Anatomy of the Eye
|
|
Before discussing conditions affecting the eye, we need to review some basic eye anatomy. Anatomy can be painful for some (personally, I hated anatomy in medical school) so I’m going to keep this simple. Let us start from the outside and work our way toward the back of the eye.
Eyelids
The eyelids protect and help lubricate the eyes. The eyelid skin itself is very thin, containing no subcutaneous fat, and is supported by a tarsal plate. This tarsal plate is a fibrous layer that gives the lids shape, strength, and a place for muscles to attach. ![]()
Underneath and within the tarsal plate lie meibomian glands. These glands secrete oil into the tear film that keeps the tears from evaporating too quickly. Meibomian glands may become inflamed and swell into a granulomatous chalazion that needs to be excised. Don’t confuse a chalazion with a stye. A stye is a pimple-like infection of a sebaceous gland or eyelash follicle, similar to a pimple, and is superficial to the tarsal plate. Styes are painful, while chalazions are not.
Eyelid Movement
![]()
Two muscles are responsible for eyelid movement. The orbicularis oculi closes the eyelids and is innervated by cranial nerve 7. Patients with a facial nerve paralyses, such as after Bell’s Palsy, can’t close their eye and the eye may need to be patched (or sutured closed) to protect the cornea. The levator palpebrae opens the eye and is innervated by CN3. Oculomotor nerve palsy is the major cause of ptosis (drooping of the eye). In fact, a common surgical treatment for ptosis involves shortening the levator tendon to open up the eye.

CN 3 opens the eye like a pillar
CN 7 closes like a fish-hook
Conjunctiva
![]() The conjunctiva is a mucus membrane that covers the front of the eyeball. When you examine the “white part” of a patient’s eyes, you’re actually looking through the semi-transparent conjunctiva to the white sclera of the eyeball underneath. The conjunctiva starts at the edge of the cornea (this location is called the limbus). It then flows back behind the eye, loops forward, and forms the inside surface of the eyelids. The continuity of this conjunctiva is important, as it keeps objects like eyelashes and your contact lens from sliding back behind your eyeball. The conjunctiva is also lax enough to allow your eyes to freely move. When people get conjunctivitis, or “pink eye,” this is the tissue layer affected.
The conjunctiva is a mucus membrane that covers the front of the eyeball. When you examine the “white part” of a patient’s eyes, you’re actually looking through the semi-transparent conjunctiva to the white sclera of the eyeball underneath. The conjunctiva starts at the edge of the cornea (this location is called the limbus). It then flows back behind the eye, loops forward, and forms the inside surface of the eyelids. The continuity of this conjunctiva is important, as it keeps objects like eyelashes and your contact lens from sliding back behind your eyeball. The conjunctiva is also lax enough to allow your eyes to freely move. When people get conjunctivitis, or “pink eye,” this is the tissue layer affected.
There is a thickened fold of conjunctiva called the semilunar fold that is located at the medial canthus – it is a homolog of the nictitating membrane seen on sharks.
Tear Production and Drainage
![]() The majority of tears are produced by accessory tear glands located within the eyelid and conjunctiva. The lacrimal gland itself is really only responsible for reflexive tearing. Tears flow down the front of the eye and drain out small pores, called lacrimal punctum, which arise on the medial lids. These puncta are small, but can be seen with the naked eye.
The majority of tears are produced by accessory tear glands located within the eyelid and conjunctiva. The lacrimal gland itself is really only responsible for reflexive tearing. Tears flow down the front of the eye and drain out small pores, called lacrimal punctum, which arise on the medial lids. These puncta are small, but can be seen with the naked eye.
After entering the puncta, tears flow down the lacrimal tubing and eventually drain into the nose at the inferior turbinate. This explains why you get a runny nose when you cry. In 2-5% of newborns, the drainage valve within the nose isn’t patent at birth, leading to excessive tearing. Fortunately, this often resolves on it’s own, but sometimes we need to force open the pathway with a metal probe.
Lid Lacerations
![]() Most lacerations through the eyelid can be easily reaproximated and repaired. However, if a laceration occurs in the nasal quadrant of the lid you have to worry about compromising the canalicular tear-drainage pathway. Canalicular lacerations require cannulation with a silicone tube to maintain patency until the tissue has healed.
Most lacerations through the eyelid can be easily reaproximated and repaired. However, if a laceration occurs in the nasal quadrant of the lid you have to worry about compromising the canalicular tear-drainage pathway. Canalicular lacerations require cannulation with a silicone tube to maintain patency until the tissue has healed.
Warning: Drug absorption through the nasal mucosa can be profound as this is a direct route to the circulatory system and entirely skips liver metabolism. Eyedrops meant for local effect, such as beta-blockers, can have impressive systemic side effects when absorbed through the nose. Patients can decrease nasal drainage by squeezing the medial canthus after putting in eyedrops. They should also close their eyes for a few minutes afterwards because blinking acts as a tear pumping mechanism.
The Eyeball:
![]() The eyeball is an amazing structure. It is only one inch in diameter, roughly the size of a ping-pong ball, and is a direct extension of the brain. The optic nerve is the only nerve in the body that we can actually see (using our ophthalmoscope) in vivo.
The eyeball is an amazing structure. It is only one inch in diameter, roughly the size of a ping-pong ball, and is a direct extension of the brain. The optic nerve is the only nerve in the body that we can actually see (using our ophthalmoscope) in vivo.
The outer wall of the eye is called the sclera. The sclera is white, fibrous, composed of collagen, and is actually continuous with the clear cornea anteriorly. In fact, you can think of the cornea as an extension of the sclera as they look similar under the microscope. The cornea is clear, however, because it is relatively dehydrated. At the back of the eye, the sclera forms the optic sheath encircling the optic nerve.
![]() The eyeball is divided into three chambers, not two as you might expect. The anterior chamber lies between the cornea and the iris, the posterior chamber between the iris and the lens, and the vitreous chamber extends from the lens back to the retina.
The eyeball is divided into three chambers, not two as you might expect. The anterior chamber lies between the cornea and the iris, the posterior chamber between the iris and the lens, and the vitreous chamber extends from the lens back to the retina.
The eye is also filled with two different fluids. Vitreous humor fills the back vitreous chamber. It is a gel-suspension with a consistency similar to Jell-O. With age and certain degenerative conditions, areas of the vitreous can liquefy. When this occurs, the vitreous can fall in upon itself – usually a harmless event called a PVD (posterior vitreous detachment). However, this normally benign vitreous detachment can sometimes tug on the retina and create small retinal tears.
Aqueous humor fills the anterior and posterior chambers. This is a watery solution with a high nutrient component that supports the avascular cornea and lens. Aqueous is continuously produced in the posterior chamber, flowing forward through the pupil into the anterior chamber, where it drains back into the venous circulation via the Canal of Schlemm. We’ll discuss the aqueous pathway in detail in the glaucoma chapter.
The Cornea:
The cornea is the clear front surface of the eye. The cornea-air interface actually provides the majority of the eye’s refractive power. The cornea is avascular and gets its nutrition from tears on the outside, aqueous fluid on the inside, and from blood vessels located at the periphery.
On cross section, the cornea contains five distinct layers. The outside surface layer is composed of epithelial cells that are easily abraded. Though epithelial injuries are painful, this layer heals quickly and typically does not scar. Under this lies Bowman’s layer and then the stroma. The corneal stroma makes up 90% of the corneal thickness, and if the stroma is damaged this can lead to scar formation. The next layer is Descemet’s membrane, which is really the basal lamina of the endothelium, the final inner layer.
The inner endothelium is only one cell layer thick and works as a pump to keep the cornea dehydrated. If the endothelium becomes damaged (during surgery or by degenerative diseases) aqueous fluid can flow unhindered into the stroma and cloud up the cornea with edema. Endothelial cell count is very important as these cells don’t regenerate when destroyed – the surviving endothelial cells just get bigger and spread out. If the cell count gets too low, the endothelial pump can’t keep up and the cornea swells with water, possibly necessitating a corneal transplant to regain vision.
Decemet’s membrane is “deep,” while Bowman’s layer is high up in the “belfry.” A belfry is a room, usually high up in a tower, where bells are hung.
![]() The Anterior Chamber Angle:
The Anterior Chamber Angle:
The angle formed by the inner cornea and the root of the iris is particularly important in ophthalmology. Here you find the trabecular meshwork with its underlying Schlemms Canal. This is where aqueous is drained, and blockage of this pathway/angle will become important as we discuss glaucoma.
![]() The Uvea:
The Uvea:
The iris, ciliary body, and the choroid plexus are all continuous with each other and are collectively called the uvea. This is an important term, as many people can present with painful “uveitis” – spontaneously or in associated with rheumatologic diseases.
The iris is the colored part of the eye and its primary function is to control the amount of light hitting the retina. Sympathetic stimulation of the pupil leads to pupil dilation and parasympathetic stimulation leads to constriction. In other words, if you see a bear in the woods, your sympathetics kick in, and your eyes dilate so you can see as much as possible as you run away. I’ll be using this mnemonic/metaphore many times throughout this book to help you remember this concept.
The inner iris flows back and becomes the ciliary body. The ciliary body has two functions: it secretes aqueous fluid and it controls the shape of the lens. The ciliary body contains sphincter muscles that change the lens shape by relaxing the zonular fibers that tether to the lens capsule.
The choroid is a bed of blood vessels that lie right under the retina. The choroid supplies nutrition to the outer one-third of the retina which includes the rod and cone photoreceptors. Retinal detachments can separate the retina from the nutritious choroid, which is disastrous for the photoreceptors as they quickly die without this nourishment.
Lens:
The lens sits behind the iris. The lens is unique in that it doesn’t have any innervation or vascularization. It gets its nourishment entirely from nutrients floating in the aqueous fluid. The lens also has the highest protein concentration of any tissue in the body (65% water, 35% protein).![]()
The lens has three layers in a configuration similar to a peanut M&M. The outer layer is called the capsule. The capsule is thin with a consistency of saran wrap and holds the rest of the lens in place. The middle layer is called the cortex, while the central layer is the hard nucleus. Cataracts are described by where they occur such as nuclear cataracts, cortical cataracts, and subcapsular cataracts. With cataract surgery the outer capsule is left behind and the artificial lens is placed inside this suporting bag.
The capsule is held in place by suspensory ligaments called zonules that insert around the periphery and connect to the muscular ciliary body. Contraction of the ciliary muscle causes the zonule ligaments to relax (think about that for a minute), allowing the lens to become rounder and increase its refracting power for close-up reading.
In children the lens is soft but with age the lens hardens and becomes less pliable. After age 40 the lens starts having difficulty “rounding out” and people have problems focusing oear objects. This process is called presbyopia. Almost everyone over 50 needs reading glasses because of this hardening of the lens.
The Retina:
![]() The retina is the sensory portion of the eye and contains layers of photoreceptors, nerves, and supporting cells. Histologically, many cell layers can be seen, but they are not worth memorizing at this point. The important ones include the photoreceptor layer, which is located further out (towards the periphery), and the ganglioerve layer which lies most inward (toward the vitreous). For light to reach the photoreceptor it has to pass through many layers. After light reaches the photoreceptors the visual signal propagates back up to the ganglioerves. These ganglioerves, in turn, course along the surface of the retina toward the optic disk and form the optic nerve running to the brain.
The retina is the sensory portion of the eye and contains layers of photoreceptors, nerves, and supporting cells. Histologically, many cell layers can be seen, but they are not worth memorizing at this point. The important ones include the photoreceptor layer, which is located further out (towards the periphery), and the ganglioerve layer which lies most inward (toward the vitreous). For light to reach the photoreceptor it has to pass through many layers. After light reaches the photoreceptors the visual signal propagates back up to the ganglioerves. These ganglioerves, in turn, course along the surface of the retina toward the optic disk and form the optic nerve running to the brain.
![]() The macula is the pigmented area of the retina that is responsible for central vision. Within the central macula lies the fovea, which is a small pit that is involved with extreme central vision. The fovea is very thin and derives its nutrition entirely from the underlying choroid, making it susceptible to injury during retinal detachments.
The macula is the pigmented area of the retina that is responsible for central vision. Within the central macula lies the fovea, which is a small pit that is involved with extreme central vision. The fovea is very thin and derives its nutrition entirely from the underlying choroid, making it susceptible to injury during retinal detachments.
The optic disk is the entry and exit point of the eye. The central retinal artery and vein pass through here, along with the the ganglioerves that form the optic nerve. A physiologic divot or “cup” can be found here that will become important when we talk about glaucoma.
The Orbital Walls:
Seven different bones form the orbital walls: don’t be intimidated by this complexity, however, as these bones are not that confusing when you break them down. For example, the roof of the orbit is a continuation of the frontal bone, the zygomatic bone forms the strong lateral wall, while the maxillary bone creates the orbital floor. This makes sense, and you could probably guess these bones from the surrounding anatomy.
The medial wall is a little more complex, however, but is mainly formed by the lacrimal bone (the lacrimal sac drains tears through this bone into the nose) and the ethmoid bone. The thinnest area in the orbit is a part of the ethmoid bone called the lamina papyracea. Sinus infections can erode through this “paper-thin wall” into the orbital cavity and create a dangerous orbital cellulites.
Despite the fragility of the medial wall, it is well buttressed by surrounding bones, such that it’s the orbital floor that breaks most often during blunt trauma. The maxillary bone fractures downward and the orbital contents can herniate down into the underlying maxillary sinus. This is called a “blowout fracture” and can present with enopthalmia (a sunken-in eyeball) and problems with eye-movements from entrapment of the inferior rectus muscle. We’ll discuss blow-out fractures in more detail in the trauma chapter.
The back of the orbit is formed by the greater wing of the sphenoid bone, with the “lesser wing” surrounding the optic canal. There’s also a little palatine bone back there in the middle, but don’t worry about that one!
The Apex: Entrance into the Orbit
The orbital apex is the entry point for all the nerves and vessels supplying the orbit. The superior orbital fissure lies between the wings of the sphenoid bones, through which many vessels and nerves pass into the orbit.
The “Annulus of Zinn,” a muscular band that serves as the insertion point for most of the ocular muscles, rests on top of the superior orbital fissure. The four rectus muscles attach to the annulus and the optic nerve passes right through the middle.
Eye Muscles:
![]() Four rectus muscles control each eye. These muscles insert at the sclera, behind the limbus, and each pull the eye in the direction of their attachment.
Four rectus muscles control each eye. These muscles insert at the sclera, behind the limbus, and each pull the eye in the direction of their attachment.
The superior, medial, and inferior rectus muscles are all controlled by the oculomotor nerve (III). The lateral rectus, however, is controlled by the abducens (VI) nerve, which makes sense as the lateral rectus “abducts” the eye.
The remaining two eye muscles are the superior and inferior oblique muscles. The superior oblique also originates in the posterior orbit, but courses nasally until it reaches the trochlea (or “pulley”) before inserting onto the eye. The inferior oblique originates from the orbital floor and inserts behind the globe near the macula. Because of these posterior insertions, the oblique muscles are primarily responsible for intorsion and extorsion (rotation of the eye sideways), though they also contribute some vertical gaze action.
Confused, yet? Don’t kill yourself learning the action of the oblique muscles or nerve innervation as we’ll discuss these topics in greater detail in the neurology chapter.
Summary:
There is much more anatomy we could cover, but let’s hold off for now and discuss more detailed anatomy in future chapters as they become relevant.
|
Pimp Questions |
1. Why don’t objects like contact lens and eyelashes get stuck behind the eye?
Because the conjunctiva covering the front of the eye loops forward and covers the inside of the eyelids as well.
2. How many chambers are there in the eyeball?
Three, actually. The anterior chamber sits in front of the iris, the posterior chamber between the iris and the lens, and the vitreous chamber lies behind the lens filling most of the eye.
3. Name each of the numbered bones.
Which bone is thinnest?
Which is most likely to fracture after blunt injury?
Which is most likely to erode from sinus infections?
The bones are: (1)Sphenoid (2)Zygomatic (3)Maxilla (4)Lacrimal (5)Ethmoid (6)Frontal. The ethmoid is the thinnest bone and most likely to perforate from an eroding sinus infection (this happens mostly in kids). The maxillary floor is most likely to fracture from blunt injury.
3. What is the uvea? What eye structures compose it?
The uvea comprises the iris, ciliary body, and the choroid. They are all connected to each other and are histologically similar. Patients can present with a painful “uveitis,” an inflammation of the uvea, often secondary to rheumatological/inflammatory conditions like sarcoidosis.
4. Where does the retina get its nutrition supply?
The inner 2/3rds of the retina (inner implies toward the center of the eyeball) gets its nutrition from the retinal vessels. The outer 1/3 (which includes the photoreceptors) is nourished by the underlying choroid plexus. A retinal detachment, which separates the retina from the choroid, is particularly dangerous for the photoreceptors. This is especially true for detachments involving the macula as the thin macula gets its blood supply primarily from the underlying choroid.
5. When the ciliary body contracts, how does the lens change shape (does it get rounder or flatter)?
The ciliary body is a round, spincter-like muscle, so when it contracts the zonules actually relax, allowing the lens to relax and become rounder. With age, the lens hardens and has a hard time relaxing, no matter how hard the ciliary muscle contracts. This aging process is called presbyopia.
6. Which extraocular muscle doesn’t originate at the orbital apex?
Unlike the other muscles, the inferior oblique originates from the orbital floor before inserting on the back of the globe near the macula.
7. Which full-thickness eyelid laceration is more dangerous – medial or lateral lacerations? Why?
You worry about the canalicular tear-drainage system involvement with medial lacerations. You want to repair this system as soon as possible, to avoid chronic epiphora.
8. How many layers are there in the cornea? Can you name them?There are five: the superficial Epithelium, Bowman’s layer, Stroma, Decemet’s membrane, and the inner Endothelium.
9. How does the water content of the cornea differ from the rest of the eye?
The cornea is relatively dehydrated, which helps with clarity. If water gets into the cornea, via a disrupted endothelium or a high pressure gradient from acute glaucoma, the cornea turns hazy and white.
As we get older, our natural lenses harden and do not change shape very well making it hard to accommodate and see near objects. This phenomenon is called presbyopia and is a normal finding in people over 40 years of age. A prosthetic lens is not able to change shape at all, so all patients (including small children) with implanted plastic lenses require reading glasses to read.
DIFFERENT VISUAL FUNCTIONS
Vision is composed of many simultaneous functions. If vision is normal, seeing is so effortless that we do not notice the different visual functions.
The different components of the visual image are:
- forms
- colours
- movement.
Thus we have form perception, colour perception and motion perception.
We see both during the day light and during very dim light. In day light, photopic vision, we perceive colours because of function of the cone cells; in very dim light, scotopic vision, we see only shades of gray, since rod cells respond only to luminance differences. In twilight, when both rod and cone cells function, we have mesopic vision.
Vision is measured with many different tests. In the following chapters we will discuss such tests and measurements that are often done in the doctors’ offices and in the hospital clinics: visual acuity, visual field, contrast sensitivity, colour vision, visual adaptation to different luminance levels, binocular vision and stereoscopic vision.
Visual acuity
Visual acuity is measured with visual acuity charts at distance and at near. The test measures what is the smallest letter, number or picture size that the patient still sees correctly. Visual acuity is good only in the very middle of the retina (Fig.20).
|
Fig.20. In the middle of the retina there is a small pit, the fovea, with which we see sharply. Only a few millimeters from the fovea (arrows) the visual acuity is 20/200 (6/60 or 0.1) even in a normal person. |
|
Visual field
When a person with normal vision looks straight forward without moving the eyes, he sees also on both sides. The area visible at once, without moving the eyes, is called visual field. Nerve fibres from both eyes are divided so that fibers from the right half of both eyes reach the right half of the brain and fibers from the left half of both eyes the left half of the brain (Fig.21).
|
|
Fig.21. Visual pathways from the eyes to the visual cortex. Note that there are also connections to the central parts of the brain. Note also that in the optic radiation, the pathway from the LGN (lateral geniculate nucleus) to the primary visual cortex there are marked arrows in the direction from the primary visual cortex to the LGN. Actually, there are some ten times more fibres bringing information from the primary visual cortex to the LGN than in the opposite direction. From the primary visual cortex information flows “backwards” also to the superior colliculus (SC). |
Visual information coming from both eyes is fused in the visual cortex in the back of the brain. The central part of the visual field is seen by both eyes (Fig.22). On both sides of this central, binocular field there are half moon formed parts of visual field that are seen by only one eye.
|
|
|
Fig.22. Visual field. |
We use our peripheral or side vision when moving around. The most central part of the visual field is used in sustained near work, e.g., reading. When the visual field is measured with the clinical instruments these instruments measure what the weakest light is that the eye still can see in different parts of the visual field. A measurement like this gives valuable information on diseases of the visual pathways related to glaucoma or neurologic diseases. It does not give information on how the person sees forms or perceives movement in the different parts of the visual field.
The visual field can change in many ways. Therefore it is often difficult to understand how a visually impaired person sees. If the side parts of the visual field function poorly the person may need to use a white cane in order to move around safely, but he may be able to read without glasses. On the other hand, if the side parts function well and the central field functions poorly, the person may walk like a normally sighted person, but may be able to read only the headings of a newspaper.
Contrast sensitivity
Contrast sensitivity is depicted by a curve (Figure 23A). Under the curve there are the objects that we can see, above and to the right of the slope of the curve is the visual information that we cannot see. Contrast sensitivity can be measured using striped patterns, gratings, or symbols at different contrast levels.
A
B
Fig.23. A. Contrast sensitivity curve. B. Visual information at different contrasts in different sizes. Note that large numbers are visible at a fainter contrast than small numbers.
When we measure hearing, an audiogram depicts whichs are the weakest tones at different frequencies that we still can hear. The measurements are made at low, intermediate and high frequencies. When we measure contrast sensitivity we measure what is the faintest grating or symbol still visible when the symbols are large, medium size or small (Fig.23B).
If a visually impaired person has poor contrast sensitivity (s)he cannot see small contrast differences between adjacent surfaces. Everything becomes flat. It is difficult to perceive facial features and expressions. Text in the newspapers seems to have less contrast than before and it is difficult to recognise the edge of the pavement and the stairs.
Contrast sensitivity decreases in several common diseases, diabetes, glaucoma, cataract and diseases of the optic nerve.
Visual adaptation to different luminance levels
A normally sighted person can read by one candle’s light and he can read in bright sun light. The difference in the amount of light present in these two situations is million times. The normal person can adapt his/her vision to function at the different luminance levels.
The rod cells of the retina see best in twilight. If they do not function, the person is night blind. Night blindness is the first symptom that develops in many retinal diseases. First the child with a retinal disease starts to see in dim light after an abnormally long waiting. Therefore he will have difficulties in finding his/her clothing in a closet or in a drawer if there is no extra illumination directed into these places. Later (s)he loses night vision completely, even when waiting for a long time (s)he does not start to see in the dark.Changes in visual adaptation time can be easily detected with the CONE Adaptation Test.
Photophobia and delayed adaptation to bright light are often additional symptoms of abnormal visual adaptation. Wheormally sighted persons enter from a darker room into a bright light, they also see very little for a second, sometimes it even hurts their eyes. They are dazzled. A visually impaired person may be dazzled for a long time. It is possible to decrease the problem by using absorptive glasses and a hat with wide brim or a visor.
Color vision
There are three different types of the retinal cone cells: some cells are most sensitive to red light, other to green light and the third type is most sensitivie to blue light. Also the “normally sighted” individuals may have minor difficulties with color perception. It is often called color blindness but the term is poorly chosen because these persons are not blind, many of them are unaware that they have anything abnormal with their vision. However, if they compare such colors as moss green, snuff brown, dark purple, and dark grey, all these color may look more or less the same. Small deviations from normal affect only some specific working conditions. That is why colour vision is examined at school before students get advice in career planning.
The screening examination uses pseudoisochromatic plates. Most commonly used test is called Ishihara’s test. Screening tests are very sensitive and detect even minor deviations from normal color perception. They do not measure the degree of deviation. For the diagnosis of deviant color perception another test is necessary, a quantitative test in form of small caps with color surfaces in all colors of the spectrum. The diagnosis of color deficiency should never be based on a screening test. If a child seems to have any confusion with colours, colour vision should be examined carefully. It can be started with clear basic colours to teach the concepts similar/different in relation to colors, after which quantitative testing is possible.
Young children may train for the quantitative test by playing the Colour Vision Game. Major colour vision deficiencies are revealed already in this game but the diagnose requires proper measurement using pigment tests.
Binocular vision and three dimensional vision
We have two eyes but see only one picture, image. Visual information coming from the two eyes is fused into one image in the visual cortex. Not all normally sighted have binocular vision. They do not use both eyes simultaneously, together. Some persons look alternatingly with their right or left eye. They are usually unaware that they use their eyes separately. It does not disturb them.
Stereovision or three dimensional vision means that we have depth perception iear vision. When we look far away we have another kind of depth perception. We pay attention to the relative size of objects and which object is partially hidden behind another object. The speed of movement with which an object seems to move when we move our head or move around (called parallax) gives us clues on the distance. Therefore persons who do not have stereovision can still assess depth.
Dominant eye
Dominant or leading eye is the eye that we use when we look very carefully at near or at far and can use only one eye. Even when both eyes are used simultaneously one of the eyes is more dominant than the other. We have hand, foot, and eye preference.
Eye motility and its disturbances
Eye movements are usually well controlled. The eyes look at the same object. Eyes turn because of the function of six eye muscles. If one of the eye muscles is paralysed, the eye turns in an abnormal position, the person sees double images (Fig.24).
|
|
Fig.24. Eye muscles seen from above. The left outer muscle has developed palsy, the left eye turns inward. |
If an eye muscle is not functioning properly the person sees double when trying to look in the direction where the muscle should function. When the eyes are turned in the opposite direction the double image is fused again. The eye with the disturbed motility is covered until the muscle function returns to normal.
Sometimes there is no disturbance in the muscles themselves but the command to turn eyes in a certain direction is not handled normally because of changes in brain function.
Variation in the nature of visual disability
Different visual functions may become impaired independent of each other. Therefore there are many different types of visual impairement and disability. Sometimes a visually impaired person seems to function in a very confusing way. One moment (s)he seems to function like a normally sighted person and in the next moment like a blind person. A visually impaired person seldom pretends to see less than what (s)he actually sees.
One reason for variation in visual behaviour might be changes in illumination. Another may be that (s)he knows the surroundins so there is no difficulty in orientation. Normally sighted move about the same way at home in the dark. They move confidently and securely as long there is nothing unexpected in their way. If somebody leaves an object on the usual path they may trip over it. In the very same way a visually impaired persoeeds only a few visual cues in a well known place in order to be able to move freely.
If it is difficult to understand how a visually impaired person sees it is quite proper to ask him/her about his/her vision. Most visually impaired people are able to describe the nature of their impairement so well that it is possible to understand their situation better. Some persons say that they have only 10% vision left. Such a number does not describe the degree of visual impairment. The person may be able to move freely relying on his/her vision or may function like a nearly blind. That number (10%) usually means that his/her visual acuity is 20/200 (6/60 or 0.1) and it describes only one of many visual functions.
If the loss of visual functioning is caused by brain damage, the behaviour of the person may look even more perplexing than when the loss is caused by changes in the eyes. In the higher visual functions, perceptual functions, small specific areas of the brain cortex are responsible for specific perceptions. If such an area with specific function is damaged, the corresponding function is either weak or completely lost. Thus an otherwise normally sighted person may not recognize people, not even close relatives. (S)he sees faces but cannot connect the visual information with pictures of faces in his/her memory.
There can be an isolated loss of motion perception, so that the person cannot tell whether a car is moving or not, or in milder cases, may perceive some movement but not how fast the car may be approaching. Colour perception may be disturbed. Recognition of geometric forms may be lost and thus learning letters and numbers may be impossible.
The structure of egocentric space may be lost and thus concepts like ‘on the right’, ‘on the left’, ‘in the middle’, ‘next’, may be difficult. Also drawing of simple pictures or even copying pictures of angles may be impossible.
It is important that these children/adult persons are not diagnosed as intellectually disabled if they have other functions where they functioormally. An uneven profile of functions should always lead to a thorough assessment of all cognitive visual functions and auditory perception. Children with loss of recognition of facial features or facial expressions are sometimes diagnosed as autistic, which is a tragic error and may negatively affect the child’s future.
VISION DEVELOPMENT IN CHILDREN
Infants see immediately after birth and look around. They become skilled users of their vision during the first few months of life and develop eye-hand coordination. Both eyes normally look at the same object. If the child’s eyes do not look at the same object the child is said to have strabismus or squint. He/she may then use his/her eyes alternatingly or only one eye all the time. If the child uses only one eye the other eye becomes a “lazy” eye, an amblyopic eye. A lazy eye cannot use central vision normally. It is important to diagnose a lazy eye early and to teach the infant to look with his lazy eye, too. Otherwise that eye will never see well.
If an infant before the age of six months seems to have crossed eyes all the time he/she should be seen by an ophthalmologist soon, not after several weeks. Even an intermittent crossing of eyes in children older than 6 months should be examined by an ophthalmologist.
When the eyes are intermittently crossed the infant sees double. Therefore he/she will accept the use of correcting glasses. If the crossing of eyes is allowed to develop manifest, i.e. present all the time, the infant no more sees double and may not accept the use of glasses.
In a family where one of the parents or older children has had strabismus or lazy eye, the younger children should be seen by an eye doctor at an early age, i.e, usually before they are 8-9 months old. It may be possible to prevent the strabismus or the lazy eye from developing if the infants get glasses early enough.
How can we observe an infant’s vision at home?
It is very difficult to notice a squint (strabismus) if the eye does not turn in or out very much. Also, some infants seem to have crossed eyes even though their eyes are straight because the distance between the eyes is small and the folds at the inner corner of the eyes are still prominent, so the eyes seem to be too close to the nose.
Fig.25a. When an infant has big eyes and nasal folds are still prominent, the infant may seem to have inward squint, “crossed eyes”, especially when the head is slightly turned. Note that the light reflexes are in the middle of both pupils, the eyes are looking in the same direction.
Whenever the parents are uncertain whether the eyes of their infant are straight it is always better to let an eye doctor check the situation. After the age of 3 months the eyes are usually straight most of the time and after the age of six months all the time. Constant squint is an abnormal situation at any age.
At the age of 3 months the infant starts to play with his/her hands. Hand regard is important and teaches spacial concepts and eye-hand coordination.
If you feel that one of the baby’s eyes might be a lazy eye, you can observe the child’s reactions when you cover the eyes one at a time (Fig.25 and in the video Lea Symbols -Assessment of vision in pre-school years).
|
|
Fig.25. Cover test. When you cover a lazy eye with a small card or your hand without touching the skin, it may not disturb the child (A) as much as when the same card is brought in front of the other eye (B). If the child repeatedly tilts his/her head as if trying to look with eye behind the cover, the child should be seen by an eye doctor. Your hand coming from above is a better way of covering the eye. |
If an infant is very hyperopic he/she sees poorly at close distances. Observation on an infant’s behaviour when crawling on the floor is a good near vision test. If an infant does not recognize small bread crumbs, etc. he/she should see an eye doctor. When a hyperopic infant gets glasses his vision can develop normally.
Vision should be checked during the normal health screenings. If the child is afraid and does not cooperate with the nurse or doctor you may want to test the child’s visual acuity with a playing card tests at home. If amblyopia is discovered early the results of the treatment are usually good.
Eyes and vision at school age
During puberty many children become myopic, near sighted, and need glasses in order to see well at the black board. Their eyes have not become “worse” or “weaker”, they have become a little bit longer as they grew. The child’s eyes are normal and he/she sees well at close distances. Glasses are needed for distance vision.
The first glasses are usually so weak that the child does not need them except in the classroom. It is better to keep them in a hard case in the school bag during pauses and on the way to school so they do not become broken.
Headache and glasses
Headache in children is seldom related to refractive errors or glasses. The most usual cause is too small a breakfast or breakfast composed of fast absorbed carbohydrates only. Then the bloodsugar will be low in the late morning and cause headache by noon or early afternoon.
Some children have swollen mucous membranes in their sinuses (Fig.10) and have therefore headaches around the eyes. This can be found out also at home as described earlier. It is good old rule that a child with headaches should play outside, eat, and spleep regularly for two weeks. If he/she still has headaches he should be seen by a doctor.
What to think and say about children’s glasses ?
It is a common misunderstanding to think that eyes are “bad” if one “has to” use glasses. It is important to say to the child, now and then, that the eyes are normal so the child develops a positive self image.
Most children do not “have to use” their glasses at school age. They use their glasses as adults do, in order to see more clearly and comfortably. There are numerous situations where one does not need to have the sharpest vision. When one of the children gets glasses other children often want see how the glasses change the image. The eyes are not hurt if a child uses someone else’s glasses for a while.
Children’s distance vision is usually checked by the nurse at school every second year. Glasses may be in poor condition before that and have to be changed. Most opticians in Europe (in some countries optometrists) check the visual acuity if the glasses are brought in for adjustment of the frame. In childhood the usual time between the changes of glasses varies from a few months to 3-4 years.
Additional information on the development of vision is in the chapters My Sight is Important and Follow-up of vision development.
Eye accidents
Accidents are far too common among children, especially young boys. They play with sharp knives, darts or sticks that can hurt their eyes. Even scissors and a regular fork may be dangerous in the hand of a young child. Sports and games also cause accidents. In ice hockey the children should always wear a face mask and in squash protective frames. Fireworks can be very dangerous in children’s hands and the home made “bombs” even more hasardous.
DYSLEXIA – READING DISORDERS
We talk about dyslexia if a child with normal intelligence, sight and hearing does not learn to read and write at the usual age. He sees the word but does not adequately process the visual image within his brain, does not find the corresponding spoken word. Children with dyslexia are often brought to the eye doctor with the hope that glasses might improve reading. Reading glasses seldom help to solve the learning problems. If they help at all, e.g. by balancing esophoria, inward squint, they are worth using because the situation is a burden to the child. However, they should not delay the use of a program of special instruction by a trained teacher or learning specialist.
Dyslexia is only one of the numerous forms of reading difficulties. Therefore a child with delay in learning to read needs a thorough neurologic and neuropsychologic assessment. Before those examinations, vision and hearing should be carefully evaluated.
Some children with good auditory memory learn better if they listen to the text while following the text with their finger. An adult can read passages on tape and the child can listen them as many times as needed without being dependent on when the adult is willing or has time to read. The child may also listen to the text that will be dealt with at school on the next day. In this way some of these children can keep up with their classmates. – Children with difficulties in attention or fixation can be helped with holding a card below the line of text or using a small “reading window” to reduce interference by the surrounding text. Special educators should get a comprehensive description of a child’s visual and learning problems for planning of therapeutic or remedial teaching.
REFRACTIVE ERRORS
The eye is a small ball but it is not a perfectly regular ball. Therefore there are small refractive errors that can be corrected with glasses.
Eyes without any refractive errors are rare. An eye without any refractive error sees clearly at far distance when its lens is relaxed. When such an eye looks at a close distance the lens has to accommodate, become thicker. If one then wants to look at a far distance the picture is first blurred for a brief moment and then becomes clear because it takes time before the lens is relaxed, flat again.
Fig.26.
A. A hyperopic, far sighted, eye with its lens relaxed, the image is not in focus at the level of the retina (the lines do not cross at the retina).
B. The image becomes clear when the lens accommodates, becomes thicker and makes the light rays bend more so they now cross at the retina.
C. In a myopic, near sighted, eye the image of a distant object is in the vitreous and the image at the retinal level is blurred. Accommodation does not make the image clear. The myopic eye sees objects close by clearly.
Hyperopia is very common. The lens of a hyperopic eye is accommodated some when the eye looks at far distance and it has to be accommodated more when the eye looks at near. If the hyperopic eyes get tired when looking at reading distance the use of reading glasses can be started at any age. Reading glasses are plus lenses, thicker in the middle than at the edge.
Myopia cannot be compensated by accommodation. A myopic person sees better at distance when squeezing the eye lids to a narrow opening which functions as an optic slit. It is not dangerous. Myopia is corrected with minus lenses, thicker at the edges than in the middle of the lens.
Astigmatism means that lines in different directions are not in focus at the same time, e.g. the vertical lines are in focus at the retina but the horizontal lines are not, and when the horizontal lines are in focus the vertical lines are not. The image is made clear by using cylinder lenses.
Irregular refractive errors are common among the visually impaired. If the cornea has irregular surface or the lens focuses the light irregularly, parts of the image are clear and some other parts distorted or blurred. Sometimes contact lenses make the image much better but not always. In other cases corneal transplantation or removal of the cataractous lens improves the image quality.
AGE RELATED CHANGES IN EYES AND VISION
All tissues become old with age. The age related changes are usually minimal in the eyes. Changes in the lens lead to lenghtening of the reading distance until one cannot read without glasses. This phenomenon is called presbyopia.
Lens may become cloudy which is called cataract. Also the retina changes with age, some of the capillaries become closed and part of retinal cells die. Changes that occur in the central retina, in the macula, may cause a decrease of visual acuity and contrast sensitivity. Then stronger glasses (with short focus) are needed and one has to read at a shorter reading distance.
It is a common misunderstanding that elderly persons should use their eyes sparingly. Vision does not wear out by being used. Even if there is some decrease of vision it is quite all right to use it as much as is pleasant. If the reading distance is very short the reading posture may be tiring. Therefore it is wise to discontinue reading now and then and move a little around. A few rounds around the arm chair or back and forth to the kitchen increases blood circulation and may make vision clearer for a while. A good reading lamp is a useful aid.
More about old age for colleagues and psychologists.
|
|
Age does not affect fine lace making if glasses are fitted to the working distance and enough light is available. |
SPECTACLES
Refractive errors exist in all populations. More than a thousand years ago “glasses” made out of metal were used in India. These metal plates had dozens of small holes in the middle (Fig.27) and thus functioned as pinhole glasses. A very small hole neutralizes the refractive errors of the eye.
Fig.27. “Glasses” made of metal were used in India.
There are now numerous types of glasses. Since the selection is so large, lenses and frames should be fitted carefully, so the glasses are comfortable.
Lenses are made by many factories and thus are different even if their refractive power, the number of the lens, is same. If the optician chooses another factory’s lenses, they may cause funny sensations even if the prescription did not change. Therefore, if you are happy with your present prescription ask the optician to choose similar or the closest similar lenses for your next glasses.
The tilt of the lenses is an important factor in fitting of the frames. Quite often uncomfortable glasses become comfortable after minor correction of the tilt. Glasses should always be made so that they are comfortable.
A B
C D
Fig.28a. Glasses are not always properly fitted. These pictures show common mistakes. A and B. Too weak a frame for -10 lenses and too little tilt of the lenses make this pair of glasses uncomfortable. The lenses should be tilted so that the line of gaze goes perpendicularly through the lens when reading. C. Too big frames are a common finding among people with intellectual disabilities. The frames touch the skin, lenses get therefore easily foggy and the frame may cause allergic reactions. The optic centre of the lens is in wrong place. D. When the lenses are bifocals, the reading part needs be placed at proper height in the lenses. In this pair they are uncomfortably low.
|
|
Fig.28 |
Persons who use glasses all the time need bifocal or progressive glasses when they become presbyopic. It is, of course, possible to have two separate pairs of glasses if the change from one type of glasses to the other type of glasses is infrequent. Later one might want to have trifocal glasses or progressive glasses. The fitting of the lenses is critical. If the lower part of the glasses, the reading segment, is placed too low the person has to bend his neck backwards when reading.
Fig.29.
Important distances to be measured when reading lenses are prescribed for a presbyopic person. Even a work station with numerous visual targets can be arranged so that regular multifocal lenses function well. The lenses chosen by the optician/optometrist should fit the work and the desk organized to fit the lenses. Therefore it is important that the work station is adjusted before new glasses are fitted and that the ophthalmologist/optometrist and the optician get correct information on the structure of the work station – and the placement of computer and other visual targets at home.
Multifocal glasses are fitted best if the optician knows at which distances and at which levels the person has to look during the day (Fig.29). When these measurements are done it is crucial that the person sits as (s)he is used to sit at the desk or working place. The height of the chair and the desk are checked and the working materials arranged at suitable distances and at correct height, i.e. so low that they can be easily seen through ordinary lenses (bi- or trifocal or progressive).
If the reading segment is placed low the person is forced to hold his head tilted backwards with his chin up [Fig.30, 1]. Too strong a reading correction forces the person to bend closer to the text. This often causes lower back pain [Fig.30, 2]. In most working places the person has to see clearly materials on the desk, the terminal surface and a table or other information further away on the wall. The lenses can be chosen so that all these targets can be seen in a comfortable head posture.
Fig.30.
Effect of lens design on ergonomy. 1. If the screen is placed too high and a presbyopic person has regular correction, bifocal or progressive, (s)he must have the chin uncomfortably high to look through the reading part of the lens. 2. If the reading part of a bifocal lens is too strong the person must lean forward to see the screen clearly. This causes lower back pain.
Fig.30.
3. Changing the gaze from the screen to the documents requires nodding and increases neck pain. 4. Even with ‘special’ progressive near vision lenses nodding is present.
Fig.30.
5. By placing the screen lower head posture becomes comfortable. There is little difference between special near vision lenses (5) and regular progressive lenses (6).
It is possible to tint the lenses in order to decrease photophobia caused by retinal diseases or opacities in the lens or cornea. Since it is difficult to choose the colour and the darkness of the lenses in the shop, it would be helpful if the optician would lend several demonstration lenses for a few days. The lenses could be used indoors and outdoors in bright sun light, in shade, during twilight and cloudy weather to find out the best ones.
Contact lenses are used increasingly often. Soft contact lenses are especially useful as sport glasses. They have to be cleaned carefully. If the eyes are irritated or the person has a common cold, it is best to use regular glasses in order to avoid corneal infections. A practical solution is to use disposable contact lenses, lenses that are used only nce. then there is no risk of infection and no problems of cleaning and desinfection.
You have certainly seen a number of articles about refractive surgery and how the cornea can be modified by surgery so glasses are no longer necessary. These operations cannot correct all refractive errors and sometimes the scars of some of these operations may decrease vision may disturb at night when the pupil is large. The quality of vision, especially contrast sensitivity, may not be as good as it was originally. Many who want to get rid of their glasses are mildly myopic. They do not consider that if they get the refraction corrected for distance vision, they will need reading glasses when they become older. With myopic eyes one can read without glasses even when old. It is also important to remember that after some operations it is necessary to have glasses all the time when outdoors to reduce the risk of scar formation.
It is not generally known that refractive surgery may cause problems in the alignment of the eyes, the person may develop strabismus. A typical situation is a person with myopia -3.0 diopters who has always read without glasses. After refractive surgery he did not need glasses for seeing at distance but needed reading lenses because otherwise he had intermittent diplopia, crossed eyes part of the time. He could not accept half frames so he now has to use expensive progressive lenses instead of the simple -3.0 lenses he used before the operation.
STRONG READING GLASSES, MAGNIFIERS, TELESCOPES, LAMPS
Whenever regular reading glasses are too weak, it is possible to try reading with stronger lenses at a closer distance. It makes the image larger.
Reading with strong reading glasses may become so tiresome that a TV-magnifier or a CCTV, closed circuit TV, is a more comfortable solution. There are different rules and regulations in different countries and states that require the visually impaired person himself to pay for some devices and subsidize some. The local representative of the organisation for the visually impaired, or the local deaf-blind worker, and your social worker should know how to get different visual aids and where to learn to use them properly.
|
Fig.31. Different reading glasses for a visually impaired person. Click at the link to see the reading position. |
|
Magnifiers are useful aids. A normally sighted person can use them when looking at something very small. Rod-formed magnifier in Fig.32.B is an inexpensive, yet useful present to be placed next to the telephone directory.
|
|
Fig.32. Different magnifiers. |
Although the Figure 32 was drawn in early 1980s the basic structures of magnifying lenses are still the same. Some convenient new magnifiers are now available, like the one in Figure 32a A for reading phonebook texts and the one in Figure 32a B to read the small texts describing the ingredients of food in packages.
When optical magnification is insufficient electro-optical magnification is possible. Use of computers makes the changes of the size of text easy either by changing the font size or by using specific programs to increase the text size.
|
|
Telescopes are used for reading street names, reading from the black board, and in different working places. Telescopes fitted on frames (Fig.33) are comfortable when the person is watching television or in a theater or at a sports event. |
Lamps are important visual aids for the visually impaired. Regular incandescent light is often sufficient if placed close enough.
Some visually impaired people prefer fluorescent light, especially if the reading distance is very short and the lamp has to be kept close to the face (Fig.34).
|
|
Fig.34. A fluorescent lamp is not hot and can be very close to the face of a visually impaired child. This child has a special slanted table for better ergonomics. |
The short reading distance may cause heart problems in the elderly. It is wise to use a supporting surface or a book rack. There are numerous different devices to be used for holding texts, also for those who read in bed.
We want everyone to be able to read comfortably; the visually impaired are no exception. Their visual aids should be chosen and fitted very carefully and these should be given after training to make sure they can be used for longer periods of time.
REHABILITATION OF THE VISUALLY IMPAIRED HEARING IMPAIRED PERSONS
The programs for the rehabilitation of the visually impaired hearing impaired or deaf persons vary in different countries and states. Again, the local representatives of the organisations for the visually impaired, for the hard of hearing or for the deaf should be able to help you to locate and get the services.
When a person starts to loose vision, moving around becomes problematic; many persons give up their daily promenades. It is very important not to give up but to try to find somebody who can escort during the promanade.
Hearing impaired visually impaired persons who work need special solutions for their working tasks. Independent living is difficult. Therefore there are group homes where several deaf-blind persons may live usually with deaf sighted persons.
The number of hearing impaired children who have congenital visual impairment is very small. They require very special teaching in order to learn to communicate. The other group of hearing impaired children who become visually impaired in school age, the Usher-children should be found among the hearing impaired children as early as possible so that their individual educational plans can be made and their language skills can be developed optimally.
IN THE EYE DOCTOR’S OFFICE
When leaving for the doctor’s appointment remember to take all old glasses and prescriptions, both for medications and glasses. It is also good to take copies of documents that should be discussed during the visit. If there is a need for new reading glasses, it is important to measure the distances used at work and at home (more about regular reading glasses and strong reading glasses, magnifiers etc.).
Sometimes the doctor may ask a question that is difficult to understand. If you feel the question is not clear enough you can always ask the doctor to try to ask the same question in other words. All interpreters have some schooling in medical interpretation but not particularly much in ophthalmology so your interpreter may have difficulties in transcribing the question.
As the doctor fits the glasses (s)he may ask several times “Is this better?” It may sound as if (s)he did not believe what you said but that is not the case. Even if the question is the same, (s)he asks different things since (s)he makes small changes in the glass correction between the questions. The doctor tries to find out what is the most comfortable glass for your eye. Quite often the change in the glass correction is so small that the doctor is hesitant whether (s)he should prescribe new lenses or not. New lenses are prescribed only if you feel that the change is worth paying the price. Therefore you may be asked to compare the new lenses with your old lenses.
When the glasses are correct, the doctor measures several visual functions: visual acuity, contrast sensitivity, colour vision, visual field, and function of the muscles of the eye. After these measurements the intraocular pressure is measured. First the eye is anesthetized with drops. Then the pressure is measured with the small blue light. During the measurement one must not blink. Most often the eyegrounds are examined after dilatation of the pupils. The dilating drops are dropped into the eyes. After that one has to wait for half an hour or more until the pupils are dilated.
Since the effect of the dilating drops is long lasting, one may be badly dazzled when coming out. On a sunny day we must remember to take sun glasses with us when we go to the eye doctor.
After dilatation of the pupils the intraocular pressure may rise in some patients. Sometimes the pressure rises after several hours, and the eye starts to ache and become reddish; the vision may become blurred. If the eye doctor is no more in his/her office, the emergency clinic gives the initial treatment. The patient’s doctor continues the treatment the day after.
We should remember that the visit to the eye doctor does not protect the patient from any diseases. There is no magic about the visit. If there are any new symptoms in the eyes or vision even the next day after the visit, it is important to contact the doctor and tell him about the new symptoms.
Ophthalmologists and Optometrists
Both ophthalmologists and optometrists take care of eyes and vision. Ophthalmologists examine your eyes to find the diagnosis of the disease that you might have. They perform surgery if needed and prescribe medicines. During the examination they measure the refraction of your eyes and often prescribe glasses for you.
The work of the optometrists varies in different countries. Their major work in most places is to prescibe glasses but in some states in the United States they take care of minor illnesses, too. In other countries there are no optometrists or only a few. If you have decreased vision, you should choose an optometrist who has knowledge of special lenses and other visual and environmental devices for the visually impaired.
When should you go to an ophthalmologist and when to an optometrist? Ask your doctor during the visit when you should be seeext time. Young healthy persons do not need to go to an ophthalmologist or an optometrist often, once in five years or not at all. If the person wears glasses, (s)he goes to the optometrist when the lenses are scratched or become uncomfortable. Elderly persons go more often if there are age related changes in their eyes that might require treatment in the future.
Many people believe that tiredness and burning sensation in their eyes are caused by old glasses. The symptoms may be caused by an illness and should be checked by the ophthalmologist. Not all symptoms are caused by weak glasses.
EYELIDS AND TEAR CHANNELS
Eyelids protect the eyes from drying and from getting flying particles into them.
|
Fig.4. Cross section of the eye lid and the eye. Sebaceous glands have their openings at the root of the eye lashes. If such a gland is inflammed it is called “hordeolum” or sty. Meibomian glands are imbedded in the cartilage of the eye lid. |
|
Meibomian Glands secret oil. If the long, thin opening of the gland becomes occluded, the gland continues to secret and a small nodule is formed in the eyelid. It may become inflammed. Usually it disappeares in a few weeks. If not, it is removed through a small wound in the skin or in the conjunctiva, the mucous membrane.
Since there are only 30 or so Meibomian glands in each eye lid, it is important to prevent inflammations in them. If most of them are destroyed by inflammations, too little oil is secreted by the remaining Meibomian glands. The oil normally covers the tear layer and decreases evaporation. If too little oil is secreted, the tear layer evaporates quickly and the cornea may get dry spots.
Tear glands secret tears. The glands are located near the eyes behind the outer upper rim of the bony orbit. Tears flow down over the eye and into the tear channels in the inner corner of the eye lids. The tear ducts are hair thin and therefore easily blocked. If there is swelling of the mucous membrane of the nose, eyes usually become watery and irritated.
|
|
Fig.5. Tear gland and tear passage into the nose. Tear gland is in the upper outer corner near the eye. Tear ducts and tear sac are in the inner corner of the eye. |
Tears are sucked into the tear ducts because of the low pressure in the tear sac during movements of the eyelids. They are pumped out of the tear sac into the nose by the same movements. If a person has facial nerve palsy the eye lids move less thaormally, the eye is watering. If the lower lid is hanging badly, the corneal surface may become too dry despite the watering.
|
|
Figure 5a . ‘Butterfly’ tape is an effective way of keeping the lower lid in a better position in the acute phase of facial nerve palsy. |
The hanging lower lid can be supported by tape as the first aid to decrease drying of the cornea (Figure 5a). If the nerve palsy is permanent, an operative correction of the lower lid may be necessary.
It is possible to measure the movement of the tears by using a special colour. A small amount of the colour is placed on the surface of the eye. After that it is measured how soon the colour arrives into the nose. The tear passages can be examined using x-ray techniques, too.
The surface of the eyes often becomes irritated in cold weather. The eyes start watering. Tear passages do not need to be occluded. There are just too many tears. The best thing to do is to protect sensitive eyes from the cold wind. Side shields (Fig.6) help a lot. A hood is the most effective protecting device on a windy day. It prevents the wind from getting between the spectacles and the eye.
Fig.6. Side shields are fixated on the spectacles.
Figure 6a. You may make the side shield yourself. Cut a piece of paper like the one in Figure 6a. Cut two slits in it and thread it on the side part of your glasses. If the form of the side shield fits your face, cut it in clear plastic, otherwise modify the form for better fit. Note that the edge of the side shield is at the level of the front surface of the glasses to prevent the wind from getting between the lens and your eye.
Tear film on the cornea has three layers: oil, water and mucus.
|
Fig. 7. Structure of the tear film. There is a thin layer of mucus on the surface of the cornea, on it there is a layer of water that contains salts. The outermost layer is a thin layer of oil that decreases evaporation of water, and thus drying of the corneal surface. (A better picture you get by clicking here.) |
|
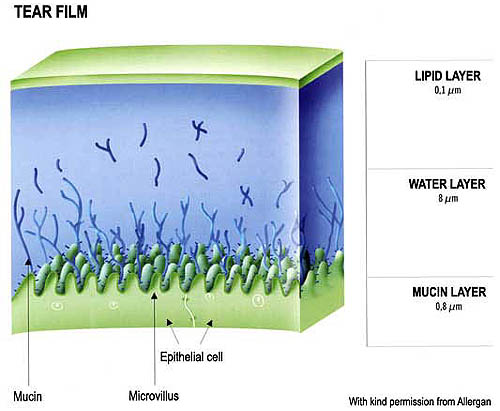
The surface cells of the cornea are hydrophobic, which means that waterdrops will not spread on such surface but roll aside. The thin layer of mucus is needed for making the surface hydrophilic, the layer of water can then spread evenly on the corneal surface.
If the mucus layer is uneven, some patches on the cornea have no mucus on the surface. The water layer rolls aside, the surface dries and wrinkles a little. This stretches the nerve endings and causes a sticking pain in the eye.
Changes in the structure of the tear film are common. Eyes are somewhat dry and irritated, now and then there is a sensation of sticking pain. The therapy is very simple: the corneal surface is protected with artificial tears or a very thin layer of ointment. It is always advisable to use a glas rod to apply ointments and all thicker drops into the eye. Otherwise, if one applies directly from the tube or the dropper, the amount of thick fluid or ointment is too big, the layer will be too thick and vision will be blurred.
|
|
|
Fig.8. Apply the ointment like this: apply a very small amount, |
STRUCTURES SURROUNDING
THE EYE
The eyes are moved by six eye muscles. Normally the eyes move so that both eyes look on the same object. The control of eye movements is usually very accurate.
|
|
Fig.9. Eye muscles. Right eye as seen from above. Two muscles below the eye are not seen. |
If the coordination of eye movements is disturbed and the eyes look at different objects, the person has strabismus or squint. If the eye turns in, the person is cross-eyed. If the eye turns out, the person is wall-eyed.
The space between the eye muscles and the bony wall of the orbit is filled with loose fat tissue. This soft tissue functions like a cushion if the eye is hit by an object. Fat tissue decreases in the elderly persons, the eyes sink into the orbit and the eyes look smaller but they are not smaller.
The bony orbit surrounding the eyes contains several small cavities, sinuses. They are located in the forehead, in both cheeks and between the eyes.
|
Fig.10. The sinuses: above the eyes the frontal sinuses, between the eyes the ethmoidal sinuses, and below the eyes the maxillary sinuses. |
|
Inflammation in the nasal sinuses may cause pain. Inflammation in the sinuses between the eyes often radiates into the eye or both eyes. The eye itself looks normal, with no redness or other signs of irritation. Vision is normal. If one presses against the aching eye, the pain is relieved as long as the hand presses the eye. The pain is felt again as soon as the pressure is removed. This is typical pain caused by poor ventilation of the sinuses. If such a pain is felt, it is usually possible to relieve the pain by using nasal spray or pills that decrease swelling of the mucous membranes in the nose and by inhaling warm vapor.
If pain around the eye is related to an inflammation in the eye itself, the eye is usually red. A similar pain can be caused by inflammation of the optic nerve, but it usually causes a decrease in central vision and the pain gets worse when the eye moves or it is pressed.
Pain in or around an eye may radiate from the muscles of the neck or – more rarely – from the facial muscles, especially from the temporal muscle. The most common areas from where the pain radiates to the eye are seen in the Figure 10a.
|
|
Figure 10a. When muscles in the different layers of neck are irritated, the pain radiates to the skin and bones around the eye and to the outer part of the eye itself. |

Pain related to muscle tension in the neck decreases when the muscles are warm in a hot shower or during a sauna bath and then gently stretched.
Positions of teeth may change and cause change in the function of the maxillar joint and/or in the function of the muscles. This possibility should also be kept in mind when there occurs pain around the eyes.
|
Pain in and around the eye Inflammation: Acute glaucoma – the eye is red, vision may be blurred Sinus problem, decreased air pressure in the sinuses Muscle pain radiating from the neck or from the temporal muscle Changes in teeth, requires consultation by a dentist. |
The optic nerve leads from the eye to the optic chiasm. The optic chiasm is where some of the fibers cross. The optic tract proceeds from the optic chiasm to the lateral geniculate nucleus (LGN). The optic radiation leads from the LGN to primary visual cortex (V1).
There are two eyes, thus we illustrate two visual fields. The fixation point is the center of the visual field; it corresponds to the fovea. T he vertical meridian splits the visual fields into left and right hemi-fields. The horizontal meridian splits the visual field into upper and lower hemi-fields. The blind spot is the region of the visual field that corresponds to the optic disc.
Principle of lateralization: The right half of the brain receives sensory information from and sends motor commands to the left half of body. In the visual system, the right half of the brain receives information about the left half of the visual field (note: not just from the left eye). Note that the fibers cross over at the optic chiasm.
Visual Fields
Visual deficits due to lesions at different points in the pathway: Suppose someone comes in complaining of vision problems. Do you send them to an ophthalmologist or to a neurologist? Is the problem an eye disease? Or is it some central problem like a tumor pressing on the optic tract?
If the deficit is in only one eye’s visual field, send the patient to an ophthalmologist. If the deficit is in corresponding parts of both eye’s visual fields, then it is a central problem, and send the patient to aeurologist for an MRI or CT scan.
Lateral Geniculate Nucleus (LGN)
The LGN has:
- 6 layers.
- Cells have monocular input.
- Layers alternate inputs from each of the two eyes.
- The top four are parvocellular layers, two layers from each eye. Parvo (small) LGN cells receive inputs from (small) midget ganglion cells.
- The bottom two are magnocellular layers, one layer from each eye. Magno (large) LGN cells receive inputs from (large) parasol ganglion cells.
- The retinal (hereafter called “retinotopic”) map is preserved. Axons from the retina preserve their order.
- There is an entire map of a visual hemi-field in each layer of the LGN.
- The maps are in register in each layer.
LGN physiology
In the LGN, cells have center-surround receptive fields just like retinal ganglion cells. There is little or no information processing beyond that done in the retina, so what is the function of the LGN? Why not send axons directly to cortex? Nobody knows for sure. There are two compelling hypotheses that I know of:
1. The LGN brings retinotopic maps from both eyes into register to make it easy for cortex to combine inputs from the two eyes.
2. Only 10% of inputs to LGN come from the retina. 90% are modulatory inputs from cortex and the brainstem. The brainstem modulates the information flow from the eye to the visual cortex, for example, according to the sleep cycle. Cortical (feedback) inputs to LGN are not well understood but might have to do with attention. The LGN is a convenient bottleneck for these modulatory inputs from the brainstem and cortex. If you tried to send these projections from brainstem and cortex all the way back to the retina then you’d end up with a blind spot that was 10 times larger.
Primary Visual Cortex (V1)
The visual cortex is subdivided into a number of separate and distinct regions called visual cortical areas. Later in the semester we will discuss how these different cortical areas are identified and what their functions are. For now, we will concentrate only on the primary visual cortex (also called V1, shown in blue). V1 is located in the Calcarine sulcus in the medial occipital lobe of the brain (near the back of the head, just to the left and right of the middle). V1 is “primary” because the LGN sends most of its axons there, so V1 is the “first” visual processing area in the cortex. V1 processes the information coming from the LGN (as described below) and then passes its output to the other visual cortical areas which are (creatively) named V2, V3, V4, etc.
All 6 layers of LGN project to area V1 in cortex. The magno and parvo layers project separately in the input layers of V1, but then these parallel pathways (that originated in the retina) get pretty much completely merged in subsequent areas.
V1 retinotopic map
The figure below shows the results of an experiment in which an anaesthetized monkey viewed a flickering bulls-eye pattern, and was injected with radioactively labeled glucose. The glucose was taken up by active neurons. The animal was then sacrificed, and V1 was surgically removed and flattened. The flattened V1 was then used to expose radioactively sensitive film. The result is a picture of regions of activity evoked by the bulls-eye. As you can see, V1 maintains a retinotopic map.
In the intact human brain, V1 is located in the occipital lobe. The retinotopic map is laid out across the folded cortical surface in the gray matter of the Calcarine sulcus. The central (foveal) part of the visual field is represented at the very back and more peripheral regions of the visual field are represented further forward (anterior). The retinotopic map is lateralized so that the left hemisphere V1 represents the right half of the visual field and vice versa.
The retinotopic map in V1 is distorted so that the central 10 degrees of the visual field occupies roughly half of V1 (orange regions in the above diagram). This makes sense because of the poor acuity in the periphery (recall that peripheral ganglion cells have large dendritic trees and pool over many photoreceptors). The distortion is called cortical magnification.
The picture below is a simulation of the distortion from cortical magnification.
V1 physiology
David Hubel and Torsten Wiesel won the Nobel prize for discovering the functional organization and basic physiology of neurons in V1. They discovered three different types of neurons that can be distinguished based on how they respond to visual stimuli that they called: simple cells, complex cells, and hypercomplex cells. V1 neurons transform information (unlike LGN cells whose receptive fields look just like those of ganglion cells) so that they are orientation selective and direction selective.
V1 physiology movie (200 Mb QuickTime movie)
In class we viewed a video that demonstrates how Hubel and Wiesel classified the various cell types and mapped their receptive fields. You can download this movie (clicking above) but be aware that it is a large movie file. The video shows visual stimuli while recording from each of several V1 neurons. The electrode was connected to an amplifier, and output to a loudspeaker. The audio track allows you to hear the loudspeaker – each click corresponds to an action potential. The movie shows examples of a simple cell, complex cell, direction-selective complex cell and a hypercomplex cell.
Orientation selectivity: Most V1 neurons are orientation selective meaning that they respond strongly to lines, bars, or edges of a particular orientation (e.g., vertical) but not to the orthogonal orientation (e.g., horizontal).
These are data from Hubel and Wiesel’s early experiments on V1. The dashed rectantangles on the left indicate a V1 neuron’s receptive field. The superimposed lines are the stimuli that were used. For each stimulus (each line orientation), Hubel and Wiesel recording how many action potentials were produced by this neuron. The middle row are exampls of the electrophysiological recordings for each of the corresponding stimulus orientations. The diagonal orientation (the middle row) evoked the greatest response (largest number of action potentials). The graph on the right shows the result after a whole bunch of measurements like these for each of a bunch of lines. There is a peak response for one particular orientation and weaker responses for other orientations, falling of to zero when the line orientaiton is about 40 degrees away from the neurons favorite (preferred) orientation).
Direction selectivity: Some V1 cells are also direction selective meaning that they respond strongly to oriented lines/bars/edges moving in a preferred direction (e.g., vertical lines moving to the right) but not at all in the opposite direction (e.g., vertical lines moving to the left).
These are also data from Hubel & Wiesel’s early experiments. The arrows above each electrophysiological recording indicate the direction of motion. This V1 neuron responds best to up-right motion but not at all to down-left motion.
Simple cells
- respond best to elongated bars or edges.
- are orientation selective.
- can be monocular or binocular.
- have separate ON and OFF subregions.
- perform length summation (they have bigger responses with increasing bar length up to some limit, at which point the response reaches a plateau).
A simple model of simple cell responses, suggested by Hubel and Wiesel, is that each simple cell sums inputs from LGN neurons with neighboring/aligned receptive fields to build an elongated receptive field that is most responsive to elongated bars or edges.
Complex cells
- are orientation selective.
- have spatially homogeneous receptive fields (no separate ON/OFF subregions).
- are nearly all binocular.
- perform length summation.
Hypercomplex cells
Hypercomplex cells are like complex cells except there are inhibitory flanks on the ends of the receptive field, so that response increases with increasing bar length up to some limit, but then as the bar is made longer the response is inhibited. This property is called end-stopping. The upper graph shows the response of a complex cell as a function of bar length. The lower graph shows the response of a hypercomplex cell as a function of bar length.
Summary of V1 physiology
The orientation selectivity of visual processing and representation in V1 is evident also in perception. Look first at panel (b) in the below figure and you will see two vertical gratings. Next fixate on the horizontal bar in the middle of panel (c) and hold your eyes on that fixation for 30 seconds or so. Then look back at panel (b), fixating again on the horizontal bar in the middle of the panel. What do you see? Why? Finally, adapt for 30 sec or so on panel (a) and then look back at panel (b). What do you see and why?
V1 functional architecture
Hubel and Wiesel also discovered that the neurons in V1 are arranged in an orderly fashion. Neurons with similar response properties (e.g., the same orientation preference) lie nearby one another.
Columnar architecture: As one moves an electrode vertically through the thickness of cortex, one finds that most neurons have the same selectivity (e.g., the same orientation preference and eye dominance). Ocular dominance columns: As one moves an electrode tangentially through the cortex, one first finds cells that respond to left eye inputs, then binocular (responsive to both/either eye), then right eye, then binocular, then left again, etc. Orientation columns: As one moves the electrode tangentially in the orthogonal direction, one first find cells selective for vertical, then diagonal, then horizontal, etc. A hypercolumn is a chunk of cortex about
The notion of a functional columnar architecture is a big theme in cortical physiology. We’ll see other visual brain centers with analogous organization: area MT has a columnar architecture of direction selectivity for visual motion perception, area IT has a columnar architecture of complex shape/feature selectivity for object recognition.
The functional architecture of V1 has been studied extensively. Hubel and Wiesel’s initial results have been replicated in recent years using optical imaging methods. In optical imaging, you open a hole in the skull, point video camera at the brain, and collect images that reflect the relative amount of oxygenated (“red”) versus deoxygenated (“blue”) blood.
Top: diagram of optical imaging experiment and apparatus. Left image: picture of the brain while the animal views stimuli with the left eye (right eye patched/occluded). Then, one takes a picture of the brain while the animal views stimuli with the right eye. Right image: subtract one image from the other to get a picture that looks like zebra stripes – these are the ocular dominance columns.
Ocular dominance movie (12 Mb QuickTime movie)
In class we viewed a video that demonstrates the optical imaging procedure for visualizing ocular dominance columns. You can download this movie (clicking above).
Analogous experiment have been carried out, but using orientation (e.g., vertical versus horizontal) instead of eye input (right eye vs left eye). This gives a picture of the orientation columns in the monkey brain.
Ocular dominance columns are also present in human V1. This is a picture of a post-mortem human brain (medial view of the occipital lobe and the Calcarine sulcus). This patient had lost an eye before they died so only the neurons responding to the other eye were active. The patient had given permission for their brain to be removed and analyzed immediately after they had died. The brain was stained for cytochrome oxidase (an enzyme used in cellular metabolism) so the dark stripes correspond to brain regions that had been recently metabolically active. In other words, the dark and light stripes are this patient’s ocular dominance columns.
Amblyopia
Amblyopia, or cortical blindness, is a term that refers to a variety of visual disorders when there is no problem with the eye (the optics and retina are fine), but one eye has better vision than the other. Amblyopia can be caused by strabismus (wandering eye) if it is not corrected in infancy. What appears to happen is that during development, if the signals from one eye are weak or out of register with input from the other eye, then the brain develops in a way that ignores the signals from the weak or misdirected eye.
Hubel and Wiesel performed a classic experiment on this topic. They raised kittens with one eye sutured shut (monocular deprivation) and found that the ocular dominance columns did not develop properly. Instead, primary visual cortex organized itself to respond almost entirely to the undeprived eye. They found that there is a critical period during development up until the kittens are about 4 months old. Monocular deprivation during this period messes up the ocular dominance columns. Deprivation after the critical period has no effect. If the kittens were monocularly deprived throughout the critical period, then they could never regain the proper ocular dominance organization.
Consequently, we now know that we must intervene in infancy to prevent amblyopia. A wandering eye can often be corrected surgically, but not until a baby is old enough. In the meantime, one covers an infant’s good eye with a patch for a few hours each day so that the brain must rely on signals from the bad eye. This helps the brain develop properly to process signals coming from both eyes.


{kind=link}
{kind=link}
{kind=link}