart disease (the cyanotic lesions) the difference between arterial blood and expired gas increases and can exceed 1 kPa.
During anaesthesia, there is interplay between two components: the patient and the anaesthesia administration device (which is usually a breathing circuit and a ventilator). The critical connection between the two components is either an endotracheal tube or a mask, and CO2 is typically monitored at this junction. Capnography directly reflects the elimination of CO2 by the lungs to the anaesthesia device. Indirectly, it reflects the production of CO2 by tissues and the circulatory transport of CO2 to the lungs.
When expired CO2 is related to expired volume rather than time, the area beneath the curve represents the volume of CO2 in the breath, and thus over the course of a minute, this method can yield the CO2 minute elimination, an important measure of metabolism. Sudden changes in CO2 elimination during lung or heart surgery usually imply important changes in cardiorespiratory function.
Capnographs usually work on the principle that CO2 absorbs infra-red radiation. A beam of infra-red light is passed across the gas sample to fall on a sensor. The presence of CO2 in the gas leads to a reduction in the amount of light falling on the sensor, which changes the voltage in a circuit. The analysis is rapid and accurate, but the presence of nitrous oxide in the gas mix changes the infra-red absorption via the phenomenon of collision broadening. This must be corrected for. Measuring the CO2 in human breath by measuring its infra-red absorptive power was established as a reliable technique by John Tyndall in 1864, though 19th and early 20th century devices were too cumbersome for everyday clinical use.
Diagnostic usage
Capnography provides information about CO2 production, pulmonary (lung) perfusion, alveolar ventilation, respiratory patterns, and elimination of CO2 from the anaesthesia breathing circuit and ventilator. The shape of the curve is affected by some forms of lung disease; in general there are obstructive conditions such as bronchitis, emphysema and asthma, in which the mixing of gases within the lung is affected.
Conditions such as pulmonary embolism and congenital heart disease, which affect perfusion of the lung, do not, in themselves, affect the shape of the curve, but greatly affect the relationship between expired CO2 and arterial blood CO2. Capnography can also be used to measure carbon dioxide production, a measure of metabolism. Increased CO2 production is seen during fever and shivering. Reduced production is seen during anaesthesia and hypothermia.
Use in anaesthesia
Capnography has been shown to be more effective than clinical judgement alone in the early detection of adverse respiratory events such as hypoventilation, oesophageal intubation and circuit disconnection; thus allowing patient injury to be prevented. During procedures done under sedation, capnography provides more useful information, e.g. on the frequency and regularity of ventilation, than pulse oximetry.
Capnography provides a rapid and reliable method to detect life-threatening conditions (malposition of tracheal tubes, unsuspected ventilatory failure, circulatory failure and defective breathing circuits) and to circumvent potentially irreversible patient injury.
Capnography and pulse oximetry together could have helped in the prevention of 93% of avoidable anaesthesia mishaps according to an ASA (American Society of Anesthesiologists) closed claim study.
Capnography in emergency medical services
Capnography is increasingly being used by paramedics to aid in their assessment and treatment of patients in the prehospital environment. These uses include verifying and monitoring the position of an endotracheal tube. A properly positioned tube in the trachea guards the patient’s airway and enables the paramedic to breathe for the patient. A misplaced tube in the esophagus can lead to death.
A study in the March 2005 Annals of Emergency Medicine, comparing field intubations that used continuous capnography to confirm intubations versus non-use showed zero unrecognized misplaced intubations in the monitoring group versus 23% misplaced tubes in the unmonitored group. The American Heart Association (AHA) affirmed the importance of using capnography to verify tube placement in their 2005 CPR and ECG Guidelines.
The AHA also notes in their new guidelines that capnography, which indirectly measures cardiac output, can also be used to monitor the effectiveness of CPR and as an early indication of return of spontaneous circulation (ROSC). Studies have shown that when a person doing CPR tires, the patient’s end-tidal CO2 (ETCO2, the level of carbon dioxide released at the end of expiration) falls, and then rises when a fresh rescuer takes over. Other studies have shown when a patient experiences return of spontaneous circulation, the first indication is often a sudden rise in the ETCO2 as the rush of circulation washes untransported CO2 from the tissues. Likewise, a sudden drop in ETCO2 may indicate the patient has lost pulses and CPR may need to be initiated.
Paramedics are also now beginning to monitor the ETCO2 status of nonintubated patients by using a special nasal cannula that collects the carbon dioxide. A high ETCO2 reading in a patient with altered mental status or severe difficulty breathing may indicate hypoventilation and a possible need for the patient to be intubated.
Capnography, because it provides a breath by breath measurement of a patient’s ventilation, can quickly reveal a worsening trend in a patient’s condition by providing paramedics with an early warning system into a patient’s respiratory status. Clinical studies are expected into the uses of capnography in asthma, congestive heart failure, diabetes, circulatory shock, pulmonary embolus, acidosis, and other conditions, with potential implications for the prehospital use of capnography.
PULSE OXIMETRY\
Pulse oximetry is a simple non-invasive method of monitoring the percentage of haemoglobin (Hb) which is saturated with oxygen. The pulse oximeter consists of a probe attached to the patient’s finger or ear lobe which is linked to a computerised unit. The unit displays the percentage of Hb saturated with oxygen together with an audible signal for each pulse beat, a calculated heart rate and in some models, a graphical display of the blood flow past the probe. Audible alarms which can be programmed by the user are provided. An oximeter detects hypoxia before the patient becomes clinically cyanosed.
How does an oximeter work? A source of light originates from the probe at two wavelengths (650nm and 805nm). The light is partly absorbed by haemoglobin, by amounts which differ depending on whether it is saturated or desaturated with oxygen. By calculating the absorption at the two wavelengths the processor can compute the proportion of haemoglobin which is oxygenated. The oximeter is dependant on a pulsatile flow and produces a graph of the quality of flow. Where flow is sluggish (eg hypovolaemia or vasoconstriction) the pulse oximeter may be unable to function. The computer within the oximeter is capable of distinguishing pulsatile flow from other more static signals (such as tissue or venous signals) to display only the arterial flow.
Calibration and Performance. Oximeters are calibrated during manufacture and automatically check their internal circuits when they are turned on. They are accurate in the range of oxygen saturations of 70 to 100% (+/-2%), but less accurate under 70%. The pitch of the audible pulse signal falls with reducing values of saturation.
The size of the pulse wave (related to flow) is displayed graphically. Some models automatically increase the gain of the display when the flow decreases and in these the display may prove misleading. The alarms usually respond to a slow or fast pulse rate or an oxygen saturation below 90%. At this level there is a marked fall in PaO2 representing serious hypoxia.
In the following situations the pulse oximeter readings may not be accurate:
1. A reduction in peripheral pulsatile blood flow produced by peripheral vasoconstriction (hypovolaemia, severe hypotension, cold, cardiac failure, some cardiac arrhythmias) or peripheral vascular disease. These result in an inadequate signal for analysis.
2. Venous congestion, particularly when caused by tricuspid regurgitation, may produce venous pulsations which may produce low readings with ear probes. Venous congestion of the limb may affect readings as can a badly positioned probe. When readings are lower than expected it is worth repositioning the probe. In general, however, if the waveform on the flow trace is good, then the reading will be accurate.
3. Bright overhead lights in theatre may cause the oximeter to be inaccurate, and the signal may be interrupted by surgical diathermy. Shivering may cause difficulties in picking up an adequate signal.
4. Pulse oximetry cannot distinguish between different forms of haemoglobin. Carbo-xyhaemoglobin (haemoglobin combined with carbon monoxide) is registered as 90% oxygenated haemoglobin and 10% desaturated haemoglobin – therefore the oximeter will overestimate the saturation. The presence of methaemoglobin will prevent the oximeter working accurately and the readings will tend towards 85%, regardless of the true saturation.
5. When methylene blue is used in surgery to the parathyroids or to treat methaemoglobinaemia a shortlived reduction in saturation estimations is registered.
6. Nail varnish may cause falsely low readings. However the units are not affected by jaundice, dark skin or anaemia.
Pulse oximeters may be used in a variety of situations but are of particular value for monitoring oxygenation and pulse rates throughout anaesthesia. They are also widely used during the recovery phase. The oxygen saturation should always be above 95%. In patients with long standing respiratory disease or those with cyanotic congenital heart disease readings may be lower and reflect the severity of the underlying disease.
In intensive care oximeters are used extensively during mechanical ventilation and frequently detect problems with oxygenation before they are noticed clinically. They are used as a guide for weaning from ventilation and also to help assess whether a patient’s oxygen therapy is adequate. In some hospitals oximeters are used on the wards and in casualty departments. When patients are sedated for procedures such as endoscopy, oximetry has been shown to increase safety by alerting the staff to unexpected hypoxia.
Oximeters give no information about the level of CO2 and therefore have limitations in the assessment of patients developing respiratory failure due to CO2 retention. On rare occasions oximeters may develop faults and like all monitoring the reading should always be interpreted in association with the patient’s clinical condition. Never ignore a reading which suggests the patient is becoming hypoxic. There is no doubt that pulse oximetry is the greatest advance in patient monitoring for many years and it is hoped that their use will eventually become routine during anaesthesia and surgery world wide. Since pulse oximeters cost at least £1200 their purchase will depend mainly on economic considerations.


{kind=link}