A PHLEGMON OF ZYGOMATIC, TEMPORAL LOBE: CHARACTERISTICS OF ORIGIN, LOCALIZATION, CLINICAL COURSE, DIFFERENTIAL DIAGNOSIS, SURGICAL TREATMENT. A PHLEGMON BUCCAL, NEAR AURICULE-CHEWING, BEHIND JAW AREAS: CLASSIFICATION, CHARACTERISTICS OF, LOCALIZATION, CLINICAL COURSE, DIFFERENTIAL DIAGNOSIS, SURGICAL TREATMENT.
Zygomatic process of temporal bone

Left temporal bone. Outer surface. Showing the zygomatic process projecting to the left side of the bone
Articulation of the mandible. Lateral aspect. (Zygomatic process visible at center.)
The zygomatic process of the temporal bone is a long, arched process projecting from the lower part of the squamous portion of the temporal bone. It articulates with the zygomatic bone.
This process is at first directed lateralward, its two surfaces looking upward and downward; it then appears as if twisted inward upon itself, and runs forward, its surfaces now looking medialward and lateralward.
Borders
The superior border is long, thin, and sharp, and serves for the attachment of the temporal fascia.
The inferior border, short, thick, and arched, has attached to it some fibers of the masseter.
Surfaces
The lateral surface is convex and subcutaneous.
The medial surface is concave, and affords attachment to the masseter.
Ends
The anterior end is deeply serrated and articulates with the zygomatic bone.
Zygomatic bone
Left zygomatic bone in situ.
In the human skull, the zygomatic bone (cheekbone, malar bone) is a paired bone which articulates with the maxilla, the temporal bone, the sphenoid bone and the frontal bone. It is situated at the upper and lateral part of the face and forms the prominence of the cheek, part of the lateral wall and floor of the orbit, and parts of the temporal and infratemporal fossa. It presents a malar and a temporal surface; three processes, the frontosphenoidal, orbital, maxillary, and temporal; and four borders.
The posterior end is connected to the squama by two roots, the anterior and posterior roots.
The posterior root, a prolongation of the upper border, is strongly marked; it runs backward above the external auditory meatus, and is continuous with th.
The anterior root, continuous with the lower border, is short but broad and strong; it is directed medialward and ends in a rounded eminence, the articular tubercle (eminentia articularis).s if twisted inward upon itself, and runs forward, its surfaces now looking medialward and lateralward.
Etymology
The term zygomatic derives from the Greek zygoma meaning “yoke”. The zygomatic bone is occasionally referred to as the zygoma, but this term may also refer to the zygomatic arch. The zygomatic is homologous to the jugal bone of other tetrapods.
Ossification
The zygomatic bone is generally described as ossifying from three centers— one for the malar and two for the orbital portion; these appear about the eighth week and fuse about the fifth month of fetal life.
Mall describes it as being ossified from one center which appears just beneath and to the lateral side of the orbit.
After birth, the bone is sometimes divided by a horizontal suture into an upper larger, and a lower smaller division.
In some quadrumana the zygomatic bone consists of two parts, an orbital and a malar.
Surfaces
The malar surface is convex and perforated near its center by a small aperture, the zygomaticofacial foramen, for the passage of the zygomaticofacial nerve and vessels; below this foramen is a slight elevation, which gives origin to the Zygomaticus.
The temporal surface, directed posteriorly and medially, is concave, presenting medially a rough, triangular area, for articulation with the maxilla (articular surface), and laterally a smooth, concave surface, the upper part of which forms the anterior boundary of the temporal fossa, the lower a part of the infratemporal fossa. Near the center of this surface is the zygomaticotemporal foramen for the transmission of the zygomaticotemporal nerve.
Processes
Each zygomatic bone is diamond-shaped and composed of three processes with similarly named associated bony articulations: frontal, temporal, and maxillary. Each process of the zygomatic bone forms important structures of the skull.
The orbital surface of the frontal process of the zygomatic bone forms the anterior lateral orbital wall, with usually a small paired foramen, the zygomaticofacial foramen opening on its lateral surface. The temporal process of the zygomatic bone forms the zygomatic arch along with the zygomatic process of the temporal bone, with a paired zygomaticotemporal foramen present on the medial deep surface of the bone. The orbital surface of the maxillary process of the zygomatic bone forms a part of the infraorbital rim and a small part of the anterior part of the lateral orbital wall.
Borders
The antero-superior or orbital border is smooth, concave, and forms a considerable part of the circumference of the orbit.
The antero-inferior or maxillary border is rough, and bevelled at the expense of its inner table, to articulate with the maxilla; near the orbital margin it gives origin to the Quadratus labii superioris.
The postero-superior or temporal border, curved like an italic letter f, is continuous above with the commencement of the temporal line, and below with the upper border of the zygomatic arch; the temporal fascia is attached to it.
The postero-inferior or zygomatic border affords attachment by its rough edge to the Masseter.
Articulations
The zygomatic articulates with four bones: the frontal, sphenoidal, temporal, and maxillae.
Pterygomandibular Abscess
Anatomic Location. This space is bounded laterally by the medial surface of the ramus of the mandible, medially by the medial pterygoid muscle, superiorly by the lateral pterygoid muscle, anteriorly by the pterygomandibular raphe, and posteriorly by the parotid gland.
The pterygomandibular space contains the mandibular neurovascular bundle, lingual nerve, and part of the buccal fat pad. It communicates with the pterygopalatal, infratemporal, submandibular,
and lateral pharyngeal spaces.
Etiology. An abscess of this space is caused mainly by infection of mandibular third molars or the result of an inferior alveolar nerve block, if the penetration site of the needle is infected (pericoronitis).
Clinical Presentation. Severe trismus and slight extraoral edema beneath the angle of the mandible are observed. Intraorally, edema of the soft palate of the affected side is present, as is displacement of the uvula and lateral pharyngeal wall, while there is difficulty in
swallowing.
Treatment. The incision for drainage is performed on the mucosa of the oral cavity and, more specifically, along the mesial temporal crest.
The incision must be 1.5 cm long and 3–4 mm deep. A curved hemostat is then inserted, which proceeds posteriorly and laterally until it comes into contact with the medial surface of the ramus. The abscess is drained, permitting the evacuation of pus along the shaft of the
instrument.
Infratemporal Abscess
Anatomic Location. The space in which this abscess develops is the superior extension of the pterygomandibular space. Laterally, this space is bounded by the ramus of the mandible and the temporalis muscle, while medially, it is bounded by themedial and lateral pterygoid muscles, and is continuous with the temporal fossa/
Important anatomic structures, such as the mandibular nerve, mylohyoid nerve, lingual nerve, buccal nerve, chorda tympani nerve, and
the maxillary artery, are found in this space. Part of the pterygoid venous plexus is also found inside this space.
Etiology. Infections of the infratemporal space may be caused by infected root canals of posterior teeth of the maxilla and mandible, by way of the pterygomandibular space, and may also be the result of a posterior superior alveolar nerve block and an inferior alveolar
nerve block.
Clinical Presentation. Trismus and pain during opening of the mouth with lateral deviation towards the affected side, edema at the region anterior to the ear which extends above the zygomatic arch, as well as edema of the eyelids are observed.
Treatment. The incision for drainage of the abscess is made intraorally, at the depth of the mucobuccal fold, and, more specifically, laterally (buccally) to the maxillary third molar and medially to the coronoid process, in a superoposterior direction.
A haemostat is inserted into the suppurated space, in a superior direction. Drainage of the abscess may be
performed extraorally in certain cases. The incision is performed on the skin in a superior direction, and extends approximately 3 cm. The starting point of the incision is the angle created by the junction of the frontal and temporal processes of the zygomatic bone. Drainage of the abscess is achieved with a curved hemostat, which is inserted through the skin into the
purulent accumulation.
Temporal Abscess
Anatomic Location. The temporal space is the superior continuation of the infratemporal space. This space is divided into superficial and deep temporal spaces. The superficial temporal space is bounded laterally by the temporal fascia andmedially by the temporalismuscle, while the deep temporal space is found between the medial surface of the temporalis muscle and the temporal bone. The spread of infection from the infratemporal space,
with which it communicates.
Clinical Presentation. It is characterized by painful edema of the temporal fascia, trismus (the temporalis and medial pterygoid muscles are involved), and pain during palpation of the edema.
Treatment. The incision for drainage is performed horizontally, at the margin of the scalp hair and approximately 3 cm above the zygomatic arch. It then continues carefully between the two layers of the temporal fascia as far as the temporalis muscle. A curved hemostat is used to drain the abscess.
Buccal Space Abscess
Anatomic Location. The space in which this abscess develops is between the buccinator and masseter muscles.
Buccal space abscess. Diagrammatic illustration showing the spread of an abscess lateral to the buccinator muscle.
Superiorly, it communicates with the pterygopalatine space; inferiorly with the pterygomandibular space. The spread of pus in the buccal space depends on the position of the apices of the responsible teeth relative to the attachment of the buccinators muscle.
Etiology. The buccal space abscess may originate from infected root canals of posterior teeth of the maxilla and mandible.
Clinical Presentation. It is characterized by swelling of the cheek, which extends from the zygomatic arch as far as the inferior border of the mandible, and from the anterior border of the ramus to the corner of the mouth. The skin appears taut and red, with or without fluctuation of the abscess, which, if neglected, may result in spontaneous drainage.
Treatment. Access to the buccal space is usually intraoral for three main reasons:
1. Because the abscess fluctuates intraorally in the majority of cases.
2. To avoid injuring the facial nerve.
3. For esthetic reasons.
The intraoral incision is made at the posterior region of the mouth, in an anteroposterior direction and very carefully in order to avoid injury of the parotid duct. A hemostat is then used to explore the space thoroughly. An extraoral incision is made when intraoral abccess
would not ensure adequate drainage, or when the pus is deep inside the space. The incision is made approximately 2 cm below and parallel to the inferior border of the mandible.
Parotid Space Abscess
Anatomic Location. The space in which this abscess develops is located in the area of the ramus of the mandible and, more specifically, between the layers of the fascia investing the parotid gland. It communicates with the lateral pharyngeal and the submandibular
spaces. It contains the parotid gland and its duct, the external carotid artery, the superficial
temporal and facial artery, the retromandibular vein, the auriculotemporal nerve, and the facial nerve.
Etiology. Infection of this space originates from odontogenic migratory infections of the lateral pharyngeal and submandibular spaces.
Clinical Presentation. It presents with characteristic edema of the retromandibular and parotid region, difficulty in swallowing and pain mainly during chewing, which radiates to the ear and temporal region. In certain cases there is redness of the skin and subcutaneous fluctuation.
Also, a purulent exudatemay be noted fromthe papilla of the parotid duct after pressure is applied.
Treatment. Depending on the margins of the edema, therapy entails a broad incision posterior to the angle of the mandible, taking particular care not to injure the respective branch of the facial nerve. Drainage of pus is achieved after blunt dissection using a hemostat to explore the purulent collection.
Submasseteric Abscess
Anatomic Location. The space in which this abscess develops is cleft-shaped and is located between the massetermuscle and the lateral surface of the ramus of the mandible.
Posteriorly it is bounded by the parotid gland, and anteriorly it is bounded by the mucosa of the retromolar area.
Etiology. Infection of this space originates in the mandibular third molars (pericoronitis), and in rare cases because of migratory abscesses.
Clinical Presentation. It is characterized by a firm edema that is painful to pressure in the region of the masseter muscle, which extends from the posterior border of the ramus of the mandible as far as the anterior border of the masseter muscle.
Also, severe trismus and an inability to palpate the angle of the mandible are observed. Intraorally, there is edema
present at the retromolar area and at the anterior border of the ramus. This abscess rarely fluctuates, while it may present generalized symptoms.
Treatment. Treatment of this abscess is basically intraoral, with an incision that begins at the coronoid process and runs along the anterior border of the ramus towards the mucobuccal fold, approximately as far as the second molar. The incision may also be performed extraorally on the skin, beneath the angle of the mandible.
In both cases, a hemostat is inserted, which proceeds as far as the center of suppuration and until it comes into contact with bone.
Because access is distant from the purulent accumulation,
often it is difficult to drain the area well, resulting in frequent relapse.
Submandibular Abscess
Anatomic Location. The submandibular space is bounded laterally by the inferior border of the body of the mandible, medially by the anterior belly of the digastric muscle, posteriorly by the stylohyoid ligament and the posterior belly of the digastric muscle, superiorly by the mylohyoid and hyoglossus muscles, and inferiorly by the superficial layer of the deep cervical fascia.
This space contains the submandibular salivary gland and the submandibular lymph nodes.
Etiology. Infection of this space may originate from the mandibular second and third molars, if their apices are found beneath the attachment of the mylohyoidmuscle. It may also be the result of spread of infection from the sublingual or submental spaces.
Clinical Presentation. The infection presents as moderate swelling at the submandibular area, which spreads, creating greater edema that is indurated and redness of the overlying skin.
Also, the angle of the mandible is obliterated, while pain during palpation and moderate trismus due to involvement of the medial pterygoid muscle are observed aswell.
Treatment. The incision for drainage is performed on the skin, approximately 1 cm beneath and parallel to the inferior border of the mandible.
During the incision, the course of the facial artery and vein (the incision should be made posterior to these) and the respective branch of the facial nerve should be taken into consideration. A hemostat is inserted into the cavity of the abscess to explore the space and an attempt is made to communicate with the infected spaces.
Blunt dissection must be performed along the medial surface of the mandibular bone also, because pus is often located in this area as well. After drainage, a rubber drain is placed.
Phlegmon of the face and neck
Introduction: Phlegmon of the face and neck constitutes the most serious of inflammatory conditions of this area, if the rarest. It develops rapidly and is characterized by a varied clinical picture and may give rise to life-threatening complications such as airways obturation, descending mediastinitis, metastatic abscess, thrombophlebitis, haemorrhage with disseminated intravascular coagulation, septic shock with circulatory and respiratory failure. Aim of the study: To discuss the therapeutic management of patients with phlegmon of the face and neck on the basis of own clinical material.
Material and methods: Case histories of three patients who were treated for phlegmon of the face and neck in the Maxillofacial Surgery Clinic,
Conclusion: Immediate treatment with targeted antibiotic therapy, wide incisions to allow flow drainage of the cervical area and causal treatment offer good prognosis. The treatment has long duration and the clinical picture may vary with a possibility of exacerbation and remission.
Introduction
Face and neck phlegmons belong to the most severe inflammatory conditions of this region but also to the least common. There are usually single reports, mostly by laryngologists. The causes of phlegmons include: peritonsillar abscess, tooth gangrene, facial bone fractures, postoperative wound complications, purulent cysts, lymph nodes inflammation, purulent skin changes, inflammatory conditions of the mastoid process bone, posterior pharynx wall injury after tonsillectomy, salivary glands inflammation and sometimes the cause is not identified .
There has even been published a case of oral cavity floor phlegmon complicated by partial tongue necrosis as an outcome of pharynx inflammation and a fatal case of purulent glottis inflammation leading to thoracic phlegmon accompanied by septic shock.
Factors prediposing to this kind of inflammation are: diabetes, immunosuppresant treatment, HIV infections, alcoholism or gamma globulin deficiency. However, very often it is impossible to determine conclusively what causes fast clinical spread of phlegmon in patients with no systemic diseases.
It is assumed that the bacterial agent is mixed flora. In gas phlegmon the gas in soft tissues with characteristic crepitation is formed owing to anaerobic flora and staphylococci, whereas in gas gangrene
– Clostridium bacilli are cultured.
Head and neck localization of gas gangrene constitutes only 2.4% of cases. Different authors emphasize rapid course of the disease, the necessity for interdisciplinary cooperation of many specialists. The therapy, apart from targeted antibiotic therapy, includes surgery with wide incisions and flow drainage of the
neck area, adjuvant treatment (especially immunoglobulin) and hyperbarium oxygen therapy at 2,5 atm.
Phlegmon spreads from the parapharyngeal space along the intrafascial spaces or the internal carotid artery and internal carotid vein to the anterior mediastinum; from the retropharyngeal space along the easophagus to the posterior mediastinum.There is also a possibility of bloodborne and lymphatic vessel route of spread of the disease. There has been a rare report of the abscess formation in lumbosacral region being a complication of the spread of suppurative process via fasciae and fissures between them as far as the palatine tonsil and parapharyngeal space. Mortality in the case of phlegmon with fascial necrosis is from 19.2% to 40% and in the most severe course of disease can even lead to septic shock with DIC syndrome. There are indications for ultrasound and computed tomography examination in phlegmon. Although CT does not always differentiate the causes, it indicates the presence of gas and purulent content in the tissues, spread routes of the infiltration, localization of drains, enables the monitoring of the scope and course of the disease . As this kind of inflammation is uncommon and has a rapid course and a high mortality risk, we wish to present three documented cases of patients treated with good results in the Department of Maxillofacial Surgery of the
Conclusion
Immediate treatment including surgical incision for drainage and antibiotic therapy was successful. Attention should be drawn to a variety of clinical symptoms and a possibility of exacerbation and remission.
Acute inflammation of the parotid gland from the phlegmon podmasseterialnoy distinguished first of all border swelling corresponding to the topography of cancer, that is, beyond masseter to the earlobe, mastoid process, and for lower edge of the lower jaw. In addition, when mumps infiltration does not reach the front edge of the chewing muscles, mouth opening less painful and limited. Often marked hyperemia of duct and serous-purulent discharge from it, mucosal edema lateral pharyngeal wall.
For recognition of suppurative lymphadenitis of the parotid or false mumps, and inflammation supramandibulyarnyh nodes is very important etiological moment. In most cases it is possible to identify past or current focus of inflammation in areas from which go way to the regional lymph glands. According to research by S. Nekrasov (1938), parotid gland lymph comes from lateral parts of the face, the buccal mucosa, tongue, eyeballs, skin front of the scalp, ear, indigenous lower teeth of the gland itself and mastoid sites.
Iadchelyustnye infection enters the lymph glands, as indicated by NN Lavrov (1949), AI Evdokimov (1959), SI and IP Bardysheva Legoshin (1965), inflammatory lesions of the lower premolars and molars, masseter, with stomatitis, periodontal disease, mucosal abrasions. Kositsyn II (1963) observed supramandibulyarnye lymphadenitis in lesions of salivary glands, skin diseases temple, nose, lower lip, tonsil, upper jaw.
In a survey, most patients say that the disease began with the appearance of a small painful nodule in front of the ear false mumps or bottom cheeks at nadchelyustnyh phlegmonous adenitis or abscess. Then about the site appeared painful swelling. Unlike podmasseterialnyh phlegmon flushed skin and thickening are limited and do not reach the limits masseter. Infiltrate more mobile, painful, and softening observed in a small area. The reduction of the jaws is weak. The general reaction, leukocytosis and change hemogram insignificant.
Inflammation of the temporomandibular jaw joint in the dominant symptom podmasseterialnogo purulent process should not be an excuse to diagnostic errors. Unexpressed pain symptom of joint tenderness and outside of the ear canal, as well as the pressure on the chin backwards and at the physiological load eliminates acute arthritis.
The possibility of mistaken diagnosis podmasseterialnoy phlegmon at festering cysts of different etiologies in the angle of the lower jaw, accompanied by swelling of the parotid jet-chewing area. However, the argument against podmasseterialnoy cellulitis is a painful lack of on-site infiltration of chewing muscles, bone deformity and radiographic data.
Particular difficulties encountered in the diagnosis of running podmasseterialnyh phlegmon, when simultaneously revealed phlegmonous processes of other related areas. According to our data, they are most often combined with phlegmons cheeks, infratemporal fossa, submandibular triangle and rare — with phlegmons pozadichelyustnoy pterygopalatine fossa and the jaw-space. A clear understanding of the basic symptoms podmasseterialnoy cellulitis and abscess combined process enables the diagnosis and determine the extent of surgical intervention.
Thus, knowledge of clinic podmasseterialnoy cellulitis and extensive differentiation of it from other acute inflammatory diseases will allow early diagnosis, to conduct effective therapy and reduce the number of serious complications.
When podmasseterialnyh phlegmon edematous tissue and infiltrated by the outer surface of the angle of the mandible and the branches, mostly in place masseter. During clenching jaws infiltrate like “hiding” behind the muscle. By inflammatory changes in tissue is thickened and rounded bottom edge of the bone and masseter front. Observed persistent trismus. Reveals a sharp pain on the pressure posterior to the muscle of the arches of the mouth, and here at the bimanual palpation is often felt fluctuation.
In contrast, the periostitis and osteomyelitis of the phenomenon of acute inflammation to contain, as a rule, do not fit within the boundaries of chewing muscles, and focus mainly on the outer surface of the bone. Accordingly, the location of a purulent focus pronounced swelling and redness of the gums and surrounding areas cheeks bulging transition smoothness and wrinkles. Tissue infiltrated in the vault arches of the mouth or in the circle of bone for causal or more adjacent, sometimes lyuksiruyuschih teeth. Less dramatic reduction of the jaws. Often violated sensitivity in the area of innervation mental nerve. The front edge of the masseter is not changed, palpation it backwards or maloboleznenna painless. Puncture pus cavity is not determined by the chewing muscles, which often happens when podmasseterialnyh phlegmon.
On the basis of diagnostic errors, podmasseterialnye cellulitis should be distinguished from some other admaxillary phlegmons primarily with phlegmon cheeks and pozadichelyustnoy fossa.
The difference between not running podmasseterialnymi phlegmon and phlegmons cheek is swelling that often goes past the edge of the zygomatic arch, there is a swelling of the infraorbital region and age, smoothness nasolabial folds. Defined cheeks bulging outwards or in the mouth and sharply painful infiltration front chewing muscles. In parotid-chewing region has only been reactive edema. While trying to open his mouth lower jaw does not move in a sick way, it can be noted in podmasseterialnyh phlegmon.
Phlegmon pozadichelyustnoy pits characterized the main focus of purulent inflammation of posterior masseter. Swelling and redness of the skin, and sometimes, painful infiltration of tissues expressed the corner jaw. Head and neck movement is limited, painful, sometimes marked pain on swallowing. The main symptoms of cellulitis podmasseterialnoy — sharp pain swelling in the chewing muscles and persistent trismus — no.
Differentiating podmasseterialnuyu phlegmon, do not forget the chewing-phlegmon parotid area that emit D. Vasiliev (1963) and P. Egorov (1961). To her authors include suppurative processes of cellular spaces but the outer surface of the posterolateral branch of the upper jaw and recommend its typical open cut at an angle of the jaw to the bundle of tissue on the outer surface of the bone. A distinctive feature of these phlegmon podmasseterialnyh is more diffuse swelling extending to the cheek and temple, beyond the fascial attachment box chewing muscles to the zygomatic arch. Along the zygomatic arch to the swelling groove eye gap narrowed rear edge contours chewing muscles are not defined, lockjaw first degree. Swelling of the upper arch arches of the mouth can move on krylochelyustnuyu crease. The front edge of the masseter somewhat infiltrated. Expressed general intoxication. We attribute this to the phlegmon podmasseterialnogo phlegmon of the upper space.
Perikoronarity as a complication of tooth eruption hindered “wisdom” occur with inflammatory changes in the tissues surrounding the crown of the tooth, swelling in the chewing and pterygoid muscles and cheeks, with sero-purulent discharge from under the hood or ulceration of it. Trismus expressed less chewing muscle almost not changed.
A Case of Phlegmon of Cheek Complicate with Severe Diabetes.
Title: A Case of Phlegmon of Cheek Complicate with Severe Diabetes.
Author: TAKAHIRO MIYASAKA; MUNEKAZU SUZUKI; TAKAHISA YAMADA; TAZUKO SATOH (The Nippon Dental University, School of Dentistry at Tokyo, Department of Oral and Maxillofacial Surgery I)
Source: ORAL THERAPEUTICS AND PHARMACOLOGY; ISSN:0288-1012; VOL.14; NO.1; PAGE.47-52; (1995)
Pub.Country: Japan
Language: Japanese
Abstract: A case of temporal abscess due to advanced phlegmon of cheek complicated with severe diabetes mellitus was diagnosed at our department. Diabetes was diagnosed in a 38-year old male at the age of 23 ; this patient had received therapy but later discontinued it.
He was slightly flushed and showed diffuse swelling from the area below the left mandible to the cheek caused by the 3rd molar of the left mandible. Mild rubefaction, heat sensation, pain and difficulty in opening his mouth were noted. Diffuse swelling, floridity and pain were focused on the molar region of the left mandible.
According to clinical examination performed during the initial consultation, the following results were obtained ; leukocyte count : 127×102/μl, blood sedimentation : 89mm/1h, CRP : 2+, blood sugar : 483mg/dl, urine sugar : > 1000mg/dl (4+), ketone body : 100mg/dl (3+), HbA1c : 11.9%, and HbA1 : 13.7%.
The patient was hospitalized and received ASPC intravenous drip infusion and he was placed on insulin therapy and a diabetic diet.
On the day after his admission, under local anesthesia, an intraoral incision was made for drainage. The drug sensitivity test performed on the 14th day after his admission showed a negative reaction to ASPC.There fore ASPC was replaced with FMOX. A left temporal abscess gradually formed and a drainage incision was made on the 18th day.
These therapeutic techniques failed to stabilize the blood sugar level and accelerated the local inflammatory symptoms. In order to improve these symptoms, a higher dose of insulin was administered. The causative tooth was extracted on the 21st day and anaerobic bacteria were detected on the 23rd day. PAPM/BP and FMOX were administered to extend the antimicrobial spectrum.
On the 26th day, formation of a temporal abscess was observed, so incisional drainage and removal of the necrotic tissues by incision were performed.
On the basis of a roentgenolography and a bone scintigraphy, a diagnosis of osteomyelitis of the left mandible was made. On the 61st day, under general anesthesia, the left mandible was scraped out after extraoral skin incision. From the 69th day on, the inflammatory symptoms improved and LAPC was orally administered.
After this surgery, insulin therapy was terminated because his blood sugar level dropped to under 200mg/dl.
He has been in satisfactory condition for seven months postoperatively.
Deep face and neck infections are potentially life threatening if they are not diagnosed in time and then treated quickly. This report describes a case of face and deep neck infection, associated with a semi-impacted and decayed wisdom tooth in a cardiopathic, immunosuppressed patient suffering from, diabetes, hypothyroidism, osteoporosis, breathlessness, chronic bronchitis, with oral, cutaneous and vaginal erythematous lichen, Cushing’s Syndrome, penicillin allergy, subjected to past hypophysectomy. The swelling was, first of all, treated in urgency, with an intravenous antibiotic therapy and, immediately afterwards, the phlegmonous infiltration linked to the avulsion of the lower third molar was surgically drained. The patient was then treated with intravenous multiple antibiotics, with the aim of eradicating the predominating bacteria that was encountered in the microbiological culture test. A complete remission of the pathological picture was obtained .
Summary: Herein we present five cases of submasseteric abscess that most commonly occurred in patients with a history dental disease. CT has been the main imaging method for diagnosing lesions in the masticator space and adjacent to the mandible; however, we found that, in some of our cases, CT defined the lesion poorly or not at all. In some cases, MR imaging defined the lesion better. Radiologic manifestations of this condition and pathologic correlations are discussed.
Submasseteric abscess is a localized, often chronic, infection between the masseter and the mandible. This location is normally only a potential space but provides a protected space for the development of an occult abscess. Although cases of submasseteric abscess have been reported in the otolaryngologic and dental literature, the findings associated with infection in the submasseteric space have not, to our knowledge, been analyzed in the radiologic literature. Most of the patients in this series presented with chronic symptoms and were initially misdiagnosed. The delay in treatment was several years in some cases. The radiologic findings can be subtle, especially in more chronic cases. We present five cases of submasseteric abscess with CT and MR imaging findings. The radiologic manifestations of this uncommon entity and pathologic correlatioeed to be understood so that appropriate treatment is not delayed.
Cases Reports
Five cases of submasseteric abscess were obtained from teaching files of the senior authors (A.J.S., L.M.) over the past 10 years. Three patients were women and two men with an age range of 16–50 years. Clinical information was obtained from the referring physician or the patient and supplemented by hospital records. Imaging was performed at our institution and also at outside hospitals. Four of the cases were surgically confirmed. In one case (patient 4), no surgery was performed and the diagnosis was not pathologically confirmed. Because of convincing clinical and imaging findings, however, the case is included.
Patient 1
This patient developed facial swelling and trismus approximately 6 months after removal of a lower left third molar. A diagnosis of infection was not made after initial CT and sialography; however, subtle signs of chronic infection were present on the initial CT examination, including diffuse thickening of the masseter, suggesting myositis, and sclerosis of the mandibular ramus, compatible with an adjacent chronic inflammatory process (Fig 1A). Symptoms persisted for 6 months, and repeat CT performed after intravenous administration of contrast material showed progression of the previous findings of myositis and sclerosis (Fig 1B).
View larger version:
· Download as PowerPoint Slide
FIG 1.
Patient 1.
A, Noncontrast axial CT image shows myositis of the left masseter muscle with diffuse swelling, but without significant surrounding inflammatory change or definite fluid collection. The parotid gland is normal.
B, Six months later, postcontrast axial CT image shows increased masseteric swelling and mandibular sclerosis with a discrete area of low attenuation (black arrow) with probable rim enhancement, suggesting the presence of an abscess.
Patient 2
After removal of a left lower molar, the patient developed left facial swelling. She received antibiotics, but facial swelling increased over 1 week accompanied by trismus. On presentation at this hospital, the patient was unable to open her mouth more than 3 mm. CT (Fig 2) showed diffuse thickening of the left masseter muscle without focal fluid collection. Bone windows showed early sclerosis of the mandibular ramus. Intraoral incision and drainage yielded 15 mL of purulent material. Eventually, the patient developed osteomyelitis of the mandible that required further treatment.
View larger version:
· Download as PowerPoint Slide
FIG 2.
Patient 2. Noncontrast axial CT image, soft-tissue view, shows diffuse thickening of the left masseter muscle with a suggestion of cortical thickening of the left mandibular ramus.
Patient 3
This patient developed spontaneous facial swelling. There was no history of dental symptoms or procedures. Because of trismus increasing over 2 months, the patient sought medical attention. Physical examination showed diffuse swelling in the right masseteric region. Palpation revealed a mildly tender, firm, nonfluctuant mass. There was no fever or leukocytosis. The presumptive diagnosis was parotitis. Dental radiographs at presentation showed an impacted third mandibular molar with a large follicular cyst. CT showed diffuse thickening of the masseter muscle, compatible with myositis, and a small focus of low attenuation, possibly representing a fluid collection (Fig 3). At surgery, a transoral approach to the submasseteric space yielded 2 mL of purulent material from an infected dentigerous cyst, which had ruptured through the buccal side of the mandible. Cultures yielded findings of Streptococcus viridans.
View larger version:
· Download as PowerPoint Slide
FIG 3.
Patient 3. Postcontrast axial CT image shows diffuse thickening of the left masseter muscle with a small, low-attenuation area, but without clear rim enhancement, possibly representing an abscess. Bony sclerosis of the mandibular ramus is present with a focus of cortical disruption of the mandible laterally (better seen on bone windows) at the level of the abscess.
Patient 4
A 17-year-old previously healthy female patient developed spontaneous facial swelling. After several months, the right lower third molar was removed. The swelling persisted without fever or trismus. MR imaging obtained several months later at an outside institution showed a fluid collection beneath the right masseter (Fig 4A–C). There was also sclerosis of the right mandibular ramus with masseteric thickening. The findings were compatible with chronic submasseteric abscess. No surgery was performed, and the patient continued to have episodic facial swelling with a variable response to antibiotics. The infection may have begun as a pericoronitis around a partially erupted tooth or as an infection associated with an unerupted tooth, but the abscess was not surgically confirmed.
View larger version:
· Download as PowerPoint Slide
FIG 4.
Patient 4.
A, Axial spin-echo T1-weighted image (500/20 [TR/TE]; number of signals averaged [NSA], 2256 × 224; section thickness, 5 mm) shows enlargement of the right masseter muscle with a subjacent curvilinear collection of low signal intensity believed to represent pus.
B, Axial fast spin-echo T2-weighted image (7100/125; NSA, 2; matrix, 256 × 224; section thickness, 5 mm) shows an elliptical mild high signal intensity zone lateral to the mandible corresponding to the low signal intensity seen on the T1 image and consistent with pus. Higher signal intensity between this collection and the masseter muscle probably represents edema and myositis.
C, Coronal spin-echo T1-weighted image (450/20; NSA, 2; matrix, 256 × 256; section thickness, 5 mm) shows thickening of the right mandibular ramus with low signal intensity within the marrow cavity consistent with cortical thickening and sclerosis of the marrow space.
Patient 5
A 43-year-old female patient had an 18-month history of episodic right facial swelling and fever that first occurred 3 weeks after multiple mandibular injections of local anesthesia for a dental procedure. A presumptive diagnosis of parotitis was made. The initial swelling subsided after a course of antibiotics, but swelling recurred many times with temporary improvement on administration of antibiotics. No significant pain, but a variable amount of trismus, was present throughout this period. Physical examination revealed no evidence of dental disease or mucosal inflammation. There was no fever or elevated white blood cell count. CT showed diffuse thickening of the right masseter muscle with subjacent region of heterogeneous attenuation, possibly representing a fluid collection. Sclerosis of the mandibular marrow cavity was also present (Fig 5A). MR imaging acquired without administration of contrast material showed focal high signal intensity on the T2-weighted images, findings compatible with an abscess, with low signal intensity in the marrow space (Fig 5C). Transoral surgery revealed purulent green material in an abscess, along with yellow granules compatible with sulfur produced by actinomyces. The organism, however, failed to grow in culture.
View larger version:
· Download as PowerPoint Slide
FIG 5.
Patient 5.
A, Postcontrast axial CT image shows diffuse thickening of the right masseter muscle with a region of mildly low attenuation posteromedially.
B, T2-weighted axial MR imaging shows a more definite fluid collection posteriorly as well as a region of high signal intensity anteriorly within the right masseter muscle compatible with edema and myositis.
C, Noncontrast coronal T1-weighted image shows T1 shortening within the collection, which is mildly hyperintense relative to muscle. This probably represents proteinaceous fluid.
Discussion
Anatomy
In 1948, Bransby-Zachary (1) first described the submasseteric space. In an effort to explain normal explorations of suspected parotid infections, he undertook cadaveric dissections. Previously, the masseter was said to have a broad, continuous insertion on the lateral aspect of the ramus of the mandible, but he found a bare area between separate attachments of deep and middle portions of the masseter muscle resulting in a potential space. Infection from a posterior molar could track posteriorly and become sequestered there as an abscess, thereby explaining the clinical findings.
The submasseteric space, a subdivision of the masticator space (2–4), results from a division of the masseter muscle into three parts: superficial, middle, and deep. All three parts originate on the zygomatic arch. Bransby-Zachary found that the insertion of a small, deep portion was limited to the lateral surface of the coronoid process and upper third of the ramus of the mandible. Insertion of the largest, superficial portion was restricted to the lower third of the ramus, especially posteriorly at the angle of the mandible. The middle portion was the smallest and inserted along a thin line curving posteriorly and superiorly over the middle third of the ramus (Fig 6) (1).
View larger version:
· Download as PowerPoint Slide
FIG 6.
Original drawing by Bransby-Zachary illustrating the insertions of the masseter (reproduced with the permission of British Dental Journal 1948; 84:10–13).
Although MacDougall (5, 6) dissected 141 cadavers and could not find a discrete submasseteric space, he reported an area of loose attachment between the middle and deep layers of the muscle that could present an incomplete barrier to infection and thereby provide a potential space for abscess formation. The presence of such a potential space along the ramus of the mandible between the insertions of the masseter muscle has been confirmed by one of the authors (L.M.) (Fig 6).
Imaging Characteristics
Although to our knowledge there are no reported cases of infection beneath the masseter muscle in the radiologic literature (2, 3, 7–10), there are many such reports in the dental and otolaryngologic literature (5, 11–17). In these, the anatomic and clinical aspects of the disease are well described, but the radiologic manifestations are not. Analysis of our cases revealed several radiologic findings that we believe are suggestive or specific for this entity.
In the four patients who underwent CT examination, no definite fluid collection was identified despite pus being drained at surgery. These patients had episodic pain and swelling for a period of weeks up to 18 months. No fluid collection was seen on the noncontrast examinations. On postcontrast studies, one failed to reveal a discrete collection (Fig 5A), the second showed a small low-attenuation area without enhancement along the mandible that could possibly represent a phlegmon or an abscess (Fig 3), and the third showed a definite abscess with rim enhancement 1 year after the patient’s initial presentation (Fig 1B). Several other studies (3, 8, 9, 13, 14,17) have failed to show a definite fluid collection despite such a finding at subsequent surgery. Thus, the absence of rim enhancement may suggest a phlegmon, but the presence of pus at the time of surgery confirms that CT findings may be falsely negative even with administration of contrast material. In our series, this may be due to the chronic nature of the infections and resultant increased attenuation of the pus that is isoattenuated relative to muscle.
In addition, partial treatment with antibiotics may contribute to the chronic nature of the condition by amelioration of systemic symptoms (ie, local infection may persist, unrecognized in a protected site, and progress to a chronic phase [5, 11, 12] without surgical drainage [15]). Such partial treatment may account for the typical absence of systemic signs and symptoms at the time of clinical presentation (5, 8). Instead, there is usually firm, relatively painless, nonfluctuant facial swelling with progressive trismus (13–15) that may mimic parotitis or tumor (8, 15). Concomitantly, the usual radiologic signs of acute infection, such as rim enhancement and infiltration of adjacent tissue planes, are rarely apparent on CT images.
Diffuse swelling of the overlying masseter or myositis was present in each case in our series and explains the symptom of trismus. The CT examination also showed sclerosis of the underlying mandibular ramus, first described by Mandel (11), in every case. Although this finding is suggestive of osteomyelitis, only one of our patients developed clinical signs of osteomyelitis following surgical drainage of the abscess. However, findings of myositis and bony sclerosis, when seen together on CT images, should suggest the presence of an infectious process.
MR imaging was obtained in two of our cases. In patient 5, the MR imaging showed a definite fluid collection beneath the right masseter muscle despite a postcontrast CT image that failed to show such an abscess (Fig 5A). Patient 4, who did not undergo CT, had MR findings demonstrating an obvious collection beneath the right masseter with abnormally low signal intensity of the underlying mandibular ramus (Fig 4C). This was our only surgically unconfirmed case. The patient was treated with multiple courses of antibiotics and continued to experience periodic facial swelling. We believe this represents a submasseteric abscess. Neither patient received intravenous gadolinium before imaging.
In the head and neck, CT plays a primary role in differentiating cellulitis from abscess and in guiding surgical drainage (3). However, the superior soft-tissue contrast offered by MR imaging provides improved visualization and differentiation of masses and inflammatory changes compared with that of CT (18). Because CT has failed to differentiate between different masseteric masses, it has been predicted that MR imaging will become the dominant technique for evaluation of this region as availability of MR systems improves (10).
Because MR imaging relies on T1 and T2 relaxation instead of attenuation of ionizing radiation to generate contrast, MR imaging is more sensitive to chronic fluid collections that are unapparent or uncertain on CT. We found MR imaging provided markedly improved definition of the abscess in one case in which both CT and MR imaging were performed (Fig 5A and B), and MR findings were clearly positive in the other case in which CT findings were not available (Fig 4B). In the case report by Fielding and colleagues (17), a medial masticator space abscess was unapparent on CT but easily visualized on MR images. We believe that MR imaging is underused for evaluation of this region and may be preferable to CT as an imaging technique.
Conclusion
Submasseteric abscess in the era of antibiotics is often chronic and misdiagnosed (1,11, 13). Radiologic criteria concerning this lesion are scarce. CT may fail to show the typical findings of an abscess, but findings of masseteric enlargement and bony sclerosis of the mandibular ramus should raise suspicion for an underlying infection. MR imaging will frequently show a fluid collection and lead to more rapid diagnosis and expeditious treatment.
A systematic review of the nonsurgical treatment of patients with appendiceal abscess or phlegmon, with emphasis on the success rate, need for drainage of abscesses, risk of undetected serious disease, and need for interval appendectomy to prevent recurrence.
SUMMARY BACKGROUND DATA:
Patients with appendiceal abscess or phlegmon are traditionally managed by nonsurgical treatment and interval appendectomy. This practice is controversial with proponents of immediate surgery and others questioning the need for interval appendectomy.
METHODS:
A Medline search identified 61 studies published between January 1964 and December 2005 reporting on the results of nonsurgical treatment of appendiceal abscess or phlegmon. The results were pooled taking the potential clustering on the study-level into account. A meta-analysis of the morbidity after immediate surgery compared with that after nonsurgical treatment was performed.
RESULTS:
Appendiceal abscess or phlegmon is found in 3.8% (95% confidence interval (CI), 2.6-4.9) of patients with appendicitis. Nonsurgical treatment fails in 7.2% (CI: 4.0-10.5). The need for drainage of an abscess is 19.7% (CI: 11.0-28.3). Immediate surgery is associated with a higher morbidity compared with nonsurgical treatment (odds ratio, 3.3; CI: 1.9-5.6; P < 0.001). After successful nonsurgical treatment, a malignant disease is detected in 1.2% (CI: 0.6-1.7) and an important benign disease in 0.7% (CI: 0.2-11.9) during follow-up. The risk of recurrence is 7.4% (CI: 3.7-11.1).
CONCLUSIONS:
The results of this review of mainly retrospective studies support the practice of nonsurgical treatment without interval appendectomy in patients with appendiceal abscess or phlegmon.
A phlegmon is an area of inflammation in the body that exudes pus and other fluids. This typically develops as a result of an infection and can create serious medical complications. The inflammation may spread to neighboring organs and lead to systemic compromise, for example, or the patient’s tissue could become so inflamed that it starts to become necrotic. Tissue necrosis, where soft tissue dies, can potentially lead to the need for amputation or other invasive treatment measures.
Patients develop phlegmonous inflammation when microorganisms start to colonize the soft tissue. This causes inflammation as the body attempts to fight them, and can lead to the production of pus and other exudate. The phlegmon may feel hot and tender to the touch, and the surface skin often has a reddish, irritated appearance. Patients may also notice swelling and a strong odor along with the irritation.
These areas of inflammation can appear in superficial or deep tissue. They may develop in association with a chronic disease or can appear independently. Bacteria are usually the cause, and the patient may develop an abscess, or a collection of pus trapped inside the body. First line treatment for a phlegmon involves medications to cut the inflammation and treat the infection. The patient may also need compresses or procedures to remove exudate if it does not drain freely.
What is phlegmon?
Phlegmon is purulent inflammation of tissue without clear boundaries, causing the destruction of the tissues. This disease often affects the blood and lymph vessels. Phlegmon often cover large areas of skin. Upper and lower limbs are often particularly affected. Doctors distinguish phlegmon breast, scrotum and neck or internal organs.
Symptoms of phlegmon
- Redness of the skin.
- Swelling.
- Pain, fever.
- Impaired function of the affected body part.
- Swollen lymph nodes.
Causes of phlegmon
Phlegmon most often caused by staphylococci, streptococci rarely, coliform bacteria and other microbes. Often the bacteria penetrate from the outside through the affected skin or mucous membranes. Skin damage can be so mild that people do not pay attention to them, such as acne, wound from an insect bite or needle stick, an abscess. Less common so-called progressive inflammation, in which the bacteria penetrate the blood flow in the subcutaneous layers, causing phlegmon. However, pathogens can spread only if the weakened defenses. Medication can weaken the immune system too.
Treatment of phlegmon
The first phase of timely treatment is usually an immobilizing the affected part of the body and performing a cold compress. With the defeat of the forearm doctors impose special fixing the tire on the upper limb. Cold compresses applied to 30% solution of isopropyl alcohol. Such treatment abscess begins to diminish after a few hours, and eventually completely go away. When tissue festered and chronic inflammation, treatment is antibiotics, skin smear reduces swelling ointments. If the treatment fails, the patient is being operated. After the operation, the wound is left drains, antiseptic lotions is being imposed on wound.
At the beginning of the disease should apply a cold compress to the affected area. They should be changed frequently, avoiding them be heating! If there was pus, the affected area of the body will have been washed with warm water several times a day. Self-treatment phlegmon is allowed only in the early stages of the disease. With the progression of phlegmon you should see a doctor.
Due to possible complications (infection can spread to the internal organs hit) phlegmon physician should always be treated.
In progressive phlegmon and a weakened immune system, the doctor refers the patient to the hospital.
Course of the disease
Phlegmon is often formed in a few hours. There are symptoms of inflammation – the skin turns red, becomes hot and painful. The function of the affected part of the body is broken. Phlegmon is characterized by the lack of clear boundaries redness Deep subcutaneous tissues become swollen. Initially tissue resemble dough and later connective tissue gradually eroded, compacted. There is the so-called woody phlegmon. Phlegmon is always very painful. If the infection is caused by streptococcus, often the patient has a fever, worsening overall health. If the infection is caused by staphylococcus, the symptoms are expressed not so bright. As the disease progresses, pus accumulates in the deeper layers of tissue. Lymph nodes near the phlegmon increases. Phlegmon is different from the abscess, it is characterized by swelling of the tissues, but little pus. In the absence of timely treatment, it quickly spread to nearby tissue and deeply, covering the blood and lymph vessels and nerves. Later, there may be complications: venous thrombosis, sepsis, when the penetration of pus in the surrounding tissue may inflammation of the joints and muscles.
Is phlegmon a dangerous disease?
If the phlegmon is repeated, deep subcutaneous layers so devastated, unable to complete healing, tissue remain tight and swollen. Getting into the blood and lymph, causative agents of purulent infection spread throughout the body, inflammation of the kidneys and lungs starts, the heart is affected. There is a serious threat to human life.
At first, a cold compress imposes in phlegmon. If there was pus, it is necessary to refuse from a cold compress and seek emergency medical attention.
|
|
Phlegmon an acute, diffuse, purulent inflammation of adipose tissue. Unlike an abscess, a phlegmon lacks precise boundaries. Phlegmons are classified by site. They may occur in many parts of the body, including the foot and the hand, and may be subcutaneous, subfascial, intermuscular, retroperitoneal, paranephric (paranephritis), pararectal (paraproctitis), or mediastinal. The causative agents are primarily staphilococci, other pyogenic microorganisms, and, less commonly, Escherichia coli and anaerobes. Phlegmons may also be classified according to the characteristics of the causative agents as suppurative, putrefactive, and anaerobic. The causative agents penetrate the tissue through breaks in the skin or from nearby foci of infection, such as furuncles, dental caries, or suppurating lymph nodes. Sometimes they are brought to the site hematogenously—that is, through the bloodstream— from foci at some distance. The symptoms of phlegmon include pain, edema, elevated body temperature, and chills; subcutaneous phlegmon has the added symptom of cutaneous hyperemia. The inflammatory process may spread to neighboring organs, and sepsis may develop. Phlegmon is treated by exposing and draining the suppurative focus and by antibiotic therapy. It is prevented by keeping the skin clean, attending to minor injuries, and promptly treating pyodermas and other local foci of infection. |
Odontogenic Infections-Oral Surgery
In order to understand how odontogenic infections are treated, the dentist must be familiar with the terminology concerning infection and the pathophysiology of inflammation, which are described below.
Inoculation
is characterized by the entry of pathogenic microbes into the body without disease occurring.An infection involves the proliferation of microbes resulting in triggering of the defense mechanism, a process manifesting as inflammation.
Inflammation
is the localized reaction of vascularand connective tissue of the body to an irritant, resulting in the development of an exudate rich in proteins and cells. This reaction is protective and aims at limiting or eliminating the irritant with various procedures while the mechanism of tissue repair is triggered. Depending on the duration and severity, inflammation is distinguished as acute, subacute or chronic.
Acute Inflammation
This is characterized by rapid progression and is associated with typical signs and symptoms. If it does not regress completely, it may become subacute or chronic.
Subacute Inflammation
This is considered a transition phase between acute and chronic inflammation.
Chronic Inflammation
This procedure presents a prolonged time frame with slight clinical symptoms and is characterized mainly by the development of connective tissue. Inflammation may be caused by, among other things, microbes, physical and chemical factors, heat, and irradiation. Regardless of the type of irritant and the location of the defect, the manifestation of inflammation is typical and is characterized by the following clinical signs and symptoms: rubor (redness), calor (heat), tumor (swelling or edema), dolor (pain), and functio laesa (loss of function).
The natural progression of inflammation is distinguished into various phases. Initially vascular reactions
with exudate are observed (serous phase), and then the cellular factors are triggered (exudative or cellular phase). The inflammation finally resolves and the destroyed tissues are repaired. On the other hand, chronic inflammation is characterized by factors of reparation and healing. Therefore, while acute inflammation is exudative, chronic inflammation is productive (exudative and reparative). Understanding the differences between these types of inflammation is important for therapeutic treatment. Serous Phase. This is a procedure that lasts approximately 36 h, and is characterized by local inflammatory edema, hyperemia or redness with elevated temperature, and pain. Serous exudate is observed at this stage, which contains proteins and rarely polymorphonuclear leukocytes.
Cellular Phase.
This is the progression of the serous phase. It is characterized by massive accumulation of polymorphonuclear leukocytes, especially neutrophil granulocytes, leading to pus formation. If pus forms in a newly developed cavity, it is called an abscess. If it develops in a cavity that already exists, e.g., the maxillary sinus, it is called an empyema.
Reparative Phase
During inflammation, the reparative phenomena begin almost immediately after inoculation. With the reparative mechanism of inflammation, the products of the acute inflammatory reaction are removed and reparation of the destroyed tissues follows. Repair is achieved with development of granulation tissue, which is converted to fibrous connective tissue, whose development ensures the return of the region to normal.
Infections of the Orofacial Region
The majority (i.e., 90–95%) of infections that manifest in the orofacial region are odontogenic. Of these, approximately 70% present as periapical inflammation, principally the acute dentoalveolar abscess, with the periodontal abscess following, etc.
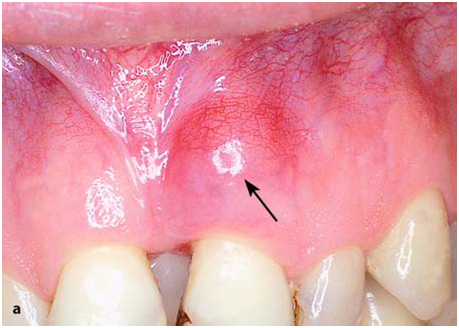
Periodontal abscess originating from a maxillary central incisor.

Radiograph of same case showing bone resorption, which led to the formation of a periodontal pocket
Etiology
The cardinal causes of orofacial infections are non-vital teeth, pericoronitis (due to a semi-impacted mandibular tooth), tooth extractions, periapical granulomas that cannot be treated, and infected cysts. Rarer causes include postoperative trauma, defects due to fracture, salivary gland or lymph node lesions, and infection as a result of local anesthesia.
Periodontal Abscess
This is an acute or chronic purulent inflammation, which develops in an existing periodontal pocket. Clinically, it is characterized by edema located at the middle of the tooth, pain, and redness of the gingiva. These symptoms are not as severe as those observed in the acute dentoalveolar abscess, which is described below.
Treatment of the periodontal abscess is usually simple and entails incision, through the gingival sulcus with a probe or scalpel, of the periodontal pocket that has become obstructed. Incision may also be performed at the gingivae; more specifically, at the most bulging point of the swelling or where fluctuation is greatest.
Acute Dentoalveolar Abscess
This is an acute purulent inflammation of the periapical tissues, presenting at nonvital teeth, especially when microbes exit the infected root canals into periapical tissues. Clinically, it is characterized by symptoms that are classified as local and systemic.
Local Symptoms
Pain
The severity of the pain depends on the stage of development of the inflammation. In the initial phase the pain is dull and continuous and worsens during percussion of the responsible tooth or when it comes into contact with antagonist teeth. If the pain is very severe and pulsates, it means that the accumulation of pus is still within the bone or underneath the periosteum. Relief of pain begins as soon as the pus perforates the periosteum and exits into the soft tissues.
Edema
Edema appears intraorally or extraorally and it usually has a buccal localization and more rarely palatal or lingual. In the initial phase soft swelling of the soft tissues of the affected side is observed, due to the reflex neuroregulating reaction of the tissues, especially of the periosteum. This swelling presents before suppuration, particularly in areas with loose tissue, such as the sublingual region, lips, or eyelids. Usually the edema is soft with redness of the skin. During the final stages, the swelling fluctuates, especially at the mucosa of the oral cavity. This stage is considered the most suitable for incision and drainage of the abscess.
Other Symptoms
There is a sense of elongation of the responsible tooth and slight mobility; the tooth feels extremely sensitive to touch, while difficulty in swallowing is also observed.
Systemic Symptoms
The systemic symptoms usually observed are: fever, which may rise to 39–40 °C, chills,malaise with pain inmuscles and joints, anorexia, insomnia, nausea, and vomiting. The laboratory tests show leukocytosis or rarely leukopenia, an increased erythrocyte sedimentation rate, and a raised C-reactive protein (CRP) level.
Complications
If the inflammation is not treated promptly, the following complications may occur: trismus, lymphadenitis at the respective lymph nodes, osteomyelitis, bacteremia, and septicemia.
Diagnosis
Diagnosis is usually based upon clinical examination and the patient’s history. What mainly matters, especially in the initial stages, is the localization of the responsible tooth. In the initial phase of inflammation, there is soft swelling of the soft tissues. The tooth is also sensitive during palpation of the apical area and during percussion with an instrument, while the tooth is hypermobile and there is a sense of elongation. In more advanced stages, the pain is exceptionally severe, even after the slightest contact with the tooth surface. Tooth reaction during a test with an electric vitalometer is negative; however, sometimes it appears positive,which is due to conductivity of the fluid inside the root canal.
Radiographically, in the acute phase, no signs are observed at the bone (whichmay beobserved 8–10 days later), unless there is recurrence of a chronic abscess,where upon osteolysis is observed. Radiographic verification of a deeply carious tooth or restoration very close to the pulp, as well as thickening of the periodontal ligament, are data that indicate the causative tooth.
Differential diagnosis of the acute dentoalveolar abscess includes the periodontal abscess, and the dentist must be certain of his or her diagnosis, because treatment between the two differs.
Spread of Pus Inside
Tissues From the site of the initial lesion, inflammation may spread in three ways:
1. By continuity through tissue spaces and planes.
2. By way of the lymphatic system.
3. By way of blood circulation.
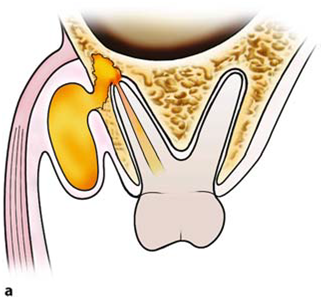
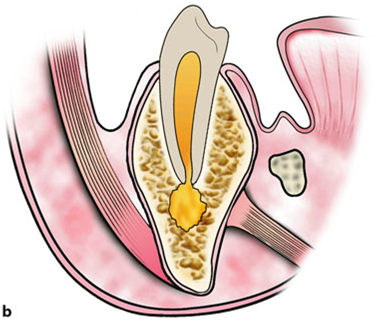
Diagrammatic illustrations showing spread of infection (propagation of pus) of an acute dentoalveolar abscess,depending on the position of the apex of the responsible tooth. a Buccal root: buccal direction.b Palatal root: palatal direction
The most common route of spread of inflammation is by continuity through tissue spaces and planes and usually occurs as described below. First of all, pus is formed in the cancellous bone, and spreads in various directions by way of the tissues presenting the least resistance.

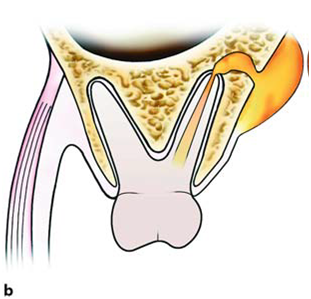
a Spread of pus towards the maxillary sinus, due to the closeness of the apices to the floor of the antrum.b Diagrammatic illustration showing the localization of infection above or below the mylohyoid muscle, depending on the position of the apices of the responsible tooth
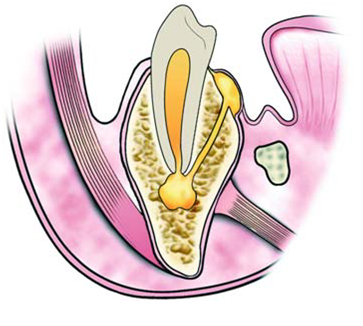
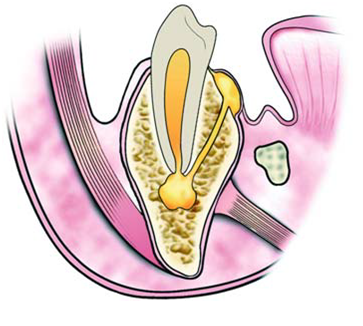
Whether the pus spreads buccally, palatally or lingually depends mainly on the position of the tooth in the dental arch, the thickness of the bone, and the distance it must travel.Purulent inflammation that is associated with apices near the buccal or labial alveolar bone usually spreads buccally, while that associated with apices near the palatal or lingual alveolar bone spreads palatally or lingually respectively. For example,the palatal roots of the posterior teeth and the maxillary lateral incisor are considered responsible for the palatal spread of pus, while the mandibular third molar and sometimes the mandibular second molar are considered responsible for the lingual spread of infection. Inflammation may even spread into the maxillary sinus when the apices of posterior teeth are found inside or close to the floor of the antrum. The length of the root and the relationship between the apex and the proximal and distal attachments of various muscles also play a significant role in the spread of pus. Depending on these relationships, in the mandible pus originates from the apices found above themylohyoid muscle, and usually spreads intraorally, mainly towards the floor of the mouth (sublingual space). When the apices are found beneath the mylohyoid muscle (second and third molar), the pus spreads towards the submandibular space, resulting in extraoral localization. Infection originating from incisors and canines of the mandible spreads buccally or lingually, due to the thin alveolar bone of the area. It is usually localized buccally if the apices are found above the attachment of the mentalis muscle. Sometimes, though, the pus spreads extraorally, when the apices are found beneath the attachment. In the maxilla, the attachment of the buccinators muscle is significant.When the apices of the maxillary premolars and molars are found beneath the attachment of the buccinator muscle, the pus spreads intraorally; however, if the apices are found above its attachment, infection spreads upwards and extraorally. Exactly the same phenomenon is observed in the mandible as in the maxilla if the apices are found above or below the attachment of the buccinator muscle.


Spread of pus depending on the length of root and attachment of buccinators muscle. a Apex above attachment: accumulation of pus in the buccal space. b Apex beneath the buccinator muscle: intraoral pathway towards the mucobuccal fold
In the cellular stage, depending on the pathway and inoculation site of the pus, the acute dentoalveolar abscessmay have various clinical presentations, such as:(1) intraalveolar, (2) subperiosteal, (3) submucosal, (4) subcutaneous, and (5) fascial ormigratory – cervicofacial.
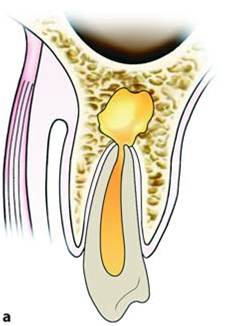
Intraalveolar abscess of maxilla (a) and mandible (b). Diagrammatic illustrations show accumulation of pus at a portion of the alveolar bone in relation to the periapical region
The initial stage of the cellular phase is characterized by accumulation of pus in the alveolar bone and is termed anintraalveolar abscess . The pus spreads outwards from this site and, after perforating the bone, spreads to the subperiosteal space, from which the subperiosteal abscess originates, where a limited amount of pus accumulates between the bone and periosteum. After perforation of theperiosteum, the pus continues to spread through the soft tissues in various directions. It usually spreads intraorally, spreading underneath the mucosa forming the submucosal abscess.

Subperiosteal abscess with lingual localization. a Diagrammatic illustration; b clinical photograph
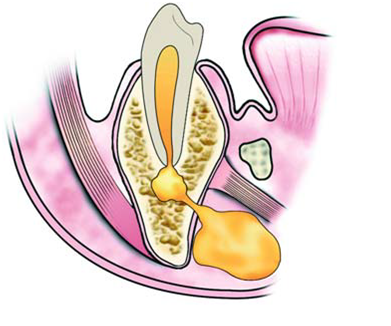
Sometimes, though,it spreads through the loose connective tissue and, after its pathway underneath the skin, forms a subcutaneous abscess, while other times it spreads towards the fascial spaces, forming serious abscesses calledfascial space abscesses.


Subcutaneous abscess originating from a mandibular tooth. a Diagrammatic illustration. b Clinical photograph.The swelling mainly involves the region of the angle of the mandible
The fascial spaces are bounded by the fascia, which may stretch or be perforated by the purulent exudate, facilitating the spread of infection. These spaces are potential areas and do not exist in healthy individuals, developing only in cases of spread of infection that have not been treated promptly. Some of these spaces contain loose connective tissue, fatty tissue, and salivary glands,while others contain neurovascular structures. Acute diffuse infection,which spreads into the loose connective tissue to agreat extent underneath the skin with or without suppuration,is termed “cellulitis” (phlegmon), and is described iext posts.
+Clinical+photograph.png)
Fascial abscess (submandibular). a Diagrammatic illustration. b Clinical photograph.


{kind=link}