Biochemistry of connective tissue: structure, properties, functions, regulation, pathology. Biochemistry of tooth tissues: structure, properties, functions, regulation, pathology
Biochemistry of saliva: sourses, functions, chemical composition, regulation and pathology of saliva secretion.
Connective tissue (CT) is a kind of biological tissue that supports, connects, or separates different types of tissues and organs of the body. It is one of the four general classes of biological tissues—the others of which are epithelial, muscular, and nervous tissues.
All CT has three main components: cells, fibers, and extracellular matrices, all immersed in the body fluids.
Connective tissue can be broadly subdivided into connective tissue proper, special connective tissue, and series of other, less classifiable types of connective tissues. Connective tissue proper consists of loose connective tissue and dense connective tissue (which is further subdivided into dense regular and dense irregular connective tissues.) Special connective tissue consists of reticular connective tissue, adipose tissue, cartilage, bone, and blood. Other kinds of connective tissues include fibrous, elastic, and lymphoid connective tissues.
Fibroblasts are the cells responsible for the production of some CT.
Type-I collagen, is present in many forms of connective tissue, and makes up about 25% of the total protein content of the mammalian body.
Functions of connective tissue
– Storage of energy
– Protection of organs
– Provision of structural framework for the body
– Connection of body tissues
– Connection of epithelial tissues to muscle tissues
Characteristics of connective tissue and fiber types
Cells are spread through an extracellular fluid.
Ground substance – A clear, colorless, and viscous fluid containing glycosaminoglycans and proteoglycans to fix the bodywater and the collagen fibers in the intercellular spaces. Ground substance slows the spread of pathogens.
Fibers. Not all types of CT are fibrous. Examples include adipose tissue and blood. Adipose tissue gives “mechanical cushioning” to our body, among other functions. Although there is no dense collageetwork in adipose tissue, groups of adipose cells are kept together by collagen fibers and collagen sheets in order to keep fat tissue under compression in place (for example, the sole of the foot). The matrix of blood is plasma.
Both the ground substance and proteins (fibers) create the matrix for CT.
Types of fibers:Tissue → Purpose → Components → Location
Collagenous fibers – → Alpha polypeptide chains → tendon, ligament, skin, cornea, cartilage, bone, blood vessels, gut, and intervertebral disc.
Elastic fibers → elastic microfibril & elastin → extracellular matrix
Reticular fibers → Type-III collagen → liver, bone marrow, lymphatic organs.
Structure and functions of collagen.
Collagen is a group of naturally occurring proteins found in animals, especially in the flesh and connective tissues of vertebrates.
It is the main component of connective tissue, and is the most abundant protein in mammals, making up about 25% to 35% of the whole-body protein content. Collagen, in the form of elongated fibrils, is mostly found in fibrous tissues such as tendon, ligament and skin, and is also abundant in cornea, cartilage, bone, blood vessels, the gut, and intervertebral disc. The fibroblast is the most common cell which creates collagen. In muscle tissue, it serves as a major component of the endomysium. Collagen constitutes one to two percent of muscle tissue, and accounts for 6% of the weight of strong, tendinous muscles. Gelatin, which is used in food and industry, is collagen that has been irreversibly hydrolyzed. Collagen is composed of a triple helix, which generally consists of two identical chains (α1) and an additional chain that differs slightly in its chemical composition (α2).

The amino acid composition of collagen is atypical for proteins, particularly with respect to its high hydroxyproline content. The most common motifs in the amino acid sequence of collagen are glycine–proline-X and glycine-X-hydroxyproline, where X is any amino acid other than glycine, proline or hydroxyproline.
Synthesis
First, a three dimensional stranded structure is assembled, with the amino acids glycine and proline as its principal components. This is not yet collagen but its precursor, procollagen. A recent study shows that vitamin C must have an important role in its synthesis. Prolonged exposure of cultures of human connective-tissue cells to ascorbate induced an eight-fold increase in the synthesis of collagen with no increase in the rate of synthesis of other proteins. Since the production of procollagen must precede the production of collagen, vitamin C must have a role in this step. The conversion involves a reaction that substitutes a hydroxyl group, OH, for a hydrogen atom, H, in the proline residues at certain points in the polypeptide chains, converting those residues to hydroxyproline. This hydroxylation reaction organizes the chains in the conformatioecessary for them to form a triple helix. The hydroxylation, next, of the residues of the amino acid lysine, transforming them to hydroxylysine, is theeeded to permit the cross-linking of the triple helices into the fibers and networks of the tissues.
These hydroxylation reactions are catalyzed by two different enzymes: prolyl-4-hydroxylase and lysyl-hydroxylase. Vitamin C also serves with them in inducing these reactions. in this service, one molecule of vitamin C is destroyed for each H replaced by OH. The synthesis of collagen occurs inside and outside of the cell. The formation of collagen which results in fibrillary collagen (most common form) is discussed here. Meshwork collagen, which is often involved in the formation of filtration systems is the other form of collagen. It should be noted that all types of collagens are triple helixes, and the differences lie in the make-up of the alpha peptides created in step 2.
1. Transcription of mRNA: There are approximately 34 genes associated with collagen formation, each coding for a specific mRNA sequence, and typically have the “
2. Pre-pro-peptide Formation: Once the final mRNA exits from the cell nucleus and enters into the cytoplasm it links with the ribosomal subunits and the process of translation occurs. The early/first part of the new peptide is known as the signal sequence. The signal sequence on the N-terminal of the peptide is recognized by a signal recognition particle on the endoplasmic reticulum, which will be responsible for directing the pre-pro-peptide into the endoplasmic reticulum. Therefore, once the synthesis of new peptide is finished, it goes directly into the endoplasmic reticulum for post-translational processing. Note that it is now known as pre-pro-collagen.
3. Alpha Peptide to Procollagen: Three modifications of the pre-pro-peptide occur leading to the formation of the alpha peptide. Secondly, the triple helix known as procollagen is formed before being transported in a transport vesicle to the golgi apparatus. 1) The signal peptide on the N-terminal is dissolved, and the molecule is now known as propeptide (not procollagen). 2) Hydroxylation of lysines and prolines on propeptide by the enzymes prolyl hydroxylase and lysyl hydroxylase (to produce hydroxyproline and hydroxylysine) occurs to aid crosslinking of the alpha peptides. It is this enzymatic step that requires vitamin C as a cofactor. In scurvy, the lack of hydroxylation of prolines and lysines causes a looser triple helix (which is formed by 3 alpha peptides). 3) Glycosylation occurs by adding either glucose or galactose monomers onto the hydroxy groups that were placed onto lysines, but not on prolines. From here the hydroxylated and glycosylated propeptide twists towards the left very tightly and then three propeptides will form a triple helix. It is important to remember that this molecule, now known as procollagen (not propeptide) is composed of a twisted portion (center) and two loose ends on either end. At this point the procollagen is packaged into a transfer vesicle destined for the golgi apparatus.
4. Golgi Apparatus Modification: In the golgi apparatus, the procollagen goes through one last post-translational modification before being secreted out of the cell. In this step oligosaccharides (not monosaccharides like in step 3) are added, and then the procollagen is packaged into a secretory vesicle destined for the extracellular space.
5. Formation of Tropocollagen: Once outside the cell, membrane bound enzymes known as collagen peptidases, remove the “loose ends” of the procollagen molecule. What is left is known as tropocollagen. Defect in this step produces one of the many collagenopathies known as Ehlers-Danlos syndrome. This step is absent when synthesizing type III, a type of fibrilar collagen.
6. Formation of the Collagen Fibril: Lysyl oxidase an extracellular enzyme produces the final step in the collagen synthesis pathway. This enzyme acts on lysines and hydroxylysines producing aldehyde groups, which will eventually undergo covalent bonding between tropocollagen molecules. This polymer of tropocollogen is known as a collagen fibril.
.svg)
Amino acids
Collagen has an unusual amino acid composition and sequence:
· Glycine is found at almost every third residue
· Proline (Pro) makes up about 17% of collagen
· Collagen contains two uncommon derivative amino acids not directly inserted during translation. These amino acids are found at specific locations relative to glycine and are modified post-translationally by different enzymes, both of which require vitamin C as a cofactor.
o Hydroxyproline (Hyp), derived from proline.
o Hydroxylysine (Hyl), derived from lysine (
Cortisol stimulates degradation of (skin) collagen into amino acids.
Collagen I formation
Most collagen forms in a similar manner, but the following process is typical for type I:
1. Inside the cell
1. Two types of peptide chains are formed during translation on ribosomes along the rough endoplasmic reticulum (RER): alpha-1 and alpha-2 chains. These peptide chains (known as preprocollagen) have registration peptides on each end and a signal peptide.
2. Polypeptide chains are released into the lumen of the RER.
3. Signal peptides are cleaved inside the RER and the chains are now known as pro-alpha chains.
4. Hydroxylation of lysine and proline amino acids occurs inside the lumen. This process is dependent on ascorbic acid (Vitamin C) as a cofactor.
5. Glycosylation of specific hydroxylysine residues occurs.
6. Triple ɣ helical structure is formed inside the endoplasmic reticulum from each two alpha-1 chains and one alpha-2 chain.
7. Procollagen is shipped to the Golgi apparatus, where it is packaged and secreted by exocytosis.
2. Outside the cell
1. Registration peptides are cleaved and tropocollagen is formed by procollagen peptidase.
2. Multiple tropocollagen molecules form collagen fibrils, via covalent cross-linking (aldol reaction) by lysyl oxidase which links hydroxylysine and lysine residues. Multiple collagen fibrils form into collagen fibers.
3. Collagen may be attached to cell membranes via several types of protein, including fibronectin and integrin.
Synthetic pathogenesis
Vitamin C deficiency causes scurvy, a serious and painful disease in which defective collagen prevents the formation of strong connective tissue. Gums deteriorate and bleed, with loss of teeth; skin discolors, and wounds do not heal. Prior to the eighteenth century, this condition was notorious among long duration military, particularly naval, expeditions during which participants were deprived of foods containing Vitamin C.
An autoimmune disease such as lupus erythematosus or rheumatoid arthritis[29] may attack healthy collagen fibers.
Many bacteria and viruses have virulence factors which destroy collagen (such as the enzyme collagenase) or interfere with its production.
Molecular structure
The tropocollagen or collagen molecule is a subunit of larger collagen aggregates such as fibrils. At approximately 300 nm long and 1.5 nm in diameter, it is made up of three polypeptide strands (called alpha peptides, see step 2), each possessing the conformation of a left-handed helix (its name is not to be confused with the commonly occurring alpha helix, a right-handed structure). These three left-handed helices are twisted together into a right-handed coiled coil, a triple helix or “super helix”, a cooperative quaternary structure stabilized by numerous hydrogen bonds. With type I collagen and possibly all fibrillar collagens if not all collagens, each triple-helix associates into a right-handed super-super-coil referred to as the collagen microfibril. Each microfibril is interdigitated with its neighboring microfibrils to a degree that might suggest they are individually unstable, although within collagen fibrils, they are so well ordered as to be crystalline.
A distinctive feature of collagen is the regular arrangement of amino acids in each of the three chains of these collagen subunits. The sequence often follows the pattern Gly–Pro-X or Gly-X-Hyp, where X may be any of various other amino acid residues. Proline or hydroxyproline constitute about 1/6 of the total sequence. With glycine accounting for the 1/3 of the sequence, this means approximately half of the collagen sequence is not glycine, proline or hydroxyproline, a fact often missed due to the distraction of the unusual GX1X2 character of collagen alpha-peptides. The high glycine content of collagen is important with respect to stabilization of the collagen helix as this allows the very close association of the collagen fibers within the molecule, facilitating hydrogen bonding and the formation of intermolecular cross-links. This kind of regular repetition and high glycine content is found in only a few other fibrous proteins, such as silk fibroin. About 75-80% of silk is (approximately) -Gly-
is rich in glycine, proline, and alanine (
Because glycine is the smallest amino acid with no side chain, it plays a unique role in fibrous structural proteins. In collagen, Gly is required at every third position because the assembly of the triple helix puts this residue at the interior (axis) of the helix, where there is no space for a larger side group than glycine’s single hydrogen atom. For the same reason, the rings of the Pro and Hyp must point outward. These two amino acids help stabilize the triple helix—Hyp even more so than Pro; a lower concentration of them is required in animals such as fish, whose body temperatures are lower than most warm-blooded animals. Lower proline and hydroxyproline contents are characteristic of cold-water, but not warm-water fish; the latter tend to have similar proline and hydroxyproline contents to mammals. The lower proline and hydroxproline contents of cold-water fish and other poikilotherm animals leads to their collagen having a lower thermal stability than mammalian collagen. This lower thermal stability means that gelatin derived from fish collagen is not suitable for many food and industrial applications.
The tropocollagen subunits spontaneously self-assemble, with regularly staggered ends, into even larger arrays in the extracellular spaces of tissues. In the fibrillar collagens, the molecules are staggered from each other by about 67 nm (a unit that is referred to as ‘D’ and changes depending upon the hydration state of the aggregate). Each D-period contains four plus a fraction collagen molecules, because 300 nm divided by 67 nm does not give an integer (the length of the collagen molecule divided by the stagger distance D). Therefore, in each D-period repeat of the microfibril, there is a part containing five molecules in cross-section, called the “overlap”, and a part containing only four molecules, called the “gap”. The triple-helices are also arranged in a hexagonal or quasihexagonal array in cross-section, in both the gap and overlap regions.
There is some covalent crosslinking within the triple helices, and a variable amount of covalent crosslinking between tropocollagen helices forming well organized aggregates (such as fibrils). Larger fibrillar bundles are formed with the aid of several different classes of proteins (including different collagen types), glycoproteins and proteoglycans to form the different types of mature tissues from alternate combinations of the same key players. Collagen’s insolubility was a barrier to the study of monomeric collagen until it was found that tropocollagen from young animals can be extracted because it is not yet fully crosslinked. However, advances in microscopy techniques (i.e. electron microscopy (EM) and atomic force microscopy (AFM)) and X-ray diffraction have enabled researchers to obtain increasingly detailed images of collagen structure in situ. These later advances are particularly important to better understanding the way in which collagen structure affects cell-cell and cell-matrix communication, and how tissues are constructed in growth and repair, and changed in development and disease. For example using AFM –based nanoindentation it has been shown that a single collagen fibril is a heterogeneous material along its axial direction with significantly different mechanical properties in its gap and overlap regions, correlating with its different molecular organizations in these two regions.
Collagen fibrils are semicrystalline aggregates of collagen molecules. Collagen fibers are bundles of fibrils.
Collagen fibrils/aggregates are arranged in different combinations and concentrations in various tissues to provide varying tissue properties. In bone, entire collagen triple helices lie in a parallel, staggered array. 40 nm gaps between the ends of the tropocollagen subunits (approximately equal to the gap region) probably serve as nucleation sites for the deposition of long, hard, fine crystals of the mineral component, which is (approximately) Ca10(OH)2(PO4)6. Type I collagen gives bone its tensile strength.
Types and associated disorders
Collagen occurs in many places throughout the body. Over 90% of the collagen in the body, however, is of type I.
So far, 28 types of collagen have been identified and described. The five most common types are:
· Collagen I: skin, tendon, vascular ligature, organs, bone (main component of the organic part of bone)
· Collagen II: cartilage (main component of cartilage)
· Collagen III: reticulate (main component of reticular fibers), commonly found alongside type I.
· Collagen IV: forms bases of cell basement membrane
· Collagen V: cell surfaces, hair and placenta
Collagen-related diseases most commonly arise from genetic defects or nutritional deficiencies that affect the biosynthesis, assembly, postranslational modification, secretion, or other processes involved iormal collagen production.
Diseases
One thousand mutations have been identified in twelve out of more than twenty types of collagen. These mutations can lead to various diseases at the tissue level.[39]
Osteogenesis imperfecta – Caused by a mutation in type 1 collagen, dominant autosomal disorder, results in weak bones and irregular connective tissue, some cases can be mild while others can be lethal, mild cases have lowered levels of collagen type 1 while severe cases have structural defects in collagen.
Chondrodysplasias – Skeletal disorder believed to be caused by a mutation in type 2 collagen, further research is being conducted to confirm this.
Ehler-Danlos Syndrome – Ten different types of this disorder which lead to deformities in connective tissue, some types can be lethal that lead to the rupture of arteries, each syndrome is caused by a different mutation, for example type four of this disorder is caused by a mutation in collagen type 3.
Alport syndrome – Can be passed on genetically, both an autosomal dominant and autosomal recessive disorder, sufferers have problems with their kidneys and eyes, loss of hearing can also develop in during the childhood or adolescent years.[43]
Osteoporosis – Not inherited genetically, brought on with age, associated with reduced levels of collagen in the skin and bones, growth hormone injections are being researched as a possible treatment to counteract any loss of collagen.[44]
Knobloch syndrome – Caused by a mutation in the collagen XVIII gene, patients present with protrusion of the brain tissue and degeneration of the retina, an individual who has family members suffering from the disorder are at an increased risk of developing it themselves as there is a hereditary link.[39]
Characteristics
Collagen is one of the long, fibrous structural proteins whose functions are quite different from those of globular proteins such as enzymes. Tough bundles of collagen called collagen fibers are a major component of the extracellular matrix that supports most tissues and gives cells structure from the outside, but collagen is also found inside certain cells. Collagen has great tensile strength, and is the main component of fascia, cartilage, ligaments, tendons, bone and skin. Along with soft keratin, it is responsible for skin strength and elasticity, and its degradation leads to wrinkles that accompany aging. It strengthens blood vessels and plays a role in tissue development. It is present in the cornea and lens of the eye in crystalline form.
Uses
Collagen has a wide variety of applications, from food to medical. For instance, it is used in cosmetic surgery and burns surgery. It is widely used in the form of collagen casings for sausages.
If collagen is sufficiently denatured, e.g. by heating, the three tropocollagen strands separate partially or completely into globular domains, containing a different secondary structure to the normal collagen polyproline II (PPII), e.g. random coils. This process describes the formation of gelatin, which is used in many foods, including flavored gelatin desserts. Besides food, gelatin has been used in pharmaceutical, cosmetic, and photography industries. From a nutritional point of view, collagen and gelatin are a poor-quality sole source of protein since they do not contain all the essential amino acids in the proportions that the human body requires—they are not ‘complete proteins‘ (as defined by food science, not that they are partially structured). Manufacturers of collagen-based dietary supplements claim that their products can improve skin and fingernail quality as well as joint health. However, mainstream scientific research has not shown strong evidence to support these claims. Individuals with problems in these areas are more likely to be suffering from some other underlying condition (such as normal aging, dry skin, arthritis etc.) rather than just a protein deficiency.
From the Greek for glue, kolla, the word collagen means “glue producer” and refers to the early process of boiling the skin and sinews of horses and other animals to obtain glue. Collagen adhesive was used by Egyptians about 4,000 years ago, and Native Americans used it in bows about 1,500 years ago. The oldest glue in the world, carbon-dated as more than 8,000 years old, was found to be collagen—used as a protective lining on rope baskets and embroidered fabrics, and to hold utensils together; also in crisscross decorations on human skulls. Collageormally converts to gelatin, but survived due to the dry conditions. Animal glues are thermoplastic, softening again upon reheating, and so they are still used in making musical instruments such as fine violins and guitars, which may have to be reopened for repairs—an application incompatible with tough, synthetic plastic adhesives, which are permanent. Animal sinews and skins, including leather, have been used to make useful articles for millennia.
Elastin – main protein of elastic fibrils, structure and biological role.
Elastin is a protein in connective tissue that is elastic and allows many tissues in the body to resume their shape after stretching or contracting. Elastin helps skin to return to its original position when it is poked or pinched. Elastin is also an important load-bearing tissue in the bodies of vertebrates and used in places where mechanical energy is required to be stored. In humans, elastin is encoded by the ELN gene.
Function
This gene encodes a protein that is one of the two components of elastic fibers. The encoded protein is rich in hydrophobic amino acids such as glycine and proline, which form mobile hydrophobic regions bounded by crosslinks between lysine residues. Multiple transcript variants encoding different isoforms have been found for this gene. The other name for elastin is tropoelastin. The characterization of disorder is consistent with an entropy-driven mechanism of elastic recoil. It is concluded that conformational disorder is a constitutive feature of elastin structure and function.
Clinical significance
Deletions and mutations in this gene are associated with supravalvular aortic stenosis (SVAS) and autosomal dominant cutis laxa. Other associated defects in elastin include Marfan’s Syndrome and emphysema caused by α1-antitrypsin deficiency.
Composition
Elastic fiber is composed of the protein fibrillin and elastin made of simple amino acids such as glycine, valine, alanine, and proline. The total elastin ranges from 58 to 75% of the weight of the dry defatted artery iormal canine arteries.[6] Comparison between fresh and digested tissues shows that, at 35% strain, a minimum of 48% of the arterial load is carried by elastin, and a minimum of 43% of the change in stiffness of arterial tissue is due to the change in elastin stiffness. Elastin is made by linking many soluble tropoelastin protein molecules, in a reaction catalyzed by lysyl oxidase, to make a massive insoluble, durable cross-linked array. The amino acid responsible for these cross-links is lysine. Tropoelastin is a specialized protein with a molecular weight of 64 to 66 kDa, and an irregular or random coil conformation made up of 830 amino acids.
Desmosine and isodesmosine are types of links for the tropoelastin molecules.
Tissue distribution
Elastin serves an important function in arteries as a medium for pressure wave propagation to help blood flow and is particularly abundant in large elastic blood vessels such as the aorta. Elastin is also very important in the lungs, elastic ligaments, the skin, and the bladder, elastic cartilage. It is present in all vertebrates above the jawless fish.
Structure and functions of proteoglycans
Proteoglycans (mucoproteins) are formed of glycosaminoglycans (GAGs) covalently attached to the core proteins.
They are found in all connective tissues, extracellular matrix (ECM) and on the surfaces of many cell types. Proteoglycans are remarkable for their diversity (different cores, different numbers of GAGs with various lenghts and compositions).
Glycosaminoglycans forming the proteoglycans are the most abundant heteropolisaccharides in the body. They are long unbranched molecules containing a repeating disaccharide unit. Usually one sugar is an uronic acid (either D-glucuronic or L-iduronic) and the other is either GlcNAc or GalNAc. One or both sugars contain sulfate groups (the only exception is hyaluronic acid).
GAGs are highly negatively charged what is essential for their function.
THE SPECIFIC GAGs OF PHYSIOLOGICAL SIGNIFICANCE ARE :
Hyaluronic acid (D-glucuronate + GlcNAc)
Occurence : synovial fluid, ECM of loose connective tissue
Hyaluronic acid is unique among the GAGs because it does not contain any sulfate and is not found covalently attached to proteins. It forms non-covalently linked complexes with proteoglycans in the ECM. Hyaluronic acid polymers are very large (100 – 10,000 kD) and can displace a large volume of water.
Dermatan sulfate (L-iduronate + GlcNAc sulfate)
Occurence : skin, blood vessels, heart valves
Chondroitin sulfate (D-glucuronate + GalNAc sulfate)
Occurence : cartilage, bone, heart valves ; It is the most abundant GAG.
Heparin and heparan sulfate (D-glucuronate sulfate + N-sulfo-D-glucosamine)
Heparans have less sulfate groups than heparins
Occurence :
· Heparin :component of intracellular granules of mast cells lining the arteries of the lungs, liver and skin
· Heparan sulfate : basement membranes, component of cell surfaces
Keratan sulfate ( Gal + GlcNAc sulfate)
Occurence : cornea, bone, cartilage ;
Keratan sulfates are often aggregated with chondroitin sulfates.
Structure of proteoglycans
The GAGs extend perpendicular from the core protein in a bottlebrush- like structure.
The linkage of GAGs such as (heparan sulfates and chondroitin sulfates) to the protein core involves a specific trisaccharide linker :
Some forms of keratan sulfates are linked to the protein core through an N-asparaginyl bond.
The protein cores of proteoglycans are rich in Ser and Thr residues which allows multiple GAG attachment.
Role of proteoglycans and glycosaminoglycans
They perform numerous vital functions within the body.
GAG dependent functions can be divided into two classes: the biophysical and the biochemical.
The biophysical functions depend on the unique properties of GAGs : the ability to fill the space, bind and organize water molecules and repel negatively charged molecules. Because of high viscosity and low compressibility they are ideal for a lubricating fluid in the joints. On the other hand their rigidity provides structural integrity to the cells and allows the cell migration due to providing the passageways between cells.
For example the large quantities of chondroitin sulfate and keratan sulfate found on aggrecan play an important role in the hydration of cartilage. They give the cartilage its gel-like properties and resistance to deformation.
Aggrecan is one of the most important extracellular proteoglycans. It forms very large aggregates (a single aggregate is one of the largest macromolecules known; it can be more than 4 microns long). Aggrecan molecules are non-covalently bound to the long molecule of hyaluronan (like bristles to the backbone in a bottlebrush). It is faciliated by the linking proteins. To each aggrecan core protein multiple chains of chondroitin sulfate and keratan sulfate are covalently attached through the trisaccharide linker .
The other, more biochemical functions of GAGs are mediated by specific binding of GAGs to other macromolecules, mostly proteins. Proteoglycans participate in cell and tissue development and physiology.
EXAMPLES OF GAG BINDING PROTEINS :
Secreted proteases and antiproteases
For example antithrombin III (AT III) binds tightly to heparin and certain heparan sulfates (so do its substrates). Thus they control the blood coagulation. In the absence of GAGs AT III inactivates proteases (such as thrombin, factors IXa and XIa) very slowly. In the presence of appropriate GAGs these reactions are accelerated 2000-fold.
GAGs are sufficiently long that both protease and protease inhibitor can bind to the same chain (thus the likelyhood of the two proteins binding to each other is increased enormously). GAGs also affect the protein conformation that contributes to improving AT III binding kinetics.
Polypeptide growth factors
Members of the FGF family, as well as several other growth factors, bind to heparin or heparan sulfate. Binding to endogenous GAGs entraps these molecules in ECM from which they may be later released. GAGs can alter the conformation, proteolytic susceptibility and biological activity of some of these proteins. The bound growth factor is resistant to degradation by extracellular proteases. Active hormone is released by proteolysis of the heparan sulfate chains. It occurs during the tissue growth and remodeling after infection.
ECM proteins
Most of the large, multidomain ECM proteins contain at least one GAG binding site.
For example fibrous collagens (type I, III, V) and fibronectin bind to heparan sulfate chains which are attached to the integral membrane core proteins of cell surface proteoglycans such as syndecan and fibroglycan. Cell surface proteoglycans are thought to anchor cells to matrix fibers.
Cell – cell adhesion molecules
· For example NCAM (see cadherins) interacts with cell surface heparan sulfate proteoglycans. This interaction is required for its function. NCAM has a distinct heparan binding domain.
· Hyaluronan is bound to the surface receptors (e.g. CD44) of many migrating cells. It is very important during differentiation (for example myoblasts which are undifferentiated muscle cell precursors bear hyaluronan- rich coat that prevents premature cell fusion). Because its loose, hydrated porous structure, the hyaluronan coat keeps cells apart from each other. They are free to move around and proliferate.
When the level of hyaluronan is lower (e.g. because of digesting by hyaluronidase), there is ceesation of cell movement and initiation of cell- cell attachment.
Mucopolysaccharidoses and collagenoses, their biochemical diagnostics
Mucopolysaccharidoses are a group of metabolic disorders caused by the absence or malfunctioning of lysosomal enzymes needed to break down molecules called glycosaminoglycans – long chains of sugar carbohydrates in each of our cells that help build bone, cartilage, tendons, corneas, skin and connective tissue. Glycosaminoglycans (formerly called mucopolysaccharides) are also found in the fluid that lubricates our joints.
People with a mucopolysaccharidosis disease either do not produce enough of one of the 11 enzymes required to break down these sugar chains into simpler molecules, or they produce enzymes that do not work properly. Over time, these glycosaminoglycans collect in the cells, blood and connective tissues. The result is permanent, progressive cellular damage which affects appearance, physical abilities, organ and system functioning, and, in most cases, mental development.
The mucopolysaccharidoses are part of the lysosomal storage disease family, a group of more than 40 genetic disorders that result when a specific organelle in our body’s cells – the lysosome – malfunctions. The lysosome is commonly referred to as the cell’s recycling center because it processes unwanted material into substances that the cell can utilize. Lysosomes break down this unwanted matter via enzymes, highly specialized proteins essential for survival. Lysosomal disorders like mucopolysaccharidosis are triggered when a particular enzyme exists in too small an amount or is missing altogether.
Features
The mucopolysaccharidoses share many clinical features but have varying degrees of severity. These features may not be apparent at birth but progress as storage of glycosaminoglycans affects bone, skeletal structure, connective tissues, and organs. Neurological complications may include damage to neurons (which send and receive signals throughout the body) as well as pain and impaired motor function. This results from compression of nerves or nerve roots in the spinal cord or in the peripheral nervous system, the part of the nervous system that connects the brain and spinal cord to sensory organs such as the eyes and to other organs, muscles, and tissues throughout the body.
Depending on the mucopolysaccharidosis subtype, affected individuals may have normal intellect or have cognitive impairments, may experience developmental delay, or may have severe behavioral problems. Many individuals have hearing loss, either conductive (in which pressure behind the ear drum causes fluid from the lining of the middle ear to build up and eventually congeal), neurosensitive (in which tiny hair cells in the inner ear are damaged), or both. Communicating hydrocephalus — in which the normal reabsorption of cerebrospinal fluid is blocked and causes increased pressure inside the head — is common in some of the mucopolysaccharidoses. Surgically inserting a shunt into the brain can drain fluid. The eye’s cornea often becomes cloudy from intracellular storage, and glaucoma
and degeneration of the retina also may affect the patient’s vision.
Physical symptoms generally include coarse or rough facial features (including a flat nasal bridge, thick lips, and enlarged mouth and tongue), short stature with disproportionately short trunk (dwarfism), dysplasia (abnormal bone size and/or shape) and other skeletal irregularities, thickened skin, enlarged organs such as liver (hepatomegaly) or spleen (splenomegaly), hernias, and excessive body hair growth. Short and often claw-like hands, progressive joint stiffness, and carpal tunnel syndrome can restrict hand mobility and function. Recurring respiratory infections are common, as are obstructive airway disease and obstructive sleep apnea. Many affected individuals also have heart disease, often involving enlarged or diseased heart valves.
Another lysosomal storage disease often confused with the mucopolysaccharidoses is mucolipidosis. In this disorder, excessive amounts of fatty materials known as lipids (another principal component of living cells) are stored, in addition to sugars. Persons with mucolipidosis may share some of the clinical features associated with the mucopolysaccharidoses (certain facial features, bony structure abnormalities, and damage to the brain), and increased amounts of the enzymes needed to break down the lipids are found in the blood.
Types
Seven distinct clinical types and numerous subtypes of the mucopolysaccharidoses have been identified. Although each mucopolysaccharidosis (MPS) differs clinically, most patients generally experience a period of normal development followed by a decline in physical and/or mental function.
Diagnosis
Diagnosis often can be made through clinical examination and urine tests (excess mucopolysaccharides are excreted in the urine). Enzyme assays (testing a variety of cells or body fluids in culture for enzyme deficiency) are also used to provide definitive diagnosis of one of the mucopolysaccharidoses. Prenatal diagnosis using amniocentesis and chorionic villus sampling can verify if a fetus either carries a copy of the defective gene or is affected with the disorder. Genetic counseling can help parents who have a family history of the mucopolysaccharidoses determine if they are carrying the mutated gene that causes the disorders.
connective tissue diseases
: any of various diseases or abnormal states (as rheumatoid arthritis, systemic lupus erythematosus, polyarteritis nodosa, rheumatic fever, and dermatomyositis) characterized by inflammatory or degenerative changes in connective tissue—called also collagen disease, collagenolysis, collagen vascular disease
Tooth is a complex system of specialized tissues
A tooth is a small, calcified, whitish structure found in the jaws (or mouths) of many vertebrates and used to break down food. Some animals, particularly carnivores, also use teeth for hunting or for defensive purposes. The roots of teeth are covered by gums. Teeth are not made of bone, but rather of multiple tissues of varying density and hardness.
Biochemical composition of teeth tissues
|
Compounds |
pulp |
dentin |
enamel |
cementum |
|
|
Water |
g per |
||||
|
30 – 40 |
13 |
2,5 |
3,2 |
||
|
Organic compounds |
40 |
20 |
4 |
25 |
|
|
Inorganic compounds |
20 – 30 |
69 |
96 |
70 |
|
|
Ca |
g per |
||||
|
30 |
35 |
36 |
35,5 |
||
|
Mg |
0,8 |
1,2 |
0,5 |
0,9 |
|
|
Na |
0,2 |
1,2 |
0,2 |
1,1 |
|
|
K |
0,1 |
0,1 |
0,3 |
0,1 |
|
|
P |
17,0 |
17,4 |
17,3 |
17,1 |
|
|
F |
0,02 |
0,02 |
0,02 |
0,02 |
|
|
citrate |
– |
1,0 |
0,3 |
– |
|
|
|
|
|
|
|
|
Оrganic components – proteins, carbohydrates, lipids, nucleic acids, vitamins, enzymes, hormones, organic acids.
Soluble proteins:
Аlbumins, globulins
Enzymes
• Alkaline phosphatase
• Acidic phosphatase
Glycoproteins (fibronectin)
Proteoglycans
Phopsphoproteins
Non soluble proteis:
Collagen
Enamelin, amelogenin (in enamel)
Carbohydrates
n Glycogen
n Glycosaminoglycans (GAG, mucopolysaccharides) are long-chain compounds made up of hundreds repeating disaccharide units. One of the sugars in each disaccharide unit is a hexosamine (glycosamine).
n Many proteoglycans contain a core protein which links them to the cellular membrane.
Hyaluronic acid is an extremely long and rigid glycosaminoglycan
Mineral matrix – apatites
n Composed of mineralized calcium phosphate (specifically, the calcium phosphate phase called hydroxyapatite (HAP) í Ca10(PO4)6(OH)2) within a matrix of collagen fibrils
n The HAP of teeth is not compositionally pure
– it’s composition can actually be better represented as
– (Ca, Sr, Mg, Na, H2O, [])10(PO4, HPO4, CO3P2O7)6(OH, F, Cl, H2O, O, [])2
– where [] represent crystal lattice defects
n HAP is a ‘living mineral’ that is continually grown, dissolved & remodeled in response to signals of internal (e.g., pregnancy) and external (e.g., gravity, exercise) origin
n Ca10(PO4)6(OH)2
n Ca8H2(PO4)6 · 5H2O
n Ca10(PO4)6CO3 or Ca10(PO4)5CO3(OH)2
n Ca10(PO4)6Cl
n SrCa9(PO4)6(OH)2
n Ca10(PO4)6F2
Hydroxylapatite, also called hydroxyapatite (HA), is a naturally occurring mineral form of calcium apatite with the formula Ca5(PO4)3(OH), but is usually written Ca10(PO4)6(OH)2 to denote that the crystal unit cell comprises two entities. Hydroxylapatite is the hydroxyl endmember of the complex apatite group. The OH– ion can be replaced by fluoride, chloride or carbonate, producing fluorapatite or chlorapatite. It crystallizes in the hexagonal crystal system. Pure hydroxylapatite powder is white. Naturally occurring apatites can, however, also have brown, yellow, or green colorations, comparable to the discolorations of dental fluorosis.
Up to 50% of bone by weight is a modified form of hydroxylapatite (known as bone mineral). Carbonated calcium-deficient hydroxylapatite is the main mineral of which dental enamel and dentin are composed.
Enamel
· Enamel—the whitish covering—is the hardest and most mineralized part of the teeth and of the entire body. About 96 percent of enamel consists of a mineral called hydroxylapatite, a form of which also makes up to 50 percent of bone. The other 4 percent is water and organic material. Because of its high concentration of mineral power, enamel is strong enough to withstand the stress of biting, chewing and grinding. However, that same trait makes enamel brittle and susceptible to cracking and chipping.
Tooth enamel is the most mineralized tissue of human body. Its composition is 96 wt.% inorganic material and 4 wt.% organic material and water. In dentin, the inorganic material represents 70 wt.%. This inorganic material is mainly composed by a calcium phosphate related to the hexagonal hydroxyapatite, whose chemical formula is Ca10(PO4)6·2(OH) 1. X-ray energy dispersive spectroscopy (EDS) analysis of enamel and dentin also indicated the presence in small quantities of other elements such as Na, Cl and Mg 2.
Human teeth are exposed to a different point-to-point pressure during mastication. Therefore, the study and analysis of their hardness is very important for understanding how masticatory strains are distributed throughout the tooth, and for predicting how stresses and strains are altered by dental restorative procedures, age and disease. Moreover, the hardness values can be related to other mechanical properties, such as Young’s modulus and yield stress. Measurement of hardness in tooth is not easy, however. Because the structures that enamel2 and dentin present, prisms running from the enamel-dentin junction (EDJ) to the surface in the case of enamel and a heterogeneous composite material in the case of dentin, it is easy to imagine that their hardness values are different, even from one site to other inside enamel and dentin themselves; and that they would be chemically dependent.
Hardness testing, together with intra-oral models, has great importance in de- and re-mineralization experiments. The hardness of human tooth has been determined by a variety of methods, including abrasion, scratch, and indentation techniques. Since considerable local variations have been reported in enamel and dentin, the methods using a micro-scratch or micro-indentation have been preferred, and the Knoop diamond indenter is commonly used. Recently, nano-indentation using atomic force microscopy was reported in hardness measurements of dentin3.
Knoop (KHN) and Vicker (VHN) hardnesses have reported approximately the same value15. The average hardness value for enamel and dentin is in the range from 270 to 350 KHN (or from 250 to 360 VHN) and from 50 to 70 KHN respectively4. However, the standard deviations (SD) for these values show broad and significative variations, although in dentin these variations are less pronounced. Thus, for example, Craig and Peyton reported for enamel a hardness in the range from 344 ± 49 to 418 ± 60 VHN; Collys et al. from 369 ± 25 to 431 ± 35;
In sound human enamel, it was reported that the hardness values, the mineral content, and the density gradually decrease from the outer surface to the EDJ. More specific, Kodaka et al. found a moderate correlation between the Vicker hardness and P concentration in enamel, but a low correlation with Ca. They indicated that VHN values, Ca and P percentage significantly decreased in the outer, middle and inner enamel sites. Other studies reported that the outer enamel surface is harder than the inner surface, and that hardness continuously decreases from the outer edge to EDJ. Gustafson and Kling proposed that the differences of hardness in enamel can be produced by variations in the direction of indentations in a single tooth section. However, some other studies13 have found any difference at all, only slight indications that enamel is harder in the cusp and outer surface than in the cervical margin or EDJ, but the difference was less than the SD reported, and thus no definite statement can be made.
Hardness numbers reported for dentin also varies. Because of the larger size of the indentation in relation to the dentin microstructure, this variation may be due to the differences in the dentinal tubule density at different locations. Kenney et al., using a modified atomic-force microscope to measure the hardness of dentin, indicated that hydrated peritubular dentin has a hardness inside the range from 2.2 to 2.5 GPa independent of location, while in intertubular dentin this hardness did depend upon location, and it was significantly greater near the EDJ (values from 0.49 to 0.52 GPa) thaear the pulp (from 0.12 to 0.18 GPa).
Another parameter that must be taken into account in is time. It was reported that in human tooth the hardness indentations restored after time. However, in general, little is known about the way the size of these indentations changes with time. Since enamel is a rather brittle material, time dependency of an indentation seems to be very small or negligible. But, in dentin, Herkstroter et al. found that indentations relaxed (becomes smaller) over a period of one day; after that the indentations do not change statistically anymore. Some explanation for indentation relaxation could be the differences in the content of organic matrix and/or in the bonding between mineral and organic matrix.
As it can be seen, too many parameters are involved in the analysis of human tooth hardness; therefore, in this work we obtain accurate Vickers hardness values (with minimum SD) for enamel and dentin in sound teeth. We took care of the sample preparation method, the chemical composition all along the tooth, and the relative orientation of the indenter with the enamel prisms and dentin tubules to identify and control the parameters that statistically affect the hardness measurement. Vickers hardness indentations were measured and analyzed with light microscopy (LM) and scanning electron microscopy (SEM).
Tooth enamel, along with dentin, cementum, and dental pulp is one of the four major tissues that make up the tooth in lobe finned fish and tetrapods. It is the hardest and most highly mineralized substance in the human body. Tooth enamel is also found in the dermal denticles of sharks. It is the normally visible dental tissue of a tooth. It covers the anatomical crown and must be supported by underlying dentin. Ninety-six percent of enamel consists of mineral, with water and organic material composing the rest. In humans, enamel varies in thickness over the surface of the tooth, often thickest at the cusp, up to 2.5 mm, and thinnest at its border with the cementum at the cementoenamel junction (CEJ).
The normal color of enamel varies from light yellow to grayish(bluish) white. At the edges of teeth where there is no dentin underlying the enamel, the color sometimes has a slightly blue tone. Since enamel is semitranslucent, the color of dentin and any material underneath the enamel strongly affects the appearance of a tooth. The enamel on primary teeth has a more opaque crystalline form and thus appears whiter than on permanent teeth.
Enamel’s primary mineral is hydroxyapatite, which is a crystalline calcium phosphate. The large amount of mineral in enamel accounts not only for its strength but also for its brittleness. Tooth enamel ranks 5 on Mohs hardness scale and a Young’s modulus of 83 GPa. Dentin, less mineralized and less brittle, 3–4 in hardness, compensates for enamel and is necessary as a support.[6] On radiographs, the differences in the mineralization of different portions of the tooth and surrounding periodontium can be noted; enamel appears more radiopaque (or lighter) than either dentin and pulp since it is denser than both, both of which appear more radiolucent (or darker).
Enamel does not contain collagen, as found in other hard tissues such as dentin and bone, but it does contain two unique classes of proteins – amelogenins and enamelins. While the role of these proteins is not fully understood, it is believed that they aid in the development of enamel by serving as a framework for minerals to form on, among other functions. Once it is mature, enamel is almost totally absent of the softer organic matter. Enamel is avascular and has no nerve supply within it and is not renewed, however, it is not a static tissue as it can undergo mineralization changes.[9]
The basic unit of enamel is called an enamel rod. Measuring 4–8 μm in diameter, an enamel rod, formally called an enamel prism, is a tightly packed mass of hydroxyapatite crystals in an organized pattern.[1] In cross section, it is best compared to a keyhole, with the top, or head, oriented toward the crown of the tooth, and the bottom, or tail, oriented toward the root of the tooth.
The arrangement of the crystals within each enamel rod is highly complex. Both ameloblasts (the cells which initiate enamel formation) and Tomes’ processes affect the crystals’ pattern. Enamel crystals in the head of the enamel rod are oriented parallel to the long axis of the rod. When found in the tail of the enamel rod, the crystals’ orientation diverges slightly(65 degrees) from the long axis.
The arrangement of enamel rods is understood more clearly than their internal structure. Enamel rods are found in rows along the tooth, and within each row, the long axis of the enamel rod is generally perpendicular to the underlying dentin.[10] In permanent teeth, the enamel rods near the cementoenamel junction (CEJ) tilt slightly toward the root of the tooth. Understanding enamel orientation is very important in restorative dentistry, because enamel unsupported by underlying dentin is prone to fracture.[10]

The area around the enamel rod is known as interrod enamel. Interrod enamel has the same composition as enamel rod, however a histologic distinction is made between the two because crystal orientation is different in each.[3] The border where the crystals of enamel rods and crystals of interrod enamel meet is called the rod sheath.
Striae of Retzius are incremental lines that appear brown in a stained section of mature enamel. These lines are composed of bands or cross striations on the enamel rods that, when combined in longitudinal sections, seem to traverse the enamel rods.[10] Formed from changes in diameter of Tomes’ processes, these incremental lines demonstrate the growth of enamel, similar to the annual rings on a tree on transverse sections of enamel. The exact mechanism that produces these lines is still being debated. Some researchers hypothesize that the lines are a result of the diurnal, or 24 hour, metabolic rhythm of the ameloblasts producing the enamel matrix, which consists of an active secretory work period followed by an inactive rest period during tooth development. Thus, each band on the enamel rod demonstrates the work/rest pattern of the ameloblasts that generally occurs over a span of a week. Perikymata which are associated with the Striae are shallow grooves noted clinically on the nonmasticatory surfaces of some teeth in the oral cavity.[13] Perikymata are usually lost through tooth wear, except on the protected cervical regions of some teeth, especially the permanent maxillary central incisors, canines, and first premolars, and may be confused as dental calculus.[12] Darker than the other incremental lines, the neonatal line is a incremental line that separates enamel formed before and after birth. The neonatal line marks the stress or trauma experienced by the ameloblasts during birth, again illustrating the sensitivity of the ameloblasts as they form enamel matrix. As one would expect, the neonatal line is found in all primary teeth and in the larger cusps of the permanent first molars. They contain irregular structures of enamel prisms with disordered crystal arrangements basically formed by the abrupt bending of the prisms towards the root; usually, the prisms gradually bent back again to regain their previous orientation.
Gnarled enamel is found at the cusps of teeth. Its twisted appearance results from the orientation of enamel rods and the rows in which they lie.
Enamel is covered by various structures in relation to the development of tooth:
Nasmyth’s membrane or enamel cuticle, structure of embryological origin is composed of keratin which gives rise to the enamel organ.
Acquired pellicle, structure acquired after tooth eruption is composed of food debris, calculus, dental plaque (organic film).
Development
Enamel initially starts with a high protein content, but these are removed and the voids backfilled with HAP as the tooth matures

Histologic slide showing a developing tooth. The mouth would be in the area of space at the top of the picture.
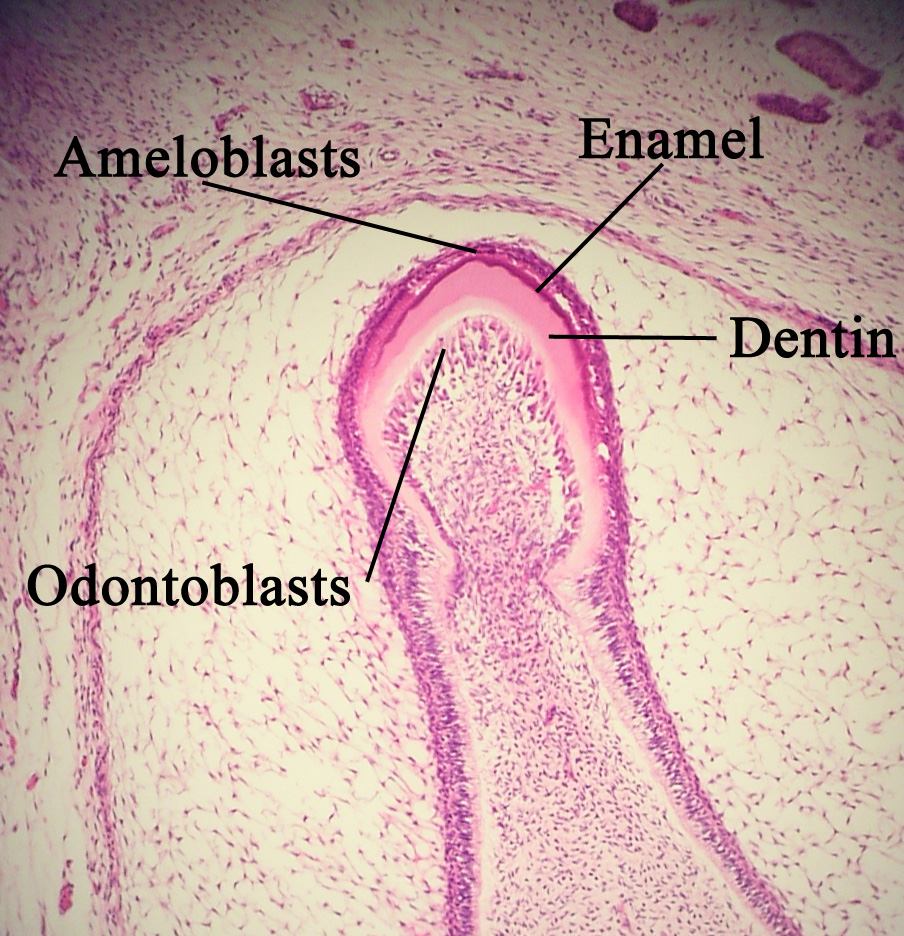
Enamel formation is part of the overall process of tooth development. When the tissues of the developing tooth are seen under a microscope, different cellular aggregations can be identified, including structures known as the enamel organ, dental lamina, and dental papilla.[19] The generally recognized stages of tooth development are the bud stage, cap stage, bell stage, and crown, or calcification, stage. Enamel formation is first seen in the crown stage.
Amelogenesis, or enamel formation, occurs after the first establishment of dentin, via cells known as ameloblasts. Human enamel forms at a rate of around 4 μm per day, beginning at the future location of cusps, around the third or fourth month of pregnancy.[10] As in all human processes, the creation of enamel is complex, but can generally be divided into two stages.[20] The first stage, called the secretory stage, involves proteins and an organic matrix forming a partially mineralized enamel. The second stage, called the maturation stage, completes enamel mineralization.
In the secretory stage, ameloblasts are polarized columnar cells. In the rough endoplasmic reticulum of these cells, enamel proteins are released into the surrounding area and contribute to what is known as the enamel matrix, which is then partially mineralized by the enzyme alkaline phosphatase.[21] When this first layer is formed, the ameloblasts move away from the dentin, allowing for the development of Tomes’ processes at the apical pole of the cell. Enamel formation continues around the adjoining ameloblasts, resulting in a walled area, or pit, that houses a Tomes’ process, and also around the end of each Tomes’ process, resulting in a deposition of enamel matrix inside of each pit. The matrix within the pit will eventually become an enamel rod, and the walls will eventually become interrod enamel. The only distinguishing factor between the two is the orientation of the calcium phosphate crystals. In the maturation stage, the ameloblasts transport substances used in the formation of enamel. Histologically, the most notable aspect of this phase is that these cells become striated, or have a ruffled border. These signs demonstrate that the ameloblasts have changed their function from production, as in the secretory stage, to transportation. Proteins used for the final mineralization process compose most of the transported material. The noteworthy proteins involved are amelogenins, ameloblastins, enamelins, and tuftelins. During this process, amelogenins and ameloblastins are removed after use, leaving enamelins and tuftelin in the enamel.[23] By the end of this stage, the enamel has completed its mineralization.
At some point before the tooth erupts into the mouth, but after the maturation stage, the ameloblasts are broken down. Consequently, enamel, unlike many other tissues of the body, has no way to regenerate itself. After destruction of enamel from decay or injury, neither the body nor a dentist can restore the enamel tissue. Enamel can be affected further by non-pathologic processes.
The discoloration of teeth over time can result from exposure to substances such as tobacco, coffee, and tea. The staining occurs in the interprismatic region internally on the enamel, which causes the tooth to appear darker or more yellow overall. In a perfect state, enamel is colorless, but it does reflect underlying tooth structure with its stains since light reflection properties of the tooth are low.
Stages of amelogenesis
n Secretion and primary mineralization
Enamel is soft and contains many org. substances
n Maturation (secondary mineralization)
Further calcification
n Final maturation (tertiary mineralization)
After teeth eruption
Destruction
The high mineral content of enamel, which makes this tissue the hardest in the human body, also makes it susceptible to a demineralization process which often occurs as dental caries, otherwise known as cavities. Demineralization occurs for several reasons, but the most important cause of tooth decay is the ingestion of fermentable carbohydrates. Tooth cavities are caused when acids dissolve tooth enamel:
Ca10(PO4)6(OH)2(s) + 8H+(aq) → 10Ca2+(aq) + 6HPO42-(aq) + 2H2O(l)
Sugars from candies, soft drinks, and even fruit juices play a significant role in tooth decay, and consequently in enamel destruction. The mouth contains a great number and variety of bacteria, and when sucrose, the most common of sugars, coats the surface of the mouth, some intraoral bacteria interact with it and form lactic acid, which decreases the pH in the mouth. Then, the hydroxylapatite crystals of enamel demineralize, allowing for greater bacterial invasion deeper into the tooth.
The most important bacterium involved with tooth decay is Streptococcus mutans, but the number and type of bacteria varies with the progress of tooth destruction.
Furthermore, tooth morphology dictates that the most common site for the initiation of dental caries is in the deep grooves, pits, and fissures of enamel. This is expected because these locations are impossible to reach with a toothbrush and allow for bacteria to reside there. When demineralization of enamel occurs, a dentist can use a sharp instrument, such as a dental explorer, and “feel a stick” at the location of the decay. As enamel continues to become less mineralized and is unable to prevent the encroachment of bacteria, the underlying dentin becomes affected as well. When dentin, which normally supports enamel, is destroyed by a physiologic condition or by decay, enamel is unable to compensate for its brittleness and breaks away from the tooth easily.
The extent to which tooth decay is likely, known as cariogenicity, depends on factors such as how long the sugar remains in the mouth. Contrary to common belief, it is not the amount of sugar ingested but the frequency of sugar ingestion that is the most important factor in the causation of tooth decay.[29] When the pH in the mouth initially decreases from the ingestion of sugars, the enamel is demineralized and left vulnerable for about 30 minutes. Eating a greater quantity of sugar in one sitting does not increase the time of demineralization. Similarly, eating a lesser quantity of sugar in one sitting does not decrease the time of demineralization. Thus, eating a great quantity of sugar at one time in the day is less detrimental than is a very small quantity ingested in many intervals throughout the day. For example, in terms of oral health, it is better to eat a single dessert at dinner time than to snack on a bag of candy throughout the day.
In addition to bacterial invasion, enamel is also susceptible to other destructive forces. Bruxism, also known as clenching of or grinding on teeth, destroys enamel very quickly. The wear rate of enamel, called attrition, is 8 micrometers a year from normal factors. A common misconception is that enamel wears away mostly from chewing, but actually teeth rarely touch during chewing. Furthermore, normal tooth contact is compensated physiologically by the periodontal ligaments (pdl) and the arrangement of dental occlusion. The truly destructive forces are the parafunctional movements, as found in bruxism, which can cause irreversible damage to the enamel.
Other nonbacterial processes of enamel destruction include abrasion (involving foreign elements, such as toothbrushes), erosion (involving chemical processes, such as dissolving by soft drinks or lemon and other juices), and possibly abfraction (involving compressive and tensile forces).
Though enamel is described as tough, it has a similar brittleness to glass making it, unlike other natural crack-resistant laminate structures such as shell and nacre, potentially vulnerable to fracture. In spite of this it can withstand bite forces as high as 1,000 N many times a day during chewing. This resistance is due in part to the microstructure of enamel which contains processes, enamel tufts, that stabilize the growth of such fractures at the dentinoenamel junction. The configuration of the tooth also acts to reduce the tensile stresses that cause fractures during biting.
Oral hygiene and fluoride
Considering the vulnerability of enamel to demineralization and the daily menace of sugar ingestion, prevention of tooth decay is the best way to maintain the health of teeth. Most countries have wide use of toothbrushes, which can reduce the number of bacteria and food particles on enamel. Some isolated societies do not have access to toothbrushes, but it is common for those people to use other objects, such as sticks, to clean their teeth. In between two adjacent teeth, floss is used to wipe the enamel surfaces free of plaque and food particles to discourage bacterial growth. Although neither floss nor toothbrushes can penetrate the deep grooves and pits of enamel, good general oral health habits can usually prevent enough bacterial growth to keep tooth decay from starting.
These methods of oral hygiene have been helped greatly by the use of fluoride. Fluoride can be found in many locations naturally, such as the ocean and other water sources. The recommended dosage of fluoride in drinking water depends on air temperature; in the
Many groups of people have spoken out against fluoridated drinking water, for reasons such as the neurotoxicity of fluoride or the damage fluoride can do as fluorosis. Fluorosis is a condition resulting from the overexposure to fluoride, especially between the ages of 6 months to 5 years, and appears as mottled enamel.[37] Consequently the teeth look unsightly, although the incidence of dental decay in those teeth is very small. It is important, however, to note that all substances, even beneficial ones, are detrimental when taken in extreme doses. Where fluoride is found naturally in high concentrations, filters are often used to decrease the amount of fluoride in water. For this reason, codes have been developed by dental professionals to limit the amount of fluoride a person should take. These codes are supported by the American Dental Association and the
Systemic conditions affecting enamel
There are different types of amelogenesis imperfecta. The hypocalcification type, which is the most common, is an autosomal dominant condition that results in enamel that is not completely mineralized. Consequently, enamel easily flakes off the teeth, which appear yellow because of the revealed dentin. The hypoplastic type is X-linked and results iormal enamel that appears in too little quantity, having the same effect as the most common type.
Gastroesophageal reflux disease can also lead to enamel loss, as acid refluxes up the esophagus and into the mouth, occurring most during overnight sleep.
Chronic bilirubin encephalopathy, which can result from erythroblastosis fetalis, is a disease which has numerous effects on an infant, but it can also cause enamel hypoplasia and green staining of enamel.
Enamel hypoplasia is broadly defined to encompass all deviations from normal enamel in its various degrees of absence. The missing enamel could be localized, forming a small pit, or it could be completely absent.
Erythropoietic porphyria is a genetic disease resulting in the deposition of porphyrins throughout the body. These deposits also occur in enamel and leave an appearance described as red in color and fluorescent.
Fluorosis leads to mottled enamel and occurs from overexposure to fluoride.
Dental fluorosis, also called mottling of tooth enamel, is a developmental disturbance of dental enamel caused by excessive exposure to high concentrations of fluoride during tooth development. The risk of fluoride overexposure occurs between the ages of 3 months and 8 years. In its mild forms (which are its most common), fluorosis often appears as unnoticeable, tiny white streaks or specks in the enamel of the tooth. In its most severe form, tooth appearance is marred by discoloration or brown markings. The enamel may be pitted, rough and hard to clean. The spots and stains left by fluorosis are permanent and may darken over time.
A mild case of dental fluorosis (the white streaks on the subject’s upper right central incisor) observed in dental practice
Risk factors for dental fluorosis
The greatest concern in dental fluorosis is aesthetic changes in the permanent dentition (the adult teeth). These changes are prone to occur in children who are excessively exposed to fluoride between 20 and 30 months of age. The critical period of exposure is between 1 and 4 years old, and the child is no longer at risk after 8 years of age. The severity of dental fluorosis depends on the amount of fluoride exposure, the age of the child, individual response, weight, degree of physical activity, nutrition, and bone growth.
Many well-known sources of fluoride may contribute to overexposure including dentifrice/fluoridated mouthrinse (which young children may swallow), bottled waters which are not tested for their fluoride content, inappropriate use of fluoride supplements, ingestion of foods especially imported from other countries, and public water fluoridation. The last of these sources is directly or indirectly responsible for 40% of all fluorosis, but the resulting effect due to water fluoridation is largely and typically aesthetic. Severe cases can be caused by exposure to water that is naturally fluoridated to levels well above the recommended levels, or by exposure to other fluoride sources such as brick tea or pollution from high fluoride coal.
Tetracycline staining leads to brown bands on the areas of developing enamel. Children up to age 8 can develop mottled enamel from taking tetracycline. As a result, tetracycline is contraindicated in pregnant women.
Celiac disease, a disorder characterized by an auto-immune response to gluten, also commonly results in demineralization of the enamel.
Dentin
n The formation of dentin – dentinogenesis. The porous, yellow-hued material is made up of
n 70% inorganic materials,
n 20% organic materials,
n 10% water.
Primary dentin – during formation and teething
Secondary dentin – formed after the eruption and is a continuation of the primary
Tertiary dentin (reparative) formed in response to pathogenic factors
Dentin is the substance between enamel or cementum and the pulp chamber. It is secreted by the odontoblasts of the dental pulp. The formation of dentin is known as dentinogenesis. The porous, yellow-hued material is made up of 70% inorganic materials, 20% organic materials, and 10% water by weight.[14] Because it is softer than enamel, it decays more rapidly and is subject to severe cavities if not properly treated, but dentin still acts as a protective layer and supports the crown of the tooth.
Dentin is a mineralized connective tissue with an organic matrix of collagenous proteins. Dentin has microscopic channels, called dentinal tubules, which radiate outward through the dentin from the pulp cavity to the exterior cementum or enamel border.[15] The diameter of these tubules range from 2.5 μm near the pulp, to 1.2 μm in the midportion, and 900 nm near the dentino-enamel junction. Although they may have tiny side-branches, the tubules do not intersect with each other. Their length is dictated by the radius of the tooth. The three dimensional configuration of the dentinal tubules is genetically determined.
Cementum
Cementum is excreted by cementoblasts within the root of the tooth and is thickest at the root apex.
· Non cellular – primary (thin layer)
· Cellular – secondary (on the apex and bifurcation areas)
Cementum is a specialized bony substance covering the root of a tooth. It is approximately 45% inorganic material (mainly hydroxyapatite), 33% organic material (mainly collagen) and 22% water. Cementum is excreted by cementoblasts within the root of the tooth and is thickest at the root apex. Its coloration is yellowish and it is softer than either dentin or enamel. The principal role of cementum is to serve as a medium by which the periodontal ligaments can attach to the tooth for stability. At the cementoenamel junction, the cementum is acellular due to its lack of cellular components, and this acellular type covers at least ⅔ of the root. The more permeable form of cementum, cellular cementum, covers about ⅓ of the root apex.
Pulp
The dental pulp is the part in the center of a tooth made up of living soft tissue and cells called odontoblasts. Those include: Fibroblasts, Granulocites, Histiosites etc. It’s commonly called ‘the nerve’, although it contains many other structures which are not nerves.
The dental pulp is the central part of the tooth filled with soft connective tissue.[14] This tissue contains blood vessels and nerves that enter the tooth from a hole at the apex of the root. Along the border between the dentin and the pulp are odontoblasts, which initiate the formation of dentin. Other cells in the pulp include fibroblasts, preodontoblasts, macrophages and T lymphocytes. The pulp is commonly called “the nerve” of the tooth.
Functions:
· Plastic
· Trophy
· Sensor
GUMS, the tough pink-colored skin that covers the bone of the jaw and supports the tooth along with the alveolar bone.
Remineralization
· Researchers believe that fluoride—a version of the element found in toothpaste—is a prominent factor in tooth remineralization. Once fluoride gets onto the surface of the tooth, it attracts other minerals. Thus such exposure reduces tooth decay.
ph of oral liquid 6,4 – 7,8 assists in mineralization
Са2+/ Р for mineralization in saliva is 1,67
Mg2+, Mn2+, Zn2+, Cu2+, Si2+ increase mineralization
ph<6,2 leads to the demineralization
Teeth demineralisation:
Са10 (РО4)6(ОН)2 + 2Н+ → Са9Н2 (РО4)6(ОН)2 + Са2+
Conversion of GAP into ftorapatite:
Са10 (РО4)6(ОН)2 + 2F– → Са10 (РО4)6F2 + 2(ОН)-
Excess of F– couses demineralisation
Са10 (РО4)6(ОН)2 + 20F- → 10CаF2 + 6РО4 3- + 2(ОН)-
Scurvy – dietary deficiency in vitamin C, leading to abnormal collagen.
Symptoms: (hemorrhages, loose of teeth, gums swell and bleed easily)
Scurvy is possibly the oldest knowutritional disease, having been described in medical writings as early as 400 B.C. It is a deficiency disorder that is caused by a lack of vitamin C, or ascorbic acid, in the diet. It is also called vitamin C deficiency or scorbutus. Vitamin C is a very important anti-oxidant that is required for the production of collagen, which is necessary for healthy development of tissues, for the functioning of the immune system, and for the healing of wounds. It is found in certain fruits and vegetables, especially citrus fruits, and green leafy vegetables such as spinach and broccoli. It was once common in sailors and soldiers, who were away from sources of fresh fruits and vegetables for long periods of time; though it was known that scurvy was nutrition-related, it wasn’t until the 20th century that the exact cause of it was identified. In contemporary times, scurvy is rare in countries where fresh fruits and vegetables are easily accessible, and where vitamin C is added to some foods.
SCURVY SYMPTOMS
Symptoms of scurvy usually begin to appear about one to three months after the intake of vitamin C has stopped. Scurvy is characterized by tiredness, weakness in the muscles, fainting, aches in the joints and muscles, a rash on the legs, hair growing in a spiral pattern, anemia, and bleeding gums. In children, it presents as painful swelling of the legs, as well as fever, diarrhea, and vomiting. Adult symptoms include malaise, as well the appearance of spots that can appear as tiny red blood blisters to large purplish blotches on the skin of the legs. Gums may swell and bleed easily, turn blue and bruised, and eventually the teeth are loosened. Other symptoms can include irritability, pain in the legs, paralysis, swelling, lung and kidneyproblems, and hemorrhaging. If the progress of scurvy is not halted, it will result in death.
SCURVY CAUSES
Scurvy is primarily caused by a lack of vitamin C in the diet. In babies, scurvy can develop if they are weaned from breast milk to cow’s milk and are not given a vitamin C supplement. It can also occur in babies whose mothers took high doses of vitamin C during pregnancy. Stress, either emotional or physiological, also contributes to scurvy.
SCURVY DIAGNOSIS
Scurvy is usually diagnosed visually, by evaluating the symptoms present. A dietary history may be taken, in which you tell your doctor about your diet, so that a vitamin C deficiency can be discerned. In some cases, a blood test can be given to test the level of ascorbic acid in the blood. Sometimes a dermatologist must be consulted to evaluate the different spots on the skin that can be caused by scurvy or may be a symptom of something else, and an internal medicine specialist can evaluate other symptoms that may affect the internal organs.
Biochemistry of saliva: sourses, functions, chemical
composition, regulation and pathology of saliva secretion.
Salivary glands are nonexcitable effector organs in which a large amount of fluid and electrolytes is transferred from the interior of the body to the outside. The amount of fluid translocated each day through salivary glands approaches 750 ml, which represents approximately 20% of total plasma volume.
Saliva is a complex fluid secreted by salivary glands containing water, mucin, proteins, salts and enzymes.
Functions:
– digestion
– lubricates both hard and soft tissues
– buffers cariogenic acids
– forms the pellicle
– provides minerals for repairing enamel / cementum (remineralization)
– delivers antimicrobial agents (immunoglobulins, enzymes, etc.)
– excretory
– regulatory
Saliva neutralises the acids which cause the pH of the tooth surface to rise above the critical pH. This causes ‘remineralisation’, the return of the dissolved minerals to the enamel.
In the presence of plaque, saliva is unable to penetrate through the plaque to neutralize the acid produced by the bacteria.
Saliva is secreted to the mouth by three major paired salivary glands (submaxillary, parotid, and sublingual glands) and by numerous minor mucous glands, at a rate of approximately 0.025 ml.min-1. The relative contributions of each of these glands to the total amount of saliva secreted average 65 per cent from the submandibular, 23 per cent from the parotid, 8 per cent from the minor mucous, and 4 per cent from the sublingual.
There are three pairs of salivary glands:
· The two largest are the parotid glands, one in each cheek in front of the ears
· Two glands are under the floor of the mouth (sublingual glands)
· Two glands are at the back of the mouth on both sides of the jaw (submandibular glands)
All of the salivary glands empty saliva into the mouth through ducts that open at various locations in the mouth.
Both of the two major parenchymal sites of the salivary glands, the acini and the striated ducti, participate in salivary secretion. Transport of water and electrolytes, and synthesis of enzymes, proteins, mucin and other organic components, occur in the acini, which secrete a fluid isotonic with plasma. This fluid is then modified in the ductus system, by both reabsorption and secretion of electrolytes.
The majority of oral secretions are contributed by the sub-mandibular and parotid glands, which equally provide 80 to 90 per cent of the saliva. The remainder is formed by sublingual and minor salivary glands. One thousand to 1500 ml of saliva is produced daily. Saliva contributes to the digestion of food and to the maintenance of oral hygiene. Without normal salivary function the frequency of dental caries , gum disease (gingivitis), and other oral problems increases significantly.
These glands may contain mucous secreting cells, serous cells or a mixture of both.
Serous cells produce a watery saliva that contains the enzymes amylase and lysozyme, IgA (immunoglobulin A), and lactoferrin (an iron binding compound).
Saliva has important functions :
· Cleanses the mouth due to the bactericidal action of lysozyme and IgA (immunoglobulin A [one of the immune system’s antibodies] )plus the constant backward flow towards the oesophagus
· Creates a feeling of oral comfort by it’s lubricating action
· Dissolve food chemicals so that they can stimulate the tongue’s taste buds
· Help to form a bolus (ball of food) by the action of mucins thus facilitating swallowing
· Contain a digestive enzyme called salivary amylase (ptyalin) which starts the process of breaking down complex starchy sugars
Salivary alpha-amylase
Amylase is an enzyme found in human saliva which is responsible for the breaking down of starch into sugar. The process of digestion begins with the chewing of food, in the presence of salivary amylase in the mouth, to convert the starch in food to sugar. Foods that are high in starch, like potatoes or bread, will taste slightly sweet when chewed – this is because of the action of amylase. The enzyme amylase is also secreted by the pancreas, where it is called pancreatic amylase; its presence in the gastrointestinal tract aids in the breakdown of food molecules into energy for the body to store and use. The diagram of the digestive system will clarify the sequence of digestion and also help in the identification of the organs of the digestive system.
Functions
To digest food, complex substances like carbohydrates and proteins need to be broken down and converted into energy. Different enzymes in the body, secreted by different organs, work on the various types of food, and each is responsible for its own food group. For instance, just as salivary amylase works on starch, pepsin is a digestive enzyme which breaks down protein, similarly, lipase aids in the digestion of fat. In this way, each enzyme has a certain composition, structured towards its function. Salivary amylase pH in the mouth is slightly acidic, at 6.8, within which the enzyme amylase is able to function. Amylase present in the stomach is deactivated due to the presence of hydrochloric acid, which creates an acidic environment in which amylase is denatured. Salivary amylase digests food, and is mainly responsible for the breakdown of complex carbohydrates into maltose. This is done by breaking bonds between the carbohydrate molecules to produce disaccharides and trisaccharides. Salivary amylase is activated by the chewing motion. A substrate is the basis or substance on which an enzyme works. In the case of salivary amylase, the substrate is starch, which it reduces to short polysaccharide chains and maltose.
Abnormal Amylase Levels
In certain cases, levels of amylase may be elevated or reduced, inducing symptoms that require pathological investigation. Generally abnormal levels of amylase will be linked to pancreas problems. Some of the situations that may cause abnormal amylase levels in blood are as follows:
· Pancreatitis is caused by inflammation of the pancreas where there are elevated amylase levels in blood. It may be acute or chronic.
· Chronic pancreatitis is often associated with alcoholism, though it can also be caused by trauma to the pancreas.
· Pancreatic cancer can also lead to an increase in amylase levels, as can gallbladder attacks and any blockages in the pancreatic duct.
· Cystic fibrosis is another cause of elevated amylase levels that may be seen with pancreatic disorders.
Uses
Apart from its function as a digestive enzyme, amylase is also useful elsewhere, other than the human body. In bread making, amylase is useful in breaking down starch in flour into simpler forms of sugar, which yeast can then feed on, causing the bread to rise, and also imparting flavor. Another form of the enzyme, bacillary amylase is used in detergents to dissolve starch from stains, and dishes when used in dishwasher detergents. Salivary amylase functions as the first main step of the process of digestion. It is an important component that acts as a catalyst for the hydrolysis of starch into simpler digestible parts. I hope this article has helped you gain a little understanding about the importance of this enzyme and its functions in the human body.
– BACKGROUND AND PURPOSE
a-Amylase (a-1,4-glucan 4-glucanohydrolase, EC 3.2.1.1) is an enzyme that degrades starch, first to oligosaccharides and then in turn to maltose and glucose, by hydrolyzing a -1,4-glucan bonds. In digestion, the role of a -amylase is primarily the first reaction of this process, generating oligosaccharides that are then hydrolyzed by other enzymes.
In vitro, a-amylase is also able to hydrolyze the a-1,4 linkages in glycogen, but has no activity on the a-1,6 linkages responsible for the more highly branched structure of glycogen. These branched structures also reduce the activity of a-amylase toward glycogen by limiting the accessibility of the target a -1,4-glucan bonds
.
The enzyme is found in saliva and pancreatic secretions, where it serves an obvious role in polysaccharide digestion. More surprisingly, a-amylase is also found in blood, sweat and tears, possibly for anti-bacterial activity (2). a -Amylase determination has been recognized as an important diagnostic tool for many years (4, 6, 7), because elevated levels of the enzyme are associated with liver and pancreatic disorders, as well as other diseases.
Enzyme Purification
In the early ’60s, purifying salivary a-amylase required a starting volume of 1 –
The data shown in Table I demonstrate the efficiency of the method for purification of a-amylases from various sources.
|
Table 1: Specific Activity of Amylase During Purification |
||||
|
|
Spec. Activity |
Spec. Activitya |
Spec. Activitya of pure enzyme b |
Yield of enzyme (%) from glycogen ppt. |
|
Pancreatin |
45 |
1200 |
1260 |
95% |
|
Human Saliva |
500 |
2400 |
1960 |
75% |
|
Parotid gland |
800 |
2700 |
2500 |
95% |
aSpecific activity is expressed in Somogyi Units/mg protein.
“Somogyi Units” are defined below. bValues obtained from the literature
Enzyme activity assay
The procedure described is essentially that of Somogyi (5), who first quantified amylase activity by measuring the time required to hydrolyze starch, in a carefully standardized substrate solution. A simple assay to measure this time takes advantage of differently colored products generated by the reaction between iodine and the saccharides depending of their degree of degradation:
|
|
-Amylase |
|
-Amylase |
|
|
Starch (polysaccharide) |
→ |
Oligosaccharides |
→––– |
Glucose + Maltose |
|
[Blue with iodine] |
|
[Red with iodine] |
|
[Yellow with iodine] |
|
Maltose |
|
|
|
|
|
Other names |
4-O-α–D-Glucopyranosyl-D-glucose |

After mixing the amylase-containing samples with a standardized starch solution, the reaction is monitored by removing portions of the mixture at timed intervals and adding these to aliquots of an iodine solution. As long as starch is present, a blue-purplish color will develop. As the incubation proceeds, the color will change from blue to blue-purple, to red-purple and then to reddish-brown. If the solution remains yellow, all the starch has been hydrolyzed to glucose and maltose and the assay must be repeated.
The reaction is considered to have reached its endpoint when samples produce a reddish-brown color with iodine.
The time required to reach the endpoint is a function of a-amylase activity expressed in Somogyi units (one Somogyi Unit is defined as the amount of amylase required to produce the equivalent of 1 mg of glucose in free aldehyde groups in 30 minutes at 40° C. (Somogyi Units/dL may be converted to International Units (µmol minute-1 L-1) by multiplying by 1.85.)
[Salivary Amylase] (Somogyi Units/dL) = Temperature Factor
Endpoint time [min]
The temperature factors for the incubation temperatures are:
|
Incubation Temperature (°C) |
Temperature Factor |
|
37 |
18 |
|
40 |
16 |
The best estimate of amylase activity can be made using samples diluted to around 3 – 6 Somogyi Units/dL, so that the assay reaches the endpoint after 3 – 6 minutes.
The submandibular salivary gland secretes a mixed product containing both serous and mucous secretions although the serous component is the larger. They are roughly ovoid in shape and are situated below the mandible (jaw bone) to the left and right. Their ducts open into the floor of the mouth on either side of the tongue’s frenulum.
The parotid salivary glands secrete a serous product only. They are situated on either side of the head in front of the ears. They have long ducts which open into the mouth opposite the second molar tooth on either side.
The sublingual glands produce a mainly mucous product. They are situated just uner the back of the tongue again in a left and right pair. Their ducts open close to those of the submandibular glands.
In addition there are numerous smaller groups of salivary gland tissue scattered diffusely in the submucosa.
The most important are:
· lingual glands in the submucosa and muscle layers of the dorsal surface of the tongue
· minor sulblingual glands close to the larger major sublingual glands (other tongue glands are found on the inferior surface of the tip of tile tongue and on its lateral borders)
· labial glands on the inner surface of the lips
· palatine glands in tile submucosa of the soft and hard palates
· tonsillar glands in the mucosa associated with the palatine and pharyngeal tonsils
· buccal glands in the submucosa lining the cheeks.
· The labial, sublingual, mlnor lingual and buccal glands are composed predominantly of mucous cells, but some serous cells may be present.
· The palatine and lateral lingual glands are entirely mucous secreting
Both the sympathetic and the parasympathetic nervous systems innervate the salivary glands. It is evident that the sympathetic nervous system, although its role in salivation is still controversial, influences the blood flow to the salivary glands and activates myoepithelial cells within the salivary ducts. These myoepithelial cells expedite the flow of saliva by squeezing saliva out of the salivary glands.
Properties of saliva
n Mixed saliva – liquid with density 0,001-0,017
n рН 6,4 до 7,8
n Optimal for mineralization рН of saliva – 7,2-7,8.
n The total concentration of inorganic and organic constituents is generally low when compared to serum.
The pH changes from being slightly acidic (at rest) to basic (pH 8) at ultimate stimulation. This increase in alkalinity is due to the increase of HCO3- in the saliva
Saliva Composition
Saliva is characteristically a colorless dilute fluid, with a density ranging from 18 to 35. Its pH is usually around 6.64, and varies depending on the concentration of CO2 in the blood. When blood CO2 concentration is increased, a higher fraction of CO2 is transferred from the blood to the saliva, and salivary pH decreases. If CO2 is low in blood, on the other hand, salivary pH increases as a result of a low transfer of blood CO2 to salivary glands.
Although a variety of components is always present in saliva, the total concentration of inorganic and organic constituents is generally low when compared to serum. The fraction of saliva represented by water usually exceeds 0.99. Of the inorganic constituents, sodium and potassium (and perhaps calcium) are the cations of major osmotic importance in saliva; the major osmotically active anions are chloride and bicarbonate. Although the percentage of total proteins in saliva is low in comparison to serum, specific proteins, such as the enzyme amylase, are synthesized in the salivary glands and may be present in saliva in concentrations exceeding those of serum. Other organic components existing in saliva include: maltase, serum albumin, urea, uric acid, creatinine, mucine, vitamin C, several amino acids, lysozime, lactate, and some hormones such as testosterone and cortisol. Some gases (CO2, O2, and N2) are also present in saliva. Saliva contains immunoglobins such as Ig A and Ig G, at an average concentration of 9.4 and 0.32 mg%, respectively. The concentration of potassium, calcium, urea, uric acid, and aldosterone are highly correlated to those existing in plasma. This high degree of correlation has not been shown, however, between salivary and plasma concentrations of phosphate. The physiological significance of other constituents of saliva, such as trace minerals, epithelial growth factor, neural growth factor, several enzymes and some proteins (kallikreins, calmodulin) remains unknown.
In animals, saliva is produced in and secreted from the salivary glands. It is a fluid containing
• Electrolytes: (2-21 mmol/L sodium, 10-36 mmol/L potassium, 1.2-2.8 mmol/L calcium, 0.08-0.5 mmol/L magnesium, 5-40 mmol/L cloride, 2-13 mmol/L bicarbonate, 1.4-39 mmol/L phosphate)
• Mucus. Mucus in saliva mainly consists of mucopolysaccharides and glycoproteins;
Salivary mucins
Salivary mucins are well recognized as an important factor in the preservation of the health of the oral cavity. These large glycoproteins play a major role in the formation of protective coatings covering tooth enamel and oral mucosa, which act as a dynamic functional barrier that can modulate the reaction towards detrimental effects of oral environment, hence defending both teeth and oral mucosa.
Structure
· two main molecular weight forms:
o MG1 >1000 kDa;
o MG2 200-300 kDa;
both displaying virtually identical carbohydrate chain make-up, ranging in size from 3 to 16 sugar units.
· Lack precise folded structure of globular proteins
· Asymmetrical molecules with open, randomly organized structure
· Polypeptide backbone (apomucin) with CHO side-chains
· Side chains may end iegatively charged groups, such as sialic acid and bound sulfate
· Hydrophillic, entraining water (resists dehydration)
· Unique rheological properties (e.g., high elasticity, adhesiveness, and low solubility)
Functions
· Lubrication
· Tissue coating
o creates a protective coating about hard and soft tissues
o has a primary role in formation of acquired pellicle
o concentrates anti-microbial molecules at mucosal interface
· Aggregation of bacterial cells
o bacterial adhere to mucins may result in surface attachment, or
o mucin coated bacteria may be unable to attach to the surface
The bacterial aggregating activity of salivary mucins appears to be associated with sulfomucins rather than sialomucins.
interaction with surfactant protein D (Lung and Saliva),anti-influenza and anti-HIV activity
While the removal of sialic acid (pathway) causes only partial loss in mucin aggregating capacity, a complete loss in the bacterial aggregating activity occurs following mucin desulfation. Salivary sulfomucins and sialomucins actively participate in the modulation of the oral mucosal calcium channel activity through the inhibition of EGF-stimulated channel protein tyrosine phosphorylation.
· Bacterial adhesion
o mucin oligosaccharides mimic those on mucosal cell surface
o react with bacterial adhesins blocking them
These functions and the buffer capacity of these mucins may also be involved in the defence against HIV infections in the oral cavity, contrasting trough pH, structure, binding variations the virus’ activity.
Mucus is a “slimy” material that coats many epithelial surfaces and is secreted into fluids such as saliva. It is composed chiefly of mucins and inorganic salts suspended in water.
Mucus adheres to many epithelial surfaces, where it serves as a diffusion barrier against contact with noxious substances (e.g. gastric acid, smoke) and as a lubricant to minimize shear stresses; such mucus coatings are particularly prominent on the epithelia of the respiratory, gastrointestinal and genital tracts. Mucus is also an abundant and important component of saliva, giving it virtually unparalleled lubricating properties (try sticking a piece of apple skin between your molars without saliva).
Mucus-secreting cells are widely distributed through the body. Goblet cells are abundant in the epithelium of the gastrointestinal and respiratory tracts, mucous glands in these same organs deliver their products through ducts into the intestine and respiratory tree, and many of the acinar epithelial cells in salivary glands secrete mucus.
• Antibacterial compounds (thiocyanate, hydrogen peroxide, and secretory immunoglobulin A).
Saliva contained in the mouth has natural disinfectants. Human saliva contains such antibacterial agents as secretory IgA, lactoferrin, and lactoperoxidase.
secretory IgA
n • Various enzymes. The major enzymes found in human saliva are alpha-amylase, lysozyme, and lingual lipase. Amylase starts the digestion of starch before the food is even swallowed. It has pH optima of 6.7-7.4. Human saliva contains also salivary acid phosphatases A+B, N-acetylmuramyl-L-alanine amidase, NAD(P)H dehydrogenase-quinone, salivary lactoperoxidase, superoxide dismutase, glutathione transferase, glucose-6-phosphate isomerase, and tissue protein. Among the protective salivary enzymes – peroxidase and сatalase.There are lactoperoxydase and myeloperoxidase, which are produced in accordance glands or leukocytes. Both enzymes inhibit lipid peroxidation, interrupting free radical reactions, since removed hydroperoxides with chain process. The presence of these things causes saliva to sometimes have a foul odor.
Lysozyme
Lysozyme is an example of a component belonging to an ancient self-defense system.
Enzymes:
Alkaline phosphatase that enhances remineralization processes
acidic phosphatase, which has demineralising action formed salivary glands, microorganisms and leukocytes. They penetrate the tooth enamel and significantly influence the processes of mineralization – demineralization.
Activity of proteolytic enzymes in saliva is low due to the high content of protease inhibitors in saliva.
Minor enzymes include salivary acid phosphatases A+B,
N-acetylmuramyl-L-alanine amidase, NAD(P)H dehydrogenase-quinone,
salivary lactoperoxidase,
glutathione transferase,
aldehyde dehydrogenase,
glucose-6-phosphate isomerase,
tissue kallikrein.
Cells: Possibly as much as 8 million human and 500 million bacterial cells per mL. The presence of bacterial products (small organic acids, amines, and mercaptans) causes saliva to sometimes exhibit foul odor.
n Histatins are polypeptides which possess exceptional anti-fungal and anti-bacterial activities, but are nevertheless present only in saliva.
n Proline-rich proteins (PRPs) are members of a closely related family, of which the acidic PRPs are found solely in saliva.
n Cystatins are closely related proteins which belong to a multigene family.
n Kallikrein and albumin are components of blood plasma. But whereas albumin diffuses into the different mucosal secretions, kallikrein is secreted specifically by the mucosal glands.
Low molecular organic components of saliva:
n Urea – 1.5-2.0 mmol / l
n residual nitrogen – 7,7-14,7 mmol / l
n amino acids – 1,5-2,2 mmol / l
n one order smaller quantities of glucose, lactate, pyruvate, thiocyanate, etc..
n Vitamins B, C, PP, A, D.
Salivary glands secrete a specific hormone – parotyn. It lowers blood Ca2 + and increases its transport into the tissues, thus promotes mineralization of teeth and bone.
With the saliva in the mouth excreted: glucocorticoids, sex, thyroid hormones, and so on. Saliva contains approximately 10-15% of hormones concentration in blood.
Determination of hormones in saliva is an informative indicator of the adrenal gland, gonads and gonadotropic pituitary function.
n In saliva detected compounds with tromboplastyc and antyheparyn activity and natural anticoagulants – plasminogen and its activators.
n In mixed saliva activity of coagulation factors and fibrinolysis greater compared to the salivatory ducts, indicating mutual activating effect of all components of mixed saliva.
Healthy people produce about
Immunoglobulin A
In the oral cavity, indigenous bacteria are often associated with two major oral diseases, caries and periodontal diseases. These diseases seem to appear following an inbalance in the oral resident microbiota, leading to the emergence of potentially pathogenic bacteria. To define the process involved in caries and periodontal diseases, it is necessary to understand the ecology of the oral cavity and to identify the factors responsible for the transition of the oral microbiota from a commensal to a pathogenic relationship with the host. The regulatory forces influencing the oral ecosystem can be divided into three major categories: host related, microbe related, and external factors. Among host factors, secretory immunoglobulin A (SIgA) constitutes the main specific immune defense mechanism in saliva and may play an important role in the homeostasis of the oral microbiota (Secretory IgA (sIgA) consists of two IgA monomers joined by the J-chain and furthermore a secretory component. It is secreted in plasma cells based in the lamina propia of mucosal membranes. Synthesis of sIgA is independent of serum IgA synthesis, therefore lack of serum IgA does not necessarily mean a lack of sIgA. Secretory IgA is the major immunoglobulin in saliva, tears, nasal mucous, colostrum, and breast milk, tracheobronchial and gastrointestinal secretions. It plays a major role in preventing adherence of microorganisms to mucosal sites, both in the activation of the alternative complement pathway and inflammatory reactions). Naturally occurring SIgA antibodies that are reactive against a variety of indigenous bacteria are detectable in saliva. These antibodies may control the oral microbiota by reducing the adherence of bacteria to the oral mucosa and teeth. It is thought that protection against bacterial etiologic agents of caries and periodontal diseases could be conferred by the induction of SIgA antibodies via the stimulation of the mucosal immune system. However, elucidation of the role of the SIgA immune system in controlling the oral indigenous microbiota is a prerequisite for the development of effective vaccines against these diseases. The role of SIgA antibodies in the acquisition and the regulation of the indigenous microbiota is still controversial. Our review discusses the importance of SIgA among the multiple factors that control the oral microbiota. It describes the oral ecosystems, the principal factors that may control the oral microbiota, a basic knowledge of the secretory immune system, the biological functions of SIgA, and, finally, experiments related to the role of SIgA in oral microbial ecology.
Regulation of saliva secretion
Secretion of saliva is usually elicited in response to stimulation of the autonomic innervation to the glands. Although no direct evidence for modification of salivary flow by hormones has been demonstrated in humans, catecholamines might also be involved in the control of saliva electrolytes and protein concentrations. Both salivary output and composition depend on the activity of the autonomic nervous system, and any modification of this activity can be observed indirectly by alterations in the salivary excretion. Although normal salivary secretion is dependent on the cooperation of sympathetic and parasympathetic nerves, the nervous control of saliva secretion is not identical in all salivary glands:
secretion of saliva from sublingual and minor mucous glands is mainly elicited in response to cholinergic stimulation, whereas secretion from the other glands is evoked mainly by adrenergic innervation. In any case, it is generally acknowledged that parasympathetic nerve impulses create the main stimulus for salivary control in general. Parasympathetic stimulation results in a copious flow of saliva low in organic and inorganic compounds concentrations. Sympathetic stimulation, on the other hand, produces a saliva low in volume. In addition, saliva evoked by action of adrenergic mediators is generally higher in organic content and its concentration of certain inorganic salts is also higher than saliva evoked by cholinergic stimulation. The higher organic content of saliva evoked by adrenergic stimulation trough the activity of adenyl-cyclase, includes elevated levels of total protein, especially the digestive enzyme alpha-amilase. High concentrations of alpha-amilase in saliva are indeed considered to be the best indicator of adrenergic evoked secretion of saliva. The levels of inorganic compounds, i.e., Ca++, K+ and HCO3–, are usually higher with sympathetic stimulation.
Besides the type of autonomic receptor being activated, the two other parameters that can affect salivary composition are the intensity and the duration of stimulation to the glands. The differences in composition between saliva collected after a change in the intensity or the duration of stimulation appear to be due to alterations in membrane permeability of secretory cells leading to changes in the rate at which electrolytes are lost from these cells.
The secretory cells are not the only glandular elements that respond to stimulation of the sympathetic innervation. Myoepithelial cells and blood vessels of the glands also respond to such innervation, and these responses can in turn modify the quantity and composition of the elaborated saliva. It has been shown, for example, that sympathetic stimulation to salivary glands can produce a markedly increased degree of vasoconstriction. Finally, other factors such as circannual rhythms and reflexly induced secretomotor responses might also influence salivary secretion.
Effects Of Exercise On Saliva Secretion And Its Composition
Several studies have shown decreases in salivary levels of immunoglobin A (s-Ig A) in response to high-intensity exercise. Lower resting levels of s-IgA have indeed been reported in cross-country skiers and in elite swimmers, when compared to matched controls of sedentary individuals. The levels of s-IgA decrease following intense exercise, and return to normal levels after 60 minutes from cessation of activity. Since Ig A represents the first line of defense against potentially pathogenic viruses, the exercise-induced decrease in s-IgA could contribute to the higher incidence of upper respiratory infections associated to strenuous athletic training. However, endurance exercise performed at lower intensities (i.e., training protocols within the guidelines recommended by the American College of Sports Medicine), does not seem to alter normal s-IgA levels.
Salivary flow rate appears to be modified during physical activity, according to most studies. Nevertheless, interpretation of the results obtained in these studies is sometimes difficult due to some methodological limitations, concerning mainly exercise protocols and saliva collection procedures. During exercise, salivary levels of total protein can be increased, since saliva secretion is then mainly evoked by action of adrenergic mediators. Exercise is indeed known to increase sympathetic activity and the high protein concentration following exercise may be due to increased ß-sympathetic activity in salivary glands. This elevated levels of protein could also be caused by the increase in blood catecholamines associated to exercise. During prolonged exercise at low to moderate intensities (lower than 60% of ![]() O2max), salivary secretion does not seem to be significantly modified. At higher intensities, however, salivary secretion decreases. Factors associated to high-intensity exercise such as an increased ß-adrenergic activity, dehydration, or evaporation of saliva through hyperventilation (although less probable) have been proposed to explain this lower secretion of saliva at high workloads.
O2max), salivary secretion does not seem to be significantly modified. At higher intensities, however, salivary secretion decreases. Factors associated to high-intensity exercise such as an increased ß-adrenergic activity, dehydration, or evaporation of saliva through hyperventilation (although less probable) have been proposed to explain this lower secretion of saliva at high workloads.
Salivary levels of cortisol are considered to be a good indicator of the adrenocortical response to exercise by some authors, since salivary cortisol closely reflects plasma free cortisol levels, presenting advantage over total cortisol measurements. During exercise, salivary and serum concentrations of cortisol are indeed very similar. In addition, both salivary and blood levels of cortisol increase with exercise intensity until a certain exercise level, at which such increase loses it linearity. This inflection point in the increase of salivary and blood levels of cortisol coincides in most of the cases with the onset of blood lactate accumulation. It has been suggested that this lactate accumulation might activate chemoreceptors within the working muscles, which in turn could stimulate the hypothalamic-pituitary axis. However, a true cause-to-effect-relationship between these variables remains to be proven. Both increases of cortisol and lactate levels could occur as a result of a marked sympathetic activity or an increase in blood catecholamines which take place at exercise intensities above anaerobic threshold.
The effects of exercise on the salivary and serum levels of Na+ and K+ have also been studied. Prolonged exercise does not appear to have a significant effect on the serum Na+ and K+. On the other hand, the salivary Na+ concentration markedly increases whereas no noteworthy changes seem to occur in salivary K+, in response to prolonged exercise. In addition, this increase in the salivary Na+/K+ ratio is positively correlated to the exercise-induced increase in salivary protein concentration.
In our laboratory, we have studied the relationship between anaerobic threshold and variations in salivary electrolytes (Na+, K+, Cl–) in response to incremental exercise. Our results evidenced that salivary Na+ and Cl– showed a dual response to exercise: their levels decreased or remained stable during early phases of exercise, until a certain exercise level, at which they began to show a systematic increase. In contrast, K+ levels did not significantly vary during physical activity. The inflection point in the salivary Na+ and Cl– was highly correlated (r= 0.82; p<0.01) with lactate threshold, suggesting the possibility of determining anaerobic threshold with a noninvasive method involving saliva analysis.
These changes in the concentration of salivary electrolytes which occur at a certain exercise intensity might be elicited in response to sympathetic stimulation. This sympathetic stimulation might induce changes in salivary flow and in both reabsorption and secretion of electrolytes in secretory cells. The decreased in saliva secretion associated to exercise could also be the result of a reduction of blood flow to salivary glands caused by elevated adrenal-sympathetic activity. The results of our investigations demonstrate the existence of a catecholamine threshold highly correlated with blood lactate increases (r= 0.84, p<0.01) during incremental exercise. This catecholamine response which occurred at or close to lactate threshold was in turn well correlated (r=0.75, p<0.05) to the point (“saliva threshold”) at which salivary electrolytes (especially Na+) showed an inflection point. Although further research in this field is necessary, our experiments suggest that saliva composition analysis might be a good estimate of the adrenal-sympathetic response during exercise. We therefore propose this new noninvasive method for anaerobic threshold determination. We believe that its potential applications in both clinical and exercise physiology areas are numerous.
Salivary gland disorders are conditions that lead to swelling or pain in the saliva-producing tissues around the mouth.
Hyper-salivation may be associated with many disorders such as herpetic stomatitis, irritation by dentures and pregnancy, but drooling does not occur in these cases unless the ability to hold secretions within the mouth or the ability to swallow secretions is impaired. Patients with hyper-salivation may expectorate repeatedly, but this is not drooling. It is the difference between salivary production and the ability to swallow saliva that results in drooling rather than the absolute production of saliva.
Difficulty in swallowing saliva is encountered at three levels of function: the oral, pharyngeal and oesophageal components of deglutition. Some of the common disorders associated with drooling, classified according to the presumable level of malfunction, are as follows: oral (cerebral palsy, Parkinson’s disease, motor-neurone disease, seventh-nerve palsy, facial disfigurement and radical cancer surgery); pharyngeal (motor-neurone disease, myasthenia gravis and polymyositis); and oesophageal (carcinoma or stricture).
Salivary Dysfunction
Too much or too little saliva can affect oral health and quality of life. Lack of saliva leads to dental decay, oral yeast infections, taste problems, bad breath, difficulty speaking and swallowing, and recurrent salivary glands infections. Too much saliva can cause social problems and may be a sign of an underlying medical problem. We evaluate salivary problems by medical history review, head, neck and oral examination, diagnostic imaging, and salivary function measurements. Management strategies for improving salivary function and preserving oral health are developed for each individual.
Tooth Erosion
Dental or tooth erosion is defined as a dissolving of tooth surfaces caused by acidic substances. (This is different than tooth surface loss caused by caries-producing bacteria.) Generally, in a given individual, all or most tooth surfaces are affected. Sources of acid may be from outside of one’s own body (dietary or environmental) or from inside the body (e.g. acids from the stomach). Erosion may also be related to salivary function. Evaluation of this condition includes a medical history review, head, neck, and oral examination, and salivary function measurements. Treatment depends on the cause of the erosion.
Taste Disorders
The following taste disorders are evaluated and treated:
· Loss of taste
· Persistent unusual or unexpected tastes
· Perversions of taste (for example, when something sweet tastes salty)
Evaluation includes medical history review, head, neck and oral examination, diagnostic imaging, salivary function assessment, and testing of ability to taste and smell.
Good mouth care is important to maintain quality of life. Speaking, the pleasure of eating, and the normal handling of saliva are taken for granted by most of us. It may be difficult to imagine the impact mouth disorders have on patients. As the mouth is largely hidden, the patient, family, and caregivers may not recognize problems when they occur. As an exercise, the reader is encouraged to consciously hold his or her mouth open for several minutes. Saliva will begin to pool about the lower teeth. At the same time the tongue will dry. Drooling eventually will occur. Suddenly, what we have taken for granted, swallowing spit, becomes precious.
Xerostomia (Dry Mouth)
Common causes of xerostomia are
· medications (anticholinergic agents, opioids to a lesser degree, clonidine)
· dehydration
· mouth breathing
· surgery or radiotherapy to the mouth
· infections of the mouth
Dry mouth is very prevalent and troublesome. As this list suggests, treatable causes are common. Taking patients off of unnecessary anticholinergic medications, for example, can be of great help. Other causes, such as dehydration, radiation-related xerostomia, and mouth breathing may be harder to address directly.
The relationships between dehydration, thirst, and dry mouth are complex and frequently misunderstood. They are discussed in more detail in the chapter 6. While systemic dehydration undoubtedly contributes to decreased saliva production, rehydration with IV fluids, for example, does not necessarily correct the problem and may be associated with undesired side effects, such as worsening respiratory secretions. Side effects of medications, especially anticholinergic agents and opioids, and mouth breathing may significantly contribute to this symptom
Difficulty Handling Saliva, Drooling, and Sialorrhea
In rare cases patients may produce excess saliva. More commonly, they have difficulty handling normally produced saliva because of alterations in mouth anatomy or because of impaired neurologic control of the swallowing reflex. The latter, often manifested by drooling, is the more common. Drooling carries a great social stigma and can be very disturbing to patients and families. Patients with Parkinson’s disease, amyotrophic lateral sclerosis, cerebral vascular accidents, dementia, and developmental disorders are prone to this. Patients in the very advanced stages of dying may also experience difficulties as they loose their swallowing and cough reflexes.
Usually, the underlying cause is untreatable. However, anticholinergic agents can be of some help in decreasing salivary flow. Care should be taken in using systemically absorbable agents, as they can produce troubling side effects. In addition, for some patients the dry mouth that results from medication may be as troubling as the earlier drooling. Studies in developmentally delayed children and more recent studies of adults who drool suggest that glycopyrrolate may be effective in decreasing salivary production with little, if any, systemic toxicity.56,57 Glycopyrrolate is an anticholinergic agent that is poorly absorbed from the GI tract and that minimally crosses the blood-brain barrier if given systemically (as it often is in anesthesia). I have had some success with this agent. Tablets of 1 mg can be dissolved in a small amount of water and held in the mouth (or swabbed onto mucosa if unable to be held) and then spit out. This is usually given BID or TID. If swallowed, glycopyrrolate will have a strong local anticholinergic effect on the GI tract and decrease motility and secretion into the gut. This will worsen constipation or treat diarrhea but decrease the systemic effect, as only 5% of the drug is absorbed. As the goal of therapy is to reduce the production of saliva, not to dry the mouth completely, the mouth should be moistened with artificial saliva if secondary xerostomia results.
Candidiasis
Candidal infections of the mouth occur frequently, especially in patients who are on steroids and in diabetics. Thrush is relatively easy to recognize. White cottage cheese-like plaques are found, often associated with tenderness, dysphagia, and altered taste (dysgeusia).
More difficult to recognize are the atrophic forms, both acute and chronic. Acute atrophic candidiasis usually presents as a reddened tongue with depapillation, which is also associated with dysgeusia. It is my impression that this form may be more common in patients with xerostomia, as inadequate moisture exists to create classic thrush. Vitamin deficiencies, poor nutrition, and xerostomia itself may all create a similar picture, making definitive diagnosis difficult on exam alone. Chronic atrophic candidiasis is similar to acute (reddened mucosa, especially in the area where upper dentures are in contact with the palate) and is most common in elderly patients with dentures. It is often associated with angular cheilitis, which is painful.
A variety of antifungals can be employed in therapy. Nystatin suspension is often well tolerated, as it is a liquid. Because efficacy relates to drug contact time with the mucosa, some caregivers make small “popsicles” with toothpicks for patients to suck on. Some strains of candida are resistant and may respond better to other agents. Mycelex troches are typically given five times a day, although less frequent administration can be given to the dying. Patients with significant xerostomia may have trouble dissolving troches. Systemic agents, such as fluconazole are rarely required and are expensive. Fluconazole may be indicated for resistant strains and when candida is suspected beyond the GI tract, such as when a patient has new-onset hoarseness with a sore throat in association with oral candida (often indicative of laryngeal involvement).
Viral and Bacterial Infections
Immuno-suppressed patients are at a higher risk for both viral (predominantly herpes simplex) and bacterial infections. Herpes infections should be suspected when such patients have new-onset pain or odynophagia (common with esophageal herpes); it is best treated with acyclovir. Patients with xerostomia appear to be at higher risk of bacterial parotitis and present with the sudden onset of a firm, warm, painful swelling under the angle of the jaw. They may be susceptible because of decreased salivary flow from the parotid gland. Broad-spectrum treatment with an antibiotic is usually effective.
The salivary glands may become inflamed (irritated) because of infection, tumors, or stones.
Symptoms
· Abnormal tastes, foul tastes
· Decreased ability to open the mouth
· Discomfort when opening the mouth
· Dry mouth
· Pain in the face or mouth pain
· Swelling in front of the ears
· Swelling of the face or neck
Tests vary depending on the condition thought to be causing the problem.
· Images of the glands can be seen using ultrasound, MRI scan, and CT scans of the glands.
· The ducts of the mouth can be investigated using an x-ray called a sialogram.
· A salivary gland biopsy can be used to diagnose problems with the salivary glands.
Prevention
Most of the problems with salivary glands cannot be prevented. Drinking enough fluids, using things that increase salivation, and massaging the gland can increase the flow of saliva and help prevent infection.
Treatment
Drinking a lot of water, using sugar-free lemon drops to increase the flow of saliva, and massaging the gland with heat may help with infections and stones.
Antibiotics are used for bacterial infections.
Stones may be removed using endoscopes, lithotripsy, or surgery.
Other treatments depend on the specific disorder.
Salivary Gland Swelling:
Salivary gland swelling can occur when one of the ducts that carry saliva from the salivary gland to the mouth is blocked. Pain may occur, especially during eating.
The most common cause of blockage is a stone. Salivary gland stones are most common in adults; 25% of those with stones have more than one. A stone can form from salts contained in the saliva. Blockage makes saliva back up inside the duct, causing the salivary gland to swell. A blocked duct and gland filled with stagnant saliva may become infected with bacteria.
Mumps is an infection caused by a virus and can cause:
· Fever
· Headache
· Swelling and tenderness of glands in one or both sides of the neck (called parotitis)
· Running nose and eyes, sore throat and ears particularly in young children.
Occasionally serious complications of mumps infection can occur. These less common, but more serious symptoms include:
· A meningitis
· Ear infections which can lead to hearing impairment.
· Swelling and tenderness of the testicles in adult men (orchitis), and inflammation of the ovaries (oophoritis) in women, though it is very rare for these to cause serious complications such as infertility.
· Pancreatitis inflammation of the pancreas.
Estimation of salivary glucose, salivary amylase, salivary total protein and salivary flow rate in diabetics
Considering the prevalence of diabetes mellitus and its oral manifestations, it has become of paramount importance to study the levels of some crucial parameters in diabetic saliva.
Salivary glucose
Mean salivary glucose levels were higher in the uncontrolled and controlled diabetic groups than in the healthy non-diabetic group and the differences were highly significant. Uncontrolled diabetics had higher mean salivary glucose levels than controlled diabetics.
Salivary amylase, total protein and flow rates
The findings were not significantly different when diabetics and healthy non-diabetics were compared for salivary amylase, salivary total protein and salivary flow rate, although mean salivary amylase levels were significantly lower in the controlled diabetic group than in the healthy non-diabetic group.
Duration and type of diabetes mellitus
No statistically significant intergroup or intragroup correlations were seen for the uncontrolled and controlled diabetic groups based on duration and type of diabetes mellitus.
Gender of participants
Each study group was analyzed for gender differences with regard to salivary parameters. Mean salivary total protein levels were significantly lower in uncontrolled diabetic males than in uncontrolled diabetic females while mean salivary stimulated flow rate was significantly higher in uncontrolled diabetic males than in uncontrolled diabetic females.
Discussion
Oral pathophysiology and general diabetic complications are complex, and there is considerable heterogeneity within the diabetic population with regard to the development and progression of such complications.
Salivary glucose
Mean salivary glucose levels were clearly higher in diabetics when compared with healthy non-diabetics. For salivary glucose levels, the results of the present study are in accordance with most previous studies (2,5,9-18,42). Normal glucose levels in saliva are 0.5-1.00 mg/100 ml, and do not significantly affect oral health or support the growth of microorganisms. However, higher salivary glucose levels favor the proliferation of microorganisms and enhance their colonization on teeth and oral mucous membranes. Glucose serves as a nutrient for candidal microorganisms and suppresses the killing capacity of neutrophils, which further accentuates colonization and likely consequences can be proposed as a result of these elevated salivary glucose levels in diabetes (1,4,15). Oral diseases that may be ascribed to the elevated salivary glucose levels include candidiasis, dental caries, gingivitis, periodontal disease, increased risk of infection, burning mouth, fungal infections, taste impairment and poor wound healing. Prolonged xerostomia may also be a contributing factor to these conditions. The elevated salivary glucose level in diabetes also confirms the effects of diabetic membranopathy, which leads to raised percolation of glucose from blood to saliva, thus altering the salivary composition in diabetes mellitus.
Salivary amylase and salivary total protein
The significantly lower mean salivary amylase levels in controlled diabetics when compared with healthy nondiabetics seen in the present study supports the study by Yavuzilmaz et al.who linked them to hormonal and metabolic changes occurring in diabetic patients. However, the results were insignificant for uncontrolled diabetics inour study. In contrast, significant increases in salivary amylase levels have also been demonstrated in diabetics.


{kind=link}
{kind=link}