Caring for patients with disease of the eye additives and the eye layers.
USHER SYNDROME
Retinitis pigmentosa is an eye disease that occurs rather often in the deaf and hard of hearing. Most often both the hearing loss and the retinal disease are caused by the same inherited disorder that is called Usher syndrome. Deafness or partial hearing loss is present at birth (Usher Type I and II) or develops later (Usher Type III) and retinitis pigmentosa develops its symptoms later. It becomes increasingly difficult to see in twilight and in the dark.
The word retinitis means inflammation of the retina and is actually a wrong name because RP is not an inflammation but a degeneration of the retina. The word pigmentosa comes from the word pigment that means colour substance. The outermost layer of the retina is pigment epithelium with pigment containing cells. Retinitis pigmentosa first affects the pigment epithelium and the rod cells, and later the cone cells and other retinal cells.
Doctors express themselves saying that Usher syndrom is a “combined loss of hearing and vision” because of sensorineural hearing loss and degeneration of the retina. The word syndrome means that the disease affects several organs (eyes and ears) in a typical way. Sensorineural hearing loss means that the damaged cells are the hearing cells of the inner ear. Degeneration of the retina means that retinal cells, rods and cones, die very slowly, the rod cells earlier, the cone cells later. Loss of retinal functions leads to loss of visual field and other changes in vision.
There are other syndromes that cause loss of hearing and vision but they are more rare than is Usher syndrome. It is also possible that a person who lost his/her hearing for another disease later develops retinal disease. Or a person who is visually impaired may develop hearing problem later in life. Not everyone who has hearing problem and retinitis pigmentosa has Usher syndrome.
One of the common symptoms of RP is photophobia, light sensitivity. It is especially important to remember light sensitivity in communication situations. It can be very difficult to see signs and to lipread if one is dazzled. The interpreter should always arrange the ligths so that the person can see as well as only possible. It would be good to have a dark surface behind the interpreter and have the interpreter wear dark clothing. During summer it may be unpleasant to wear a dark blouse. Then it is better to use a dark apron with sleeves and collar if the deaf person is very light sensitive. Some interpreters may not know the importance of good illumination so they need to be reminded about it.
Another thing to consider is how far and where the interpreter should stand or sit in order to be within the limited field of the visually impaired person. We usually call it communication-field. It is the area that the person can see without moving his/her eyes. The interpreter should always know the size of the communication field. Otherwise he/she may use too large signs.
Changes in vision occur in different Usher persons at different ages. This is called individual variation. Night vision deceases first, then color vision and visual field, and later visual acuity. Some Usher-patients have difficulties in balance function (Usher Type I).
Heredity
Usher syndrom is inherited from both parents. They both have the abnormal gene that is needed to cause the disease. Only some of their children get the disease. Every child either gets it or does not get it. The risk is that about every fourth child will inherit the disease but since every child has the same chance, it is possible that only one child has it or that even all children may have it.
If an Usher individual wants to have children, he or she is likely to have normal children if the partner does not have the RP disorder in his family. The children, however, all are carriers of the abnormal gene.
All Usher individuals should have genetic counseling at school and when planning their family. Knowledge about the genetic mechanisms and risks does not usually affect the decision to get married to someone but it may affect the decision to have children.
Usher children at school
The oldest child with Usher syndrome in a family is often diagnosed first at school age. It is possible to make the diagnosis earlier if there are any symptoms of decreased night vision or visual field (the child starts looking at his feet when going down the stairs). The visual fields can be measured at the age of 5-6 years in many deaf children and easily at the age of of 7-8 years. All children with sensorineural hearing loss are suspect of Usher syndrome until it is proven that no visual changes develop.
Because Usher syndrome may lead to very poor vision at the age of 25-50 years, it is important that these children have the best possible teaching and motivation in learning language skills, both sign language and written language; also spoken language if possible. Good written language is necessary for learning braille if print is no longer seen.
It is much easier to adjust to live with the dual sensory impairment if the child grows up with that knowledge. Many deaf youngsters go throug a really difficult time in their life when they learn about the visual impairment at 16-18 years of age. A good adjustment requires understanding and acceptance by the family, the teachers and the peers. Therefore it is important that all deaf children learn about visual impairments and learn to live with the visually impaired deaf individuals among them.
DISEASES OF THE OUTER EYE
Inflammations and small traumas of the cornea are common. Usually they heal quickly but are often painfull. There is one exceptional infection that is nearly painless, beginning herpes simplex-infection. It is an infection of the nerves and therefore the pain sensation is diminished. Because the eye does not hurt, a patient with herpes simplex keratitis (keratitis = inflammation of the cornea) may not realize that he should be treated. Quite often the infection has prevailed weeks or months before it is diagnosed.
Corneal erosions, small wounds, may be caused in many ways: a comb, a scarf, or a piece of dirt may scratch the surface. Superficial corneal wounds heal in a few hours if the eye is treated with ointment and kept closed for a couple of hours. It is best to keep both eyes closed so they do not move.
|
A. |
|
B. |
|
Small scratches and wounds are easier to see if the surface is stained with fluorescein. A. Dry fluorescein ”sticks” can be used to apply small amount of the dye on the conjuntiva of the lower lid from where it spreads into the tear fluid and stains the wound. B. A healing wound has cloused, the surface is even but under the thin epithelial layer is a drop of fluid that delays the growing of the cells into the deeper layers of the cornea. At this stage the wound is easily torn open, especially in the morning if the lid has adhered to the wound area where the tear layer is not normal. |
||
If the wound is not allowed to heal well, it easily breaks open a new. If this happens several times the wound may not heal completely but becomes a recurrent wound breaking opeow and then. The eye is then painful, watering and light sensitive. The healed wound is often torn open in the morning when the eye lids are opened. During the night less tears are formed than during the day. The lid may adhere to the healing surface of the wound and pull it loose when opening. It is therefore important to use lubricating ointment each night at least a week after the trauma. If a recurrent erosion is present it is ofteecessary to use the ointment for at least six months.
Inflammation of the conjunctiva, conjunctivitis, is common when a person has flu or common cold. The discharge and watering usually disappear without medication, sometimes antibiotic drops are needed.
Allergic reactions make eyes itching, irritated and watering. The best treatment of allergic reactions would be to avoid the allergen but often it is not known. There are many different medications, pills, eye drops, and nasal sprays to reduce the symptoms. Eye drops that contain cortison-like medications, steroids, should be used sparingly. If they are needed for a longer time, an ophthalmologist should take care of the patient. Since the reaction is superficial, medications that do not get deeper into the eye should be used. Among steroids, hydrocortison does not enter through the cornea.
Conjunctiva may swell sometimes. The loose conjunctival tissue may swell so much that part of it hangs outside the lids. It looks bad but is not dangerous. Conjunctival oedema is caused by allergic and toxic reactions: insect bites, plant juices (often geranium), dusts, or food allergens. Swelling disappears in a few hours to few days. It disappears more quickly if the eyes are covered with cold, dry compress (crushed ice in plastic bag wrapped in a towel). Decongestive eye drops help, too.
RETINAL DEGENERATIONS
Retinal degenerations are a large group of diseases. Macular degenerations involve the tiny central area of the retina that we read with. That area is called macula. There are several different types of macular degeneration. The most common type is the so called ‘dry’ macular degeneration, where the central retina disappears as small patches or as one slowly growing solitary area.

Fig.16a. Changes in the macula may look very small. In the visual field examination there are losses in the very centre of the field: dark grey patch in the picture to the right means severe loss of function and the light grey patches somewhat less severe loss of function. Because of these changes the person uses retinal functions around the central retina to read texts. The person sees still nearly normally in the minute area in the center of the visual field marked with a light grey dot and therefore has “normal central acuity” but the area is too small to allow reading, only one letter at a time can be read with it.
At the places, where the retinal layers have disappeared, also choroidal structures have vanished and bare sclera is visible behind the largest choroidal vessels. If its function becomes disturbed it is still possible to read with the retina surrounding the macula. Because the surrounding retina does not see as well as does the macula, a person with macular degeneration has to use larger texts or magnify the text with a magnifying lens or strong reading glasses. If still greater magnification is needed it is possible to use a TV- reading aid, CCTV (closed circuit television).
Figure 16b. Macular degeneration with decrease in visual acuity causes need of stronger and stronger reading glasses. If the person is myopic, reading without glasses or with a close circuit TV reading aid may be good techniques. Use of talking books and braille are options when reading print becomes too slow.
Macular degeneration makes lipreading and reading of finger alphabet difficult. A person with macular degeneration should remember to ask people to talk more slowly, to pronounce words carefully and to stand facing the light. Then it would be easier to see the lips. It would be still easier if people who talk to the hearing impaired use a contrast pen to accentuate the lip margins. There are also brown contrast pens so one does not need to use lipstick and a red contrast pen.
Peripheral retinal degenerations usually start in the midperipheral retina, in an area surrounding the central retina. Later during the course of the changes peripheral retina may loose its function. Eventually only the central retina functions, the person has tunnel vision. The first symptom is often night blindness, difficulties seeing in twilight and in the dark.
Since it is difficult to explain how one sees when vision has become abnormal, I have written a list of questions. Interpreters have found them important because they are often used during a visual assessment. This list may help the interpreters and the patients to be better prepared for the visit to the doctor’s office.
Questions:
1. Vision in twilight.
- Do you see poorly in twilight and at night?
- If you wait in the dark, do you start seeing better?
- How long a time do you have to wait?
- When you go into a dark room, does your field of vision become smaller?
- There is often very little light in the trains and busses. Is it difficult to see on trains and busses?
- Is it difficult to go from a brightly lighted area to a place in shadow?
- When you go into a store, do you have to stop at the door and wait for a while before you start seeing in the store?
2. Light sensitivity, photophobia, dazzle.
- If the sun is shining into your eyes, does your vision become much worse?
- Does the sun dazzle you for a long time? How long?
- Does bright light cause pain in your eyes?
- Do you use sunglasses? Goggles?
- Do you have several different sunglasses? How many?
- Do you bump into people even if you are wearing your sunglasses in bright light?
- Do car head lights dazzle you?
3. Disturbances related to motion.
- Is it difficult to move in places where people walk close by?
- If you walk in a place where the wind moves branches of bushes and trees, does the movement of the branches bother you?
- If you turn your head quickly, does it bother your vision?
- If movements disturb your vision, what happens to your vision when it becomes disturbed? How does it change?
4. Contrast sensitivity.
- Can you see the curb?
- Can you see the stairs when you walk downstairs?
- Do you see the poles of traffic signs in time?
- Is it difficult to see light coloured food on a white plate?
- Has it become more difficult to read lips and fingerspelling?
- Is the newspaper text difficult to read because of the light ink in the print?
5. Illumination.
- Is it uncomfortable to sit facing a window?
- Do you find small local lights, like candles, disturbing?
- When you read, how do you want to arrange the lights in the room and the reading light?
- What colour of light is most comfortable? Do you use filter glasses when reading?
- Does extra light make reading small texts easier?
- Look around at home and think which lights should be moved to another place? Where you would like to have more light?
- Are the street lights strong enough? Do you need a flash light?
6. Visual field.
- How large an area do you see in front of you?
- Do small objects disappear from your vision and pop up after a while?
- Since you have loss of vision in parts of your field of vision, have you sometimes misunderstood a situation?
- How many letters do you see clearly without moving your eyes?
(This is asked when you read different sizes of test texts. Look at several different texts at home in different illuminations and at different distances to find out what you find best. Write down the reading distances and bring the texts with you.) - When you read, can parts of the letters disappear?
- If you use sign language, does the person signing have to go further away to be seen?
- How much of the interpreter do you see without moving your eyes around?
7. Visual illusions.
- Is there flickering of the picture (image) in any part of your field of vision?
- Do you see lights moving around (near) the blind areas of your field of vision?
- Are there any other lights moving in the visual field? How do they look like?
- If you cough or laugh, does the image change?
- If you see lights moving across the visual field, do you see your surroundings as through a frosted glass? Or does the image disappear? Do straight lines become different? How?
8. Progression of the disease.
- When did you notice the first changes in your vision? Before school age, at school, after school?
- How rapidly did the changes develop then?
- Has there been any change in your vision during the last year? During last five years?
- Has there ever been a period of very rapid progression of the changes? When? How did your vision change then?
- Have colours become different?
- Do you have difficulties with any colours?
- Has your reading speed changed? How much? When?
- Do you have any pain in your eyes?
9. Visual aids.
- Do you have several pairs of glasses? ( If you do, please, bring them all to the office. Bring also all other devices.)
- Do you have tinted glasses? Sunglasses?
- Do you use magnifying lens(es)?
- Do you have a telescope?
- Do you use any other visual devices?
- Which visual devices would you like to try this time?
It is often difficult to be sure that one has understood the question correctly. Do not hesitate asking the doctor whether (s)he could ask the same question using other words.
In order to understand what might happen in different diseases, it is good to know more about the retina.

Fig.16c. Structure of the retina.
A.The basic organisation of the retina. The inner layers of the retina (ganglion cells and bipolar cells) are transparent. The light traverses the inner layers and is absorbed in the outer segments of the sensory cells. When the light is absorbed there are chemical and electrical changes in the sensory cells. These changes are transmitted to the bipolar cells and from there to ganglion cells, that in turn send the information as an electric impulse into the brain. B.Sensory cells, rods (R) and cones (C), pigment epithelium (PE) and choriocapillaris (ChC). The outer segments of the sensory cells (the striped part) have lamellae. The visual pigment that absorbs the light, is located on these lamellae.
Although the word retinitis means inflammation, retinitis pigmentosa-disease is not an inflammation but a degeneration of the retina.
When the cone cells are affected, loss of visual field starts as small patches around the central vision. These patches grow slowly to form ring scotoma around the central vision. Then the person sees within the central field and in the peripheral vision but not in between. It is often difficult to understand such vision. Especially children may be puzzled by small objects disappearing and reappearing. Children sometimes believe that someone is teasing them and making things to disappear.
|
|
Fig 17. Changes in the visual field start as small patches. They are not seen white or black, but “empty”. When they are small they are difficult to notice. The patches grow slowly and form a ring, ring scotoma. Later only the central visual field functions, the person has tubular field, tunnel vision. |

When the peripheral vision disappears the person may have a small central visual field called tunnel vision.
Changes in the retinal cells often cause peculiar lights, illusory lights, to appear. To many retinitis pigmentosa patients these lights look like shiny sausage-formed balloons and appear at the edge of the functioning central field. If a child sees such lights he/she may not understand why other persons do not want to look at the lights. All children who mention seeing lights that are not there should be carefully examined by an ophthalmologist.
Some persons with retinitis pigmentosa see wiggling lights going across the visual field. The different lights may apppear at different ages in different individuals. Not all persons with retinitis pigmentosa see these illusory lights.
Sometimes the light phenomena are seen after coughing, sneezing or laughing. The visual field may also become much smaller for a while and slowly increase to its usual size.
There are half a dozen pictures related to retinitis pigmentosa in the German text Funktionales Gesichtsfeld and in the corresponding English text Functional Field of Vision.
Nearly one half of all persons with retinitis pigmentosa and many other visually impaired are disturbed by photophobia. Light falling directly into the eyes causes dazzle. Light coloured surfaces may also reflect enough to disturb vision.
Decreased contrast sensitivity is a common feature of retinitis pigmentosa and several other eye diseases. It means that the person does not see faint shadows, (s)he needs high contrast in order to see. Lips are easier to see if the person uses a contrast pen or lipstick.
Decreased contrast sensitivity can be a problem in play situations. One of my young patients was left alone to ski in a birch forest on a cloudy winter afternoon. The contrasts between the white birch trees, cloudy sky and newly fallen snow were very low. The child could not find his way out of the forest. Persons with limited vision should never be left alone in places where they might not find their way.
Sighted Blind
We call RP-patients with tunnel vision “sighted blind” because they behave as if they were both sighted and blind. They move about using the white cane to find their way into the bus or train and sit down and start reading their newspaper without glasses. Quite often the people around the RP-patient react negatively, sometimes hostily, because they cannot understand why a “blind” person can read small text. We should explain them that there are people who need to use the white cane because of small field but who can read print.
If the visual field is limited, the further away one looks, the more one sees. Many RP-patients have reported that they do not experience particular difficulties when driving. As one of them put it, “It is not difficult to drive, but it is difficult to find the car in the parking lot”. The RP-patients may be unaware of the dangers they come close to in trafic. Every person who has changes in his/her visual field should let his/her driving capability be tested at regular interwalls.
DIABETES
Diabetes can cause changes in the eyes. Therefore the eyes of an diabetic person are examined regularly. The smallest vessels of the retina, the capillaries, may become closed or their diameter may become wider thaormal. This causes oedema, swelling of the retina and small haemorrhages. This is called diabetic retinopathy. If the control of diabetes is good, changes in the retina develop very slowly.
|
A. |
B. |
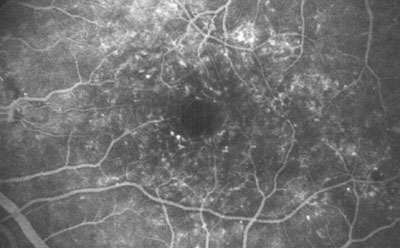
Fig.18a. Fluorescein angiograms of retinal vessels in patients with diabetic retinopathy. In diabetic retinopathy the wall of capillaries may be damaged so that fluid diffuses into the retinal tissue more thaormally causing oedema. Small distentions of the wall, microaneuryms, are seen in fluoresein angiograms as bright dots. This angiogram was taken in 1974 when photocoagulation was used instead of laser treatment. The round black areas are scars of the photocoagulation burns. Changes of the vessel wall become less and less after the treatment and during good basic care of diabetes. Central vision of this person is good 25 years after a period of rapidly increasing vascular changes, which demonstrates the great value of both photocoagulation treatment and good basic care.
|
|
Fig.18b.Collection of blood between the retinal surface and vitreous after bleeding from new formed vessels, meovascularisation. There is a risk of a bleeding like this bursting into vitreous. |
In some diabetic patients, new formed vessels start to grow on the retina. These vessels have very thin walls and bleed easily. The blood may collect in front of the retina or burst into the vitreous making the image blurred. Diabetic changes in the retinal vessels are destroyed with laser burns.
Fig.18c. Examination using 3-mirror contact lens on the cornea. The contact lens contains mirrors that reflect the light into different parts of the retina. A lens like this is used also during the laser treatment.
Laser treatment means that small laser burns are used to reduce retinal oedema and to destroy vessels that might cause bleeding. In most cases the diabetic changes can be brought under control, the vision of the patient remains good. Sometimes so much of the retina must be destroyed that night vision is decreased. It is, however, a reasonable price if the other functions of the retina remain good or fairly good.
IRITIS
Iritis can occur at any age. It is rare in childhood. Children with rheumatoid arthritis may have iritis without having its usual symptoms. Therefore their eyes are checked regularly.
Iritis usually causes pain and redness of the eye, the eye may be very light sensitive, too. As one looks at near with the inflamed eye, it may hurt badly. When we look at near distance the small muscles of the iris contract. Contraction of the inflammed muscle causes the pain.
In young children iritis is often quite symptom free when it occurs with inflammation of a joint, a rheumatoid reaction. Also the swelling of the joint may have developed unnoticed, so the child may come to an ophthalmologist because of decrease of vision, caused by cataractous changes in the lens. In such a case inflammation must have been present for weeks or months.
Iritis should be treated as soon as possible. It is best to go to the emergency clinic or to the eye doctor’s office if you can go there without delay. It is important not to make an appointment which usually means several weeks of waiting.
The treatment of iritis is based on rest and steroids, cortison-like medications. Rest is instituted by using dilatation of the pupil, then the small muscles cannot contract.
The eye may become quite comfortable in a few days but the treatment is continued for weeks and often months until the interior of the eye looks normal. If the treatment is discontinued too early, the symptoms may reappear. Iritis tends to be reactivated by viral infections now and then. If one has had the symptoms once, they are easily recognized the next time. The treatment is always the same.
EMERGENCY SITUATIONS
Eye diseases that require immediate care are very rare. Actually only one situation is real emergency: if the vision disappears in one eye as if the light was switched off. The treatment should be started as soon as possible. The cause of the sudden disappearance of vision is disturbance in the circulation of the eye, the retinal artery is blocked. The treatment should be started within an hour at the latest, otherwise the retinal cells would be too badly damaged and could not recover.
If you need an interpreter in the emergency situation, it is important to inform the hospital that you need an interpreter. The clinic may not have interpreters for emergency patients and a young doctor may feel confused if exposed suddenly to an emergency situation with communication difficulties.
All accidents should be taken care of immediately but there is usually no great hurry. It is more important that the patient is transported calmly with both eyes covered. If the patient is a young child only the traumatized eye should be covered.
If an eye becomes reddish, painful and vision becomes blurred, the reason for the symptoms should be found out within a day. It may be iritis, glaucoma, or corneal or optic nerve inflammation.
Small flashes of light, that appear in a certain part of the peripheral visual field when one enters a darker room, may be a symptom of retinal detachment and should be checked.
Eyes are moved by six eye muscles. If one of the muscles is paralysed the patient develops double vision, diplopia. The two images are further away from each other when the person looks in the direction of the paralysed muscle’s action. If the head is turned to compensate for the loss of action, double vision disappears. It is easier to get rid of the disturbing double image by covering one eye. If there are no other symptoms there is no emergency situation. Double vision is usually caused by circulatory disturbance in the nerve that innervates the muscle. The family doctor can take care of the basic examination and consults an ophthalmologist if needed.
Sometimes a small blood vessel bleeds on the surface of the eye. The white part of the eye may become blood red. Bleeding under the conjunctiva, sugillatio, looks frightening but is quite harmless. It is comparable to a bruish in the skin, on the eye it only looks worse.
Bleeding under conjunctiva or sugillatio disturbs the family and neighours more than the person him- or herself. It requires no treatment and disappears in a few days.
The eye lids may become so swollen that it is impossible to open the eye or the conjunctiva hangs outside the eye lids. First aid is to fill a small plastic bag with crushed ice, wrap it in a towel and place it over the itching and burning eyes. Soothing eye drops can be obtained over the counter in most places. The symptoms usually disappear in a few hours. The reason for the lid swelling may be an allergic or toxic reaction. If only the right eye is swollen and the person is right handed the reason often is chemical, e.g. plant juice.
FIRST AID
The most common eye accident is a piece of dirt under the eye lid. If it does not come out with a few blinks it is wise not to blink any more but turn the eye lid and remove the dirt.
|
Fig 19. The eye lid is easy to turn over if one places a cotton swab just above the cartilage of the eye lid at the middle of the upper lid, and gently pulls from the lashes upwards as the patient looks down. |
|
If no obvious piece of dirt is visible it is good to wipe the conjunctival surface with a wet cotton swab. The piece may be very small or translucent. If the sensation of foreign body in the eye does not disappear it is best to contact an eye doctor. Quite often the irritating piece is so small that it is found only with a microscope.
Sometimes a drop of a chemical happens to get into the eye. All chemicals should be rinsed away immediately. In places where chemicals are used people should always use goggles and have rinsing solution at hand. Artificial tear fluid is a convenient rinsing solution in the first aid kit for travelling. It is a perfect ‘first aid’ during long flight when the tear layer on the cornea becomes too thin and uneven.
Systemic Management of Ocular Inflammation, Allergy & Pain
Ocular inflammation, allergy, pain and related anxiety share many common characteristics and therapeutic interventions. As a major component of inflammation, pain management often involves treatment of inflammation. As an outcome of the allergic immune response, inflammation can be managed by intervention in the hypersensitivity process. As pain perception is often modulated by anxiety, anxiolytic agents can be beneficial to pain control.
This course will be loosely divided into four categories; Inflammation, Allergy, Pain and Anxiety.
This course will review foundational terminology, anatomy and physiology of the eye and body pertinent to the management of ophthalmic inflammation, allergy, pain and related anxiety. This knowledge will serve as the basis for presentation of successful practices and pitfalls of systemic prescriptive pharmaceutical management. Specifically the course will present pharmaceuticals and biologicals that can be used in non-topical formulations to manage ophthalmic pain, allergy, pain and related anxiety. The mechanism of action, common clinical use, caution and adverse effect and case examples will be addressed for each category.
Inflammation Management: Anti-Inflammatories
Inflammation is a physiological process intended to protect and repair the body when threatened, injured and or invaded by agents recognized as “foreign”. There are three subclasses of inflammation: Traumatic, Immunogenic and Neurogenic inflammation.
Traumatic inflammation results from physical tissue damage.
(eg. Corneal abrasion)
Immunogenic inflammation develops where “foreign” substances contact and couple with immune cells. (eg. Bacterial conjunctivitis)
Neurogenic inflammation manifests when toxic substances encountered release neuropeptides that stimulate inflammation. (eg. Onion keratoconjunctivitis)
Each of these forms of inflammation can present acutely and or chronically.
Acute phase inflammatory response is frequently stimulated by an identifiable unsustained tissue insult. The response is rapid in onset with a distinct termination. The process is self regulated and usually abates in several days to a week following the triggering event. It is characterized by a predominantly exudative vascular response. The classic signs and symptoms of acute inflammation are:
- Pain
- Fever
- Edema or swelling
- Erythema or redness
- Dysfunction
Following an unsustained insult, acute inflammation unfolds in a predictable and generally well understood cascade of tissue activity. Understanding these physiologic and anatomical responses is necessary to determine if, when and what intervention should be initiated by the clinician.
Regardless of the type of acute inflammation, the signs and symptoms arise from insult to and response of cells and their membranes. In some instances the insult and response are localized to the same tissue (blunt trauma causing a black eye), while in others the response can manifest away from the exposure site (aspirin triggered asthma) or disseminate from the site of insult/exposure (staphylococcal septicemia). The basic mechanism of acute phase inflammation is initiated and mediated by phospholipids richly populating cell membranes. Whether it be physical damage, immunologic or neurgenic insult, cells produce arachadonic acid from cell membrane phosphotidyl choline combined with phosphotidyl inositol (Figure 1). Arachidonic acid is the primary building block for the vast majority of inflammatory mediators (Eicosanoids) (Figure 2.
Figure 1: Cell membrane phospholipid bilayer: home to phosphotidylcholine and phosphotidyl inositol which combine to form arachadonic acid.
Figure 2
As cell membranes and the cell machinery produce arachadonic acid the acute inflammatory cascades “wind up” developing the inflammatory tissue responses of vasodilatation, vascular endothelial activation and neutrophil (white blood cell) activation. The stages and sequence of the acute extracellular inflammatory process are seen in the following flow diagram (Figure 3).
Figure 3
Modifying or disrupting the activity of any or all of these stages will modulate the inflammatory response. Anywhere from the initiating cellular response to potentiating cellular and extracellular activity the clinician has to potential to intervene and modify acute inflammation.
Chronic inflammatory response is more challenging to describe, assess and manage. Inherent to the definition is prolonged duration of response. This response can result from sustained tissue insult, failed resolution of the acute inflammation or hypersensitivity immune response. Chronic inflammation often demonstrates slow onset with a persistent cyclical tissue destruction and repair (Figure 4).
Figure 4
In summary, inflammation is intended to protect and repair the body. Acute inflammation is short in duration of rapid response and less challenging to describe and manage to resolution. Chronic inflammation is of longer time course, sometimes indefinite, with definite resolution frequently difficult to achieve and identify. Often seen as the adversary, inflammation can be inappropriately or improperly attacked by the clinician. This can be minimized by always remembering the purpose of the inflammatory response and tenaciously seeking out its cause and mechanism before and during intervention.
Inflammatory intervention involves more than systemic anti-inflammatory pharmaceuticals, but this course is not prepared to address the full scope of the topic. In the larger picture anti-infectives play a critical role in treatment of inflammation, as does surgery, restricted activity, cryotherapy, etc.
Before the clinician initiates anti-inflammatory drug therapy they must aggressively search for the etiology of the inflammation. Included in the discovery is a comprehensive health and medication history. This is important to diagnosis as well as intervention. The cliniciaeeds to consider the impact of the modes of administration, sites of action and mechanisms of pharmaceutical neutralization and elimination. Gastro-intestinal health and action are uniquely important to the administration of oral anti-inflammatories. Some anti-inflammatories have erosive, anti-coagulative effects on gastrointestinal lining. Casually prescribed they can lead to serious adverse events such as ulceration and hemorrhage. Hepatic and renal function impact drug metabolism and elimination. The kidney is the primary organ of elimination for drugs, while the liver is the primary organ to metabolize drugs prior to elimination. The kidney is dependent on prostaglandins for normal function, therefore drugs that interfere with prostaglandin activity can significantly impact kidney function. The kidney’s adrenal medulla provides the body vital glucocorticoids that can be critically impacted by administration of exogenous corticosteroids like prednisone. In addition to GI, hepatic and renal health, pulmonary and cardiovascular systems also impact and are impacted by anti-inflammatory drug activity.
When prescribing medication for the old, the young, the fat, the thin and the medically complex the clinician must pay increasing attention to the history of present illness (HPI) and personal health history (PHHx). If you question the suitability of a non-inflammatory medication in the context of the patients’s HPI and PHHx consider consultation with the patient’s primary healthcare provider. If you question a failure of treatment reconsider the working diagnosis and query for the primary cause of treatment failure, non-compliance.
In general, anti-inflammatory interventions are greatest the earlier they act in they in the inflammatory cascades (Figure 5).
Figure 5
Commonly prescribed systemic anti-inflammatory medications are divided into groups: Salicylate non-steroidals and non-steroidals (NSAIDs), glucocorticoids (steroidals), antihistamines and anti-rheumatics (DMARDs).
Salicylates:
In general salicylates are rapidly absorbed and distributed following oral ingestion. They are extensively bound to plasma protein and commonly reach peak blood concentration in one to two hours. They are metabolized in the liver and excreted by the kidney. This class of anti-inflammatories can be formulated as a pro-drug. A pro-drug is an agent that is converted by the body into a metabolite drug which then imparts the desired therapeutic effects. Salicylate pro-drugs are hydrolyzed in minutes to a few hours, while the half life of most salicylates is 6 to 20 hours. Eliminating the action of salicylates can require days to several weeks of “washout”. Salicylates act both locally, modulating the effects of the inflammatory cascades and centrally suppressing the pain pathway. One Of the known mechanisms of action is prostaglandin inhibition by irreversible acetylation of the cyclo-oxygenase enzyme.
Aspirin (acetylsalicylate) is used for both acute and chronic intervention. Common dosage for acute inflammation is 325mg to 650mg every four hours not to exceed 4g/day. Generally aspirin is not used for pediatric application, do to the risk of inciting Reyes Syndrome. Aspirin is metabolized in the gut, blood plasma and liver, with a half-life of 15 to 120 minutes. Its’ metabolites are excreted in the urine.
Coated 325mg aspirin
Chronic low dose aspirin (81mg daily) is used for its’ platelet inhibitory effects to promote cardiovascular health. Coated aspirin slows absorption decreasing the onset of therapeutic benefit, while reducing the adverse effects to the gut. If rapid response is indicated coated aspirin should be avoided.
Low dose 81mg coated aspirin
Dolobid (diflunisal) is a long acting salicylate with a half life of 8 to 12 hours. It is metabolized by the liver and excreted in both the feces and urine. Usual dosing is 250mg to 500mg taken by mouth every 12 hours not to exceed 1500mg/day. Dolobid exhibits all the actions of other salicylates though there are aspects of the mechanism of action that are still unknown. A major effect of Dolobid to inhibition of prostaglandins.
Like any pharmaceuticals, salicylates’ can produce adverse drug reactions (ADR). Allergy to these agents can be life threatening. Some asthmatics can be aggravated by salicylates. Patients with severe pulmonary disease may have respiratory difficulty due to the added load salicylates place on respiration. Salicylates are additive with steroids, NSAIDs and anticoagulants. Patients with a history of gastro-intestinal bleeding are at risk for hemorrhagic events.
Ophthalmic indications for salicylates most commonly exploit the anti-platelet effects of the class. Amarosis Fugax, diabetic retinopathy and retinal vascular occlusions are conditions most commonly prompting prescription of salicylates.
Non-steroidal anti-inflammatory drugs include several sub-classes and a large number of agents. All classes have some degree of anti-inflammatory, anti-pyretic and analgesic effect. There are seven sub-classes fenamates (eg. Ponstel), indoles (eg. Indocin), pyrazolones (eg. Butazolidin), proprionates(eg. Advil), Phenylacetates (eg. Voltaren), oxicams (eg. Feldene). NSAIDs turn down the cyclooxygenase “valve”, reducing the production of prostaglandins and thrombaxanes. There are two physiological pathways that require cyclooxygenase (Figure 6). One, the COX-1 pathway, is primarily responsible for facilitating and modulating “housekeeping” activities carried out by the body. These actions involve normal renal function, gastric protection, platelet production, to name a few. The other pathway, COX-2, is primarily involved with inflammatory response producing and mediating prostaglandin activities, some of which produce pain, heat and swelling.
Figure 6
In general orally administered NSAIDs are rapidly absorbed and distributed, being extensively bound to plasma protein. Peak blood concentration is reached one to two hours following ingestion. NSAIDs are metabolized by the liver and excreted by the kidney. The half life is a couple of hours to a couple of days. NSAIDs can produce a number of systemic adverse reactions. Such responses include nausea, cramping, gastrointestinal ulceration, perforation and hemorrhage. Some recipients may develop allergic reactions, including asthma and dermatitis. NSAIDs will reduce blood clotting, but not to the degree that aspirin does. Renal and cardiac function can also be adversely affected by this class of anti-inflammatory agents. Prescibing NSAIDs for patients with GI, cardiovascular, renal or hepatic conditions must be done with added caution.
The selective COX-2 inhibitors have been implicated in cardic complications. The mechanism of action contributing to these events is still uncertain. Two popular theories are imbalance in COX activity leading to platelet aggregation and vasoconstriction, and elevated blood pressure secondary to sodium retention causing vasoconstriction. From the published studies reviewed these events have overwhelmingly been connected with chronic treatment with oral COX 2 inhibitors. It is unlikely that a short course of these medications, in a properly screened patient, would produce a clinically significant increased risk for myocardial infarction.
There are several ocular indications for oral NSAID therapy are: recalcitrant episcleritis, recalcitrant uveitis, recalcitrant cystoid macular edema and scleritis. An example of dosing for episcleritis would be 250 mg to 500 mg of Naproxen bid to tid. An example of dosing for diffuse and nodular scleritis would be Indomethacin 25 mg to 50 mg tid.
Corticosteroid anti-inflammatory medications exploit the studies of the adrenal gland by Addison and Brown-Sequard from the 1800s. They studied the role of adrenal glands in regulating body function, and in the early 1900s several hormones termed glucocorticoids and mineralocorticoids were isolated from the cortex of the adrenal gland.
Soon thereafter followed the discovery of the link between the adrenal glands, the pituitary gland (responsible for secreting adrenocorticotropic hormone (ACTH), which stimulates adrenal cortex corticosteroid production), and the hypothalamus (responsible for secreting corticotropin-releasing factor (CRF), which stimulates pituitary ACTH production). The hypothalamus, in turn, secretes more CRF in response to neural excitatory stimuli and reduced plasma corticosteroid concentration. This increases pituitary ACTH production which ultimately increases adrenal cortex corticosteroid production. This interdependent feedback mechanism is termed the H-P-A axis (Figure 7).
Figure 7
Iormal individuals, the adrenal cortex secretes about 25mg of cortisol (hydrocortisone) and 5 mg corticosterone per day. Only about 5% of these steroids are biologically active, the remainder being bound to plasma protein. Naturally occurring corticosteroid hormones are critical to normal physiologic function. Exogenous corticosteroid anti-inflammatory agents (steroids) mimic the action of naturally produced adrenocorticoid hormones, produced by the adrenal cortex. Corticosteroid drugs impart their effects by entering cells, binding with cytoplasmic receptors, which then transport the complexes into the cell’s nucleus. In the nucleus protein production is modified up-regulating production of anti-inflammatory proteins. These proteins, in part, inhibit phospholipase A2 which impairs the production of Arachodonic acid the primary precursor to eicosanoid production (Figure 8).
Figure 8
By inhibiting Arachodonate production the inflammatory cascades are inhibited very early in their path of activity, and thereby inflammation powerfully inhibited.
In equally powerful ways corticosteroid agents will up-regulate a number of other physiological mechanisms, which can lead to undesirable adverse effects from this drug class. The prescriber must always be cognizant of the possible adverse effects of hypertension, hyperglycemia, congestive heart failure, psychosis, mood shifts, insomnia, allergy, osteoporosis, nausea/vomiting, appetite suppression, peptic ulceration, papilledema, impaired growth & healing, fat redistribution, muscle atrophy and promotion of infection.
The need for systemic steroids in the management of ophthalmic conditions is uncommon, but when indicated remarkably effective in minimizing sequelae. In general systemic steroids are indicated when topical and/or injectable delivery is not appropriate or sufficient to achieve desired therapeutic effect. Systemic steroids are also indicated when the ophthalmic condition is part of a more disseminated disease process requiring steroid treatment.
Ophthalmic conditions warranting systemic corticosteroid therapy:
- Acute ocular allergic response, which is severe or recalcitrant to topical therapy
- Anterior uveitis not adequately responding to topical anti-inflammatories
- Scleritis
- Corneal graft rejection
- Posterior Uveitis
- Chorioretinitis
- Arteritic ischemic optic neuropathy
- Non-infectious optic neuritis
- MS neuritis IV methylprednisilone followed by oral prednisone
- Sarcoid optic neuritis
- Zoster optic neuritis
- Grave’s orbitopathy threatening compressive optic neuropathy
- Orbital pseudotumor
- Pseudotumor cerebri
Common agents and dosing for acute ophthalmic intervention:
Prednisone
Adult up to 120 mg PO QD
Child 0.05 to 2 mg/kg/day PO
Dexamethasone
Adult up to 9 mg PO QD
Child up to 0.3 mg/kg/day PO
Injection – 4 mg/cc up to 0.5 cc SCI
Triamcinalone (Kenalog)
Adult up to 50 mg QD
Child not advised for under age 12 years
Injection – 40 mg/cc up to 0.5 cc SCI
Methylprednisilone Dosepak (Medrol Dosepak)
Adult: Presorted system of 4 mg tablets. 24 mg of drug are taken day one, reducing dose by 4 mg each day until the pack is completed.
Nasal inhaler
Flonase & Beconase
2 sprays/nostril/day
Typical systemic corticosteroid adult dosing for ophthalmic conditions: Arteritic ischemic optic neuropathy 1000 mg IV methylprednisilone per day x 3 days or 60 mg to 100 mg oral prednisone daily tapering based on response to therapy. Highly suspect orbital pseudotumor is treated with 60 mg to 100 mg oral predisone and tapered based on clinical course. Dramatic and rapid response of orbitopathy is strongly supportive of the working diagnosis. Graves orbitopathy is less uniformly responsive to oral prednisone. Maximum therapeutic benefit of 80 mg to 100 mg oral prednisone daily should be achieved in 2 weeks or less. Prompt taper of prednisone should begin, at the latest, two weeks into treatment. Severe type I allergic blepharoconjunctivitis usually responds rapidly to treatment with a Medrol dosepak (24 mg down to 4 mg over 6 days).
DMARDs (anti-rhematics) and immunosuppressive agents are not covered in this course.
Allergy Management: Antihistamines Plus
Allergic immune response presenting to the ophthalmic practice can vary in manifestation and needed management. Linguistically, allergy is derived from two roots, allos, meaning other, and ergon, meaning action. The term was “coined” by pediatrician Clemensv Piquet in 1906. Physiologically, allergy is an exaggerated response of the immune system to substances recognized by the body, as foreign (immune hypersensitivity). This response is frequently characterized by inflammation.
There are four classic categories of immune hypersensitivity/allergy:
- Type I Immediate, anaphylactic
- Type II Cytotoxic
- Type III Immune complex
- Type IV Delayed, cell mediated
Immediate hypersensitivity is most common of the classes. It is manifest when and inciting agent (allergen) adheres to a pair of IgE immunoglobulins, antibodies produced by the body’s immune system. These antibodies are surface bound to a mast cell or basophil triggering degranulation and release of histamine, the primary mediator of type I allergy (Figure 9).
Figure 9
Histamine is found in high concentration in the “linings” & “coverings” of the body; stomach, duodenum, bronchial & nasal mucosa, conjunctiva & episclera and skin. Histamine binds with three receptor types. H1 receptors are concentrated in smooth muscle of the bronchi, blood vessels and intestinal mucosa. H2 receptors are primarily found on gastric parietal cells, cardiac tissue, pulmonary vessels and immune cells. H3 receptors have been recently described, with ocular implication yet to be put forth. Histamine’s effects include vasodilation of pre-capillary vessels, capillary dilation and increased permeability, vasoconstriction of post-capillary venules, direct action on immune cells. All of these actions contribute to characteristic inflammatory signs and symptoms of skin flushing, edema and pruritis (itching). Histamine also effects change in cardiac function reducing blood pressure, increasing heart rate and strength of contraction. Pulmonary action of Histamine is dualistic with H1 receptors producing bronchiol constriction and H2 receptors producing bronchiol relaxation. In the gut histamine increases gastric acid production while neurologically it mimics cholinergic agents like pilocarpine.
Allergens commonly causing type I response are airborne antigens (pollen, mold spore and dust), insect venom, foods(nuts) and drugs (penicillin, sulfa, aspirin, heparin, insulin). Ocular manifestation of type I allergy includes lid edema (angioedema), pruritis (itching), tearing, conjunctival chemosis and papillary reaction. Commonly such a case presents as allergic blepharoconjunctivitis. Systemic manifestation of type I allergy includes disseminated angioedema and pitting edema, erythema of the skin, prutitis, urticaria (infiltration of the skin), bronchoconstriction, generalized vasodilation and increased permeability, cardiac hypotension and dysrythmia.
Intervention for type I ophthalmic disease involves prompt and proper etiological diagnosis (diagnosis of cause). Once type I hypersensitivity is determined to be part, or all of the cause, the allergen should be identified and exposure reduced or preferably eliminated. Pharmaceutical treatment is aimed at reducing or eliminating the signs and symptoms arising from exposure to the allergen.
Systemic drug therapy for type I allergy is indicated when local topical medications are inadequate for the severity of response and or insufficient to keep signs and symptoms suppressed. Systemic pharmaceutical intervention is commonly directed at interference with the action of the primary mediator of type 1 allergy, histamine. Drugs that compete for histamine receptors are referred to as antihistamines. This class of pharmaceuticals competes with histamine for receptor binding sites, but does not actively displace receptor bound histamine. For this reason antihistamines do little to impact the manifest reaction, but rather they inhibit ongoing histamine binding thereby suppressing continued allergic stimulation. Over dose with antihistamines can produce toxicity. Antihistaminic toxicity may appear similar to adverse reaction to anticholinergic agents (Hypertension, tachycardia, urinary retention, constipation, dermal flush and “fever”, xerosis, delirium). Ophthalmic effects of systemic antihistamine include mydriasis, reduced accommodation and reduced lacrimation.
First generation antihistamines are commonly called sedating antihistamines. These agents effect sedation when they cross the blood brain barrier and bind with H1 receptors in the brain. For this reason the type 1 allergy inhibition is not possible without some degree of concurrent sedation. This may or may not be desireable. First generation antihistamines include diphenhydramine (Benedryl), chlorpheniramine (Chlor-trimeton) and Brompheniramine (Dimetapp). Most first generation antihistamines are available with out prescription.
Second and third generation antihistamines have been engineered with reduction of the sedation effect as a priority. Their molecular structures greatly impair the ability of the drugs to cross the blood brain barrier to bind CNS H1 receptors.
Common dosing for sedating antihistamines is as follows:
- First generation sedating antihistamines
- Diphenhydramine (Benedryl)
- Adult: 25 – 50mg po q 4-6h, 12.5/5ml IV or IM
- Maximum 300mg/24h
- Child: half adult dose
- Brompheniramine (Dimetapp)
- Adult: 4mg po q 4-6h, 2mg/5ml IV, IM or SC
- Child: half adult dosing down to age 6 years
- Chlorpheniramine (Chlor-trimeton)
- See Brompheniramine
- Sustained release adult: 8mg po q12h
Common dosing for non-sedating antihistamines is as follows:
- Second generatioon-sedating antihistamines
(Newer, more expensive, larger molecule impaired blood brain diffusion)
- Loratadine (Claritin)
- Adult: 10 mg po qd
- Child: half adult dosing down to age 2 years
- Cetirizine (Zyrtec)
- Adult: 5 – 10 mg po qd
- Child: half adult dose down to 6 years, quarter dose to 6 months
- Third generatioon-sedating antihistamines
(Newer, more expensive, metabolites of second generation)
- Fenofexadine (Allegra, Allegra D)
- Adult: 60 mg po q12h
- Child: half adult dose down to 6 years, quarter dose to 6 months
- Desloratadine (Clarinex)
- Adult: 5 mg po qd
- Child: half adult dosing down to age 5 years, 1/5 dose to 6 months
- Levocetirizine (Xyzal) recent FDA approval
- Adults: 5 mg po qd
- Child: half adult dosing down to age 6 years
NSAIDs may also be employed in the management of type I ocular allergy. NSAID inhibition of prostaglandins reduces mast cell release of histamine, as well other COX pathway mediators of inflammation. NSAIDs are able to actively interfere with mast cell and basophile degranualation, in opposition to the action of histamine and thereby accelerate resolution of inflammatory signs produced by the offending allergens.
Steroidal drugs are the most effective at reducing the inflammatory signs of type I allergy. However, as presented earlier, the impressive non-specific anti-inflammatory effects of steroids, come with a much larger “bag” of adverse effects. For this reason prescription of systemic steroidal agents demands an adequate medical history. Short course tapered treatment is desirable when used for treatment of type I allergy (eg. Medrol dosepak).
Type II hypersensitivity (cytotoxic reaction) manifests when the triggering antigen is bound to a cell which then binds antibodies IgG or IgM triggering the complement inflammatory cascade. This leads to lysis (rupture) of the targeted cell, thus the term cytotoxic hypesensitivity. Examples of type II hypersensitivity are graft early graft rejection, drug induced hemolytic anemia and “autoimmune” diseases such as Graves and Myasthenia. In type II response IgE (the type I allegy immunoglobulin) is not the mediating immunoglobulin, therefore histamine is not the dominant mediator of the reaction. For this reason antihistamines of little if any practical benefit in managing type II disease.
Initial intervention for cytotoxic disease usually involves steroidal agents. Corneal transplant rejection is most often treated topically or with injection as follows:
- Primary management, high dose topical prednisilone acetate 1%
- Loading dose 5 – 10 drops first hour
- 1 – 2 drops every 15 minutes first half day then q1h
- May require drops during sleep first 72 hours
- Supplemental management
- Subconjunctival triamcinilone injection
- 0.1 to 0.5 cc SCI
Acute Grave’s ophthalmopathy if needed is treated systemically as follows:
- High dose IV methyl prednisolone and/or oral prednisone
- 250 mg every 6 hours of IV methyl prednisolone
- Converted to oral steroid based on clinical course
- 80 mg to 100 mg per day of oral prednisone and tapered per clinical course
- Many clinicians reserve steroid intervention for cases threatening the optic nerve
Type III hypersensitivity (immune complex reaction) presents when antigen binds to blood cell immunoglobulin (IgG, IgM) complex, which then migrates to tissue, there triggering the complement cascade producing inflammation. Examples of immune complex disease are serum sickness, rheumatoid arthritis and systemic lupus. Rheumatoid disease and lupus are known for ophthalmic manifestations of scleritis and varied chorioretinitis. Like type II disease high dose systemic steroids are often indicated, as are some NSAIDs. Patients with ocular manifestations of type III and frequently type II hypersensitivity are often managed or comanaged with subspecialist in immunology of ocular and systemic disease.
Type IV hypersensitivity (delayed allergy, cell mediated response) occurs when antigen attaches to macrophages or dendritic cells. These antigen presenting cells (APC) sensitize T lymphocytes leading to production and release of lymphokines which mediate the immune/allergic response. Type IV hypersensitivity requires prolonged exposure to the antigens to produce T cell sensitization and resulting inflammatory response. Examples of type IV ocular allergy are ophthalmic drug induced blepharoconjunctivitis (eg. Brimonidine, atropine), contact dermatoblepharitis (make up exposure), chronic corneal graft rejection.
Like type I allergy intervention for type IV ocular allergy is initially directed at identification and elimination of the offending antigen/allergen. Ocular medications, skin preparations and occupational chemicals are common culprits. The next step is suppression of the immune response. In mild manifestations, removal of the antigen with or without supportive therapy (hydration, lubrication) is frequently sufficient. Moderate cases will frequently justify topical anti-inflammatory treatment, while severe presentation may warrant oral non-steroidal or steroidal treatment.
Pain Management: Analegsics
One of the cardinal signs of inflammation is pain, though pain can present without inflammation. Pain is “an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such” (Merskey, 1986). Pain is classified in several ways. Location of pain stimulus, central vs peripheral, is one way of classification. An example of central pain would be pain resulting from an intracranial tumor. Peripheral pain would result from a broken bone or torn ligament. Pain is also classified by the status of the neural tissue involved in the pain sensation. Nociceptive pain results wheeural tissue responds normally to tissue insult. Neuropathic pain results from adaptation and abnormal function pain receptors subsequent to tissue insult. Finally, pain is classified as acute or chronic/persistent a distinction which greatly influences the impact of pain on daily living, as well as management thereof.
- Mechanisms
- “The reign of pain is mainly in the brain” yet peripheral tissue insult is frequently the trigger for neural activity which produces pain
A review of the neural pathways of pain (Figure 10) is fundamental to the use of analgesics for management. The afferent pathways can be divided into peripheral and central. The basic pain receptor is the nociceptor. These receptors are numerous and widely distributed throughout the body. They are innervated by C fiber neurons which synapse in the dorsal horn of the spinal cord or midbrain. Nociceptors are up regulated by thromboxanes, prostaglandins, leukotrienes. Up regulation of the peripheral pathway is referred to as peripheral sensitization. Pain sensation is reported when the peripheral afferent pathway achieve “wind up”, which occurs wheociceptor stimulation exceeds an impulse frequency of 1 per 3 seconds. At this rate, or higher, the central pathway threshold is exceeded and substance P is up regulated forwarding the pain signal toward the brain. The central pathway begins at the synapse with the peripheral C fibers in the dorsal horn of the cord (the origin of the spinothalamic tracts) or midbrain (spinocerebral tracts). The spinocerebral tracts have been subclassified based on anatomy and correlated pain perception. The spinothalmic tract relays stimulation producing discriminate pain. The spinoreticular tract transmits signal relative to suffering pain. Gut pain is transmitted by the dorsal column, while the spinohypothalamic tract forwards neural signaling from cornea, lips, tongue, genitals and GI tract.
The efferent pathways of pain perception are feedback/afferent modulating tracts. Many cortical and subcortical centers are convergently connected with the cord’s dorsal horn providing feedback, modulating afferent transmission. Persistent pain stimuli trigger physiological changes in the efferent pathway converting persistent acute pain stimulation to chronic pain.
Schematic showing the afferent and efferent pathways of pain Figure 10
Ocular conditions producing pain are numerous, but do have some differentiating characteristics helpful to management. The following ophthalmic conditions are no where near exhaustive, but provide examples of the more common and familiar conditions presenting to the ophthalmic practice.
Ocular trauma can be blunt, abrasive, lacerative or perforating. Abrasive pain is described as lancinating, sharp or stabbing, aggravated by relative lid globe movement. Lacerative injury produces pain similar in quality to abrasion though it is more variable and usually less intense. Perforating trauma in pure presentation can be mildly painful to painless. If there is an abrasive or lacerative component the pain report will increase. Blunt ocular trauma frequently produces a deep pulsatial pain, which varies from debilitating to annoying. Pain from acute ocular trauma begins with the mechanical tissue insult stimulating nociceptors. If the tissue insult is sufficient to produce pain producing inflammation the severity of the pain response generally increases. As tissue repair proceeds feedback will modulate both the inflammatory response and the associated pain perception. Pain sensation and the course of it’s quality and severity are extremely helpful in the management of ocular trauma, as well as other pain producing ocular disease.
Pain producing ocular infections most frequently presenting to the optometric clinician are preseptal cellulitis, and keratitis. Some less common pain producing ocular infections are dacriocystitis, severe viral keratoconjunctivitis and orbital cellulitis. As with traumatic pain the quality and severity of the clinical course are quite helpful to management. In general fungal and parasitic keratitis produce a disproportionate pain sensation relative to the clinical signs while viral keratitis can look “nasty” and deserving of a stronger pain report. In general more virulent organisms produce greater inflammation which correlates with a stronger pain report. If intervention involves anti-inflammatory and or analgesic intervention the pain response may be iatrogenically (clinician caused) down regulated, while the infecting organism may continue to thrive. In the setting of anti-infective therapy only pain reduction is nearly always an indication of movement toward resolution and restoration of tissue health.
“Non-infectious” non-traumatic ocular conditions producing pain include orbital cellulitis, of Grave’s disease and orbital pseudotumor, uveitis, optic neuritis, scleritis and acute angle closure glaucoma. Non-infectious is placed in quotes as some of these conditions may result from infective agents yet undiscovered, or from past infectious states since converted to non-infectious immune responses. This group of pain producing ophthalmic conditions primarily produces pain out of the inflammatory process, the exception being acute angle closure glaucoma. When the stimulus for inflammation is determined to be non-infectious the clinician can more comfortably prescribe anti-inflammatory and analgesic medication to facilitate the return of normal function and resolution of inflammation and associated pain.
- Treating ocular pain can be effectively approached with a similar strategy to that used to manage allergy
- Take a complete medical and drug Hx
- Aggressively seek out underlying cause
- First Rx treatment to neutralize and eliminate underlying agent or causative process
- Next consider case appropriate anti-inflammatory therapy
- Primarily peripheral therapeusis
- Last institute non-anti-inflammatory analgesia
- Primarily central therapeusis
- God intended pain to protect us, so use a comprehensive approach to intervention
In ophthalmic pain management supportive therapy is more valuable than often given credit for. Lubrication, cold compress, cycloplegia, protective lenses (tinted and wet chamber), bandage contact lenses are measures that can be very beneficial to pain management. With supportive therapy properly employed pharmaceutical intervention can be appropriately administered and prescribed. Be vigilant for adverse drug responses and conditions that facilitate such responses. Specifically be alert for aspirin allergy, which is more common in asthmatics. Use caution when using Acetaminophen in patients with hepatic dysfunction. Prostaglandin inhibitors like Ibuprofen can seriously compromise renal function in patients with kidney disease. Narcotics are addictive, impair cognitive function, will slow gastrointestinal and urinary activity (constipation and urinary retention), depress respiration.
Patients with compromised pulmonary, cardiac, renal and hepatic function are at greater risk with the use of systemic medications. Remember that analgesics can mask symptoms of infection.
Common agents and dosing for ophthalmic pain:
Aspirin aka ASA (Bayer, Ecotrin) 325 mg to 650 mg every 4 to 6 hours, not to exceed 4000 mg per day. Toxicity is heralded by tinitis from neurotoxicity of CN VIII. Aspirin produces analgesia by blocking prostaglandin synthesis. It exhibits “ceiling effect” (point at which increasing dose adds no additional analgesic effect). Aspirin’s platelet inhibition reduces clotting and can complicate gastric hemorrhage triggered by prostaglandin inhibition (stomach lining rich source of prostaglandins).
Acetaminophen aka APAP (Tylenol) 325 mg – 650 mg every 4 to 6 hours. Mechanism of action is unknown, but thought to be central acting by blocking generation of pain impulses in the CNS. Acetaminophen has no known anti-inflammatory effect. It does not inhibit blood clotting or produce GI ulceration, but can produce liver toxicity with overdose or use with alcohol. Tylenol is a pregnancy category B drug and considered safe for use in pregnancy.
Ibuprofen (Advil, Motrin) 200 mg to 400 mg every 4 to 6 hours not to exceed 3200 mg per day. Naproxen (Aleve) is another NSAID that has analgesic benefit. Initial dosing is 400 mg followed by 200 mg every 8 to 12 hours.
Codiene in Tylenol #1, 2, 3 & 4 and Empirin #3 & 4 varies in dose from 7.5 mg to 60 mg of codeine per dose. Tylenol #3 couples 300 mg of acetaminophen with 30 mg of codeine. Empirin #3 combines 325 mg of aspirin with 30 mg of codeine. This combined analgesics are classified as schedule III controlled substances.
Hydrocodone in Lortab, Vicodin and Vicoprofen vary in dose from 2.5 mg to 10 mg of hydrocodone. Loratab couples 500 mg of acetaminophen with 2.5 to 10 mg of hydrocodone. Vicodin couples 500 mg of acetaminophen with 5 mg of hydrocodone. Vicoprofen combines 200 mg of Ibuprofen with 7.5 mg of hydrocodone. Like the codeine combination drugs the hydrocodone combos are schedule III controlled substances.
100 mg of Propoxyphene is found in Darvocet N-100 combined with 650 mg of Acetaminophen. Do not prescribe for patients diagnosed with depression on suicidal ideation. Propoxyphene is highly addictive. In it’s combination formulation it is a schedule IV controlled substance.
Prescribing controlled substance analgesics requires additional caution and attention to regulation. The following outlines information to know in safely and effectively prescribing these agents:
Controlled substances
- Prescribing practices
- Non-topical pharmaceutical certification for your state of practice
- DEA licensure & number
- Complete written prescription
- Patient Name
- Date
- Medication
- Quantity: numeric and alphabetic
- Dosage: numeric and alphabetic direction
- Frequency
- Special instruction
- Doctor name, location and signature
- Counsel on adverse effects
Controlled substance class and definition
- I – High abuse potential, no accepted medical use
- heroin, marijuana, LSD, illegal substances
- II – High abuse potential with severe dependence liability
- morphine, oxycodone, codeine, cocaine, meperidine, amphetamines, barbiturates
- III – Less abuse potential than schedule II and moderate dependence liability
- codeine and hydrocodone combinations (Tylenol with codeine, Vicodin, etc.)
- IV – Less abuse potential than schedule III and limited dependence liability
- propoxyphene, benzodiazepines (Valium, Xanax)
- V – Limited abuse potential
- codeine cough syrups, antidiarrheals
Neurontin (Gabapentin) is a non-narcotic analgesic used in treatment of post Zoster neuralgia. Dosing is 300 mg to 600 mg three times daily titrating low to high with a maximum acceptable dose of 3600 mg/day. Dosing needs to be adjusted for renal function. This is a good agent to comanage with the patient’s PCP.
Anxiety Management: Anxiolytics
Anxiety is the sense of apprehension and or fear. Pain and the anticipation of pain is frequently a contributor to distressing and debilitating anxiety. Though I have been addressing physical pain, “psychological pain” is another common cause of anxiety. Ophthalmic conditions are quite effective in producing both types of pain. Ocular tissue insult or the anticipation thereof (surgery) and the possibility or actuality of sight loss is very effective in producing anxiety. Pharmaceutical agents that inhibit anxiety are referred to anxiolytics. Agents that produce anxiolysis often produce sedation and hypnosis when dosing quantity and or frequency are increased. Anxiolytics vary widely relative to their pharmacokinetics and pharmacodynamics.
Benzodiazepines (BZDs) are commonly prescribed for short term treatment of acute anxiety as well general anxiety disorder (GAD). BZDs or commonly used to prepare an individual for a medical proceudure. BZDs reduce anxiety and enhance anterograde amnesia. This class can also be used as a hypnotic (sleep induction), though close monitoring is mandatory. Prescribers must be prepared to reverse decompensation of vital functions if such occurs.
See table of BZDs showing brand names, typical and maximal dosing (Figure11)
Figure 11
BZD mechanism of action is to attach to GABA (gaba amino benzoic acid) receptors in the CNS. GABA is the major inhibitory neurotransmitter of the CNS. BZDs indirectly up regulate the effects of GABA resulting in increased firing of neurons. It is difficult to separate the pharmacological actions of BZDs. Along with axiolysis comes sedation and anterograde amnesia, and with higher doses hypnosis/sleep. In contrast, tricyclic antidepressants do not produce axiolysis. Though some BZDs can induce stage III anesthesia they are not a desirable agent for this purpose.
BZD are not exempt from adverse drug reactions (ADRs), though at therapeutic levels they are consider to have a favorable safety margin. Caution is necessary when prescribing for patients with pulmonary disease. Respiratory depression of the medullary respiratory center in such patients could produce arrest. Concurrent heart disease, such as congestive heart failure, can be additive to the risk for ADR. The prescribing clinician should carry heightened awareness for patients suffering from hepatic disease, pregnancy or is nursing (category D). Adverse drug interaction occurs most commonly when BZD are taken with alcohol.
Ophthalmic conditions for which anxiolytics can be useful are:
- Ophthalmic surgery
- Blepharoplas
- Cataract
- Refractive
- Corneal transplant & pterygium
- Glaucoma
- Vitreoretinal
- Ophthalmic procedures
- Periocular and intraocular injection
- Foreign body removal
- Nasolacrimal dilation & irrigation
- Scleral depression
- Ocular suture removal
- Pediatric examination
- Procedures for the psychologically fragile
What is Conjunctivitis (Pink Eye)?
Conjunctivitis is inflammation of the conjunctiva, the thin, filmy membrane that covers the white of your eye. The conjunctiva, which produces mucus to coat and lubricate the surface of the eye, contains fine blood vessels that can be seen on close inspection. When the conjunctiva becomes irritated or inflamed, the blood vessels, which supply it, enlarge and become more prominent, causing the eye to turn red.
- Pinkness or redness in the eye
- Red, inflamed inner eyelids
- Blurred vision
- Sandy or scratchy feeling in the eye
- Pus, mucous, or watery discharge from the eye
The symptoms described above may not necessarily mean that you have conjunctivitis. However, if you experience one or more of these symptoms, contact your ophthalmologist for a complete exam.
There are many sources of eye irritation that can cause conjunctivitis.
- Bacterial Conjunctivitis
Bacterial infections can cause a red eye, which is associated with pus or discharge from the eye, or they can cause a red eye which is associated with crusting of the eyelashes with little or no discharge. - Viral Conjunctivitis
Viruses can cause conjunctivitis, such as the familiar red eyes, sore throat, and runny nose of a common cold. Viral conjunctivitis usually produces a watery mucous discharge and lasts from 1 to 2 weeks. Infectious conjunctivitis, commonly known as “pink eye,” can be quite contagious. Cloth handkerchiefs and towels should not be shared during this time. Hand washing also will help prevent the spread of this infection. - Allergies
Allergies can cause conjunctivitis, which produces a stringy, white discharge. Allergies can make the eyes itchy or produce a chronic red eye and environmental irritants, such as smoke or fumes, may cause conjunctivitis. Any type of conjunctivitis is aggravated by dryness of the eyes.
The risk factors for conjunctivitis depend on the type of conjunctivitis. Bacterial conjunctivitis results from exposure to a bacterial organism to which the eye is vulnerable. Some of the more worrisome types of bacterial conjunctivitis can be caused by organisms that also cause sexually transmitted diseases; a sudden onset of the above symptoms in the context of a new sexual partner needs to be evaluated.
Viral conjunctivitis is extremely contagious. Often the person with viral conjunctivitis has had an upper respiratory infection preceding the onset of the red eye or has been around someone with an upper respiratory infection. People who work in health care settings or with children have a high risk of exposure to the viruses that can cause viral conjunctivitis.
Allergic conjunctivitis is caused by the environmental factors that trigger an allergic reaction in the eye and these triggers are different for each person.
The different types of conjunctivitis often can be distinguished by an eye examination, including your medical history. If your ophthalmologist suspects bacterial conjunctivitis, s/he will culture your eyelids, conjunctiva, and discharge to make a diagnosis and choose the best treatment. Viral and allergic conjunctivitis often do not require special testing for diagnosis.
If you think you might have conjunctivitis, you should
- Keep your hands away from your eyes
- Thoroughly wash your hands before and after applying eye medications
- Do not share towels, washcloths, cosmetics, or eyedrops with others
- Seek treatment promptly
- Small children, who may forget these precautions, should be kept away from school, camp, and the swimming pool until the condition is cured
Treatment for Bacterial or Viral Conjuntivitis
Infectious conjunctivitis, caused by bacteria, usually is treated with antibiotic eye drops and/or ointment. Other infectious forms, caused by viruses, can’t be treated with antibiotics. They must be fought off by your body’s immune system. But some antibiotics may be prescribed to prevent secondary bacterial infections from developing. Artificial tears and warm compresses may help keep the eye comfortable while viral conjunctivitis runs its course.
Treatment for Allergic Forms of Conjuntivitis
When treating allergic and chemical forms of conjunctivitis, the cause of the allergy or irritation must first be removed. For instance, avoid contact with any animal if it causes an allergic reaction. Wear swimming goggles if chlorinated water irritates your eyes. In cases where these measures won’t work, prescription and over-the-counter eye drops are available to help relieve the discomfort.

