Dental implantation
A dental implant is a “root” device, usually made of titanium, used in dentistry to support restorations that resemble a tooth or group of teeth to replace missing teeth.
Virtually all dental implants placed today are root-form endosseous implants, i.e., they appear similar to an actual tooth root (and thus possess a “root-form”) and are placed within the bone (endo- being the Greek prefix for “in” and osseous referring to “bone”). The bone of the jaw accepts and osseointegrates with the titanium post. Osseointegration refers to the fusion of the implant surface with the surrounding bone. Dental implants will fuse with bone, however they lack the periodontal ligament, so they will feel slightly different than natural teeth during chewing.

Prior to the advent of root-form endosseous implants, most implants were either blade endosseous implants, in that the shape of the metal piece placed within the bone resembled a flat blade, or subperiosteal implants, in which a framework was constructed to lie upon and was attached with screws to the exposed bone of the jaws.
Dental implants can be used to support a number of dental prostheses, including crowns, implant-supported bridges or dentures.[1] They can also be used as anchorage for orthodontic tooth movement. The use of dental implants permits undirectional tooth
History
The Maya civilization has been shown to have used the earliest known examples of endosseous implants (implants embedded into bone), dating back over 1,350 years before Per-Ingvar Brånemark started working with titanium. While excavating Maya burial sites in Honduras in 1931, archaeologists found a fragment of mandible of Maya origin, dating from about 600 AD. This mandible, which is considered to be that of a woman in her twenties, had three tooth-shaped pieces of shell placed into the sockets of three missing lower incisor teeth. For forty years the archaeological world considered that these shells were placed after death in a manner also observed by the ancient Egyptians. However, in
In the 1950s research was being conducted at Cambridge University in
Dr. Leonard Linkow placed his first dental implant in 1952, four months after he graduated from dental school. By 1992, Dr. Linkow had placed over 19,000 dental implants and stopped counting. He retired from private practice in 2002 leaving a body of work that included 12 books and 36 patents. Many implant dentists refer to Dr. Linkow as the father of modern implant dentistry.
Meanwhile an Italian medical doctor called Stefano Melchiade Tramonte, understood that titanium could be used for dental restorations and after designing a titanium screw to support his own dental prosthesis, started to use it on many patients in his clinic in 1959. The good results of his clinical studies on humans were published in 1966.[3]
Although Brånemark had originally considered that the first work should centre on knee and hip surgery, he finally decided that the mouth was more accessible for continued clinical observations and the high rate of edentulism in the general population offered more subjects for widespread study. He termed the clinically observed adherence of bone with titanium as ‘osseointegration’. In 1965 Brånemark, who was by then the Professor of Anatomy at Gothenburg University in Sweden, placed his first titanium dental implant into a human volunteer.
Contemporaneous independent research in the
Over the next fourteen years Brånemark published many studies on the use of titanium in dental implantology until in 1978 he entered into a commercial partnership with the Swedish defense company,
Some current research in dental implantology is focusing on the use of ceramic materials such as zirconia (ZrO2) in the manufacture of dental implants. Zirconia is the dioxide of zirconium, a metal close to titanium in the periodic table and with similar biocompatibility properties. Although generally the same shape as titanium implants, zirconia, which has been used successfully for orthopaedic surgery for a number of years, has the advantage of being more cosmetically aesthetic owing to its bright tooth-like colour. However, long-term clinical data is necessary before one-piece ZrO2 implants can be recommended for daily practice.
Composition
A typical implant consists of a titanium screw (resembling a tooth root) with a roughened or smooth surface. The majority of dental implants are made out of commercially pure titanium, which is available in 4 grades depending upon the amount of carbon and iron contained. More recently grade 5 titanium has increased in use. Grade 5 titanium, Titanium 6AL-4V, (signifying the Titanium alloy containing 6% Aluminium and 4% Vanadium alloy) is believed to offer similar osseointegration levels as commercially pure titanium. Ti- 6Al-4V alloy offers better tensile strength and fracture resistance. Today most implants are still made out of commercially pure titanium (grades 1 to 4) but some implant systems are fabricated out of the Ti-6Al-4V alloy. Implant surfaces may be modified by plasma spraying, anodizing, etching, or sandblasting to increase the surface area and osseointegration potential of the implant.
Training
There is no specialty recognized by the ADA for dental implants in the
The legal training requirements for dentists who carry out implant treatment differ from country to country. In the
The degree to which both graduate and post-graduate dentists receive training in the surgical placement of implants varies from country to country, but it seems likely that lack of formal training will lead to higher complication rates.
In the
Surgical procedure
Surgical planning
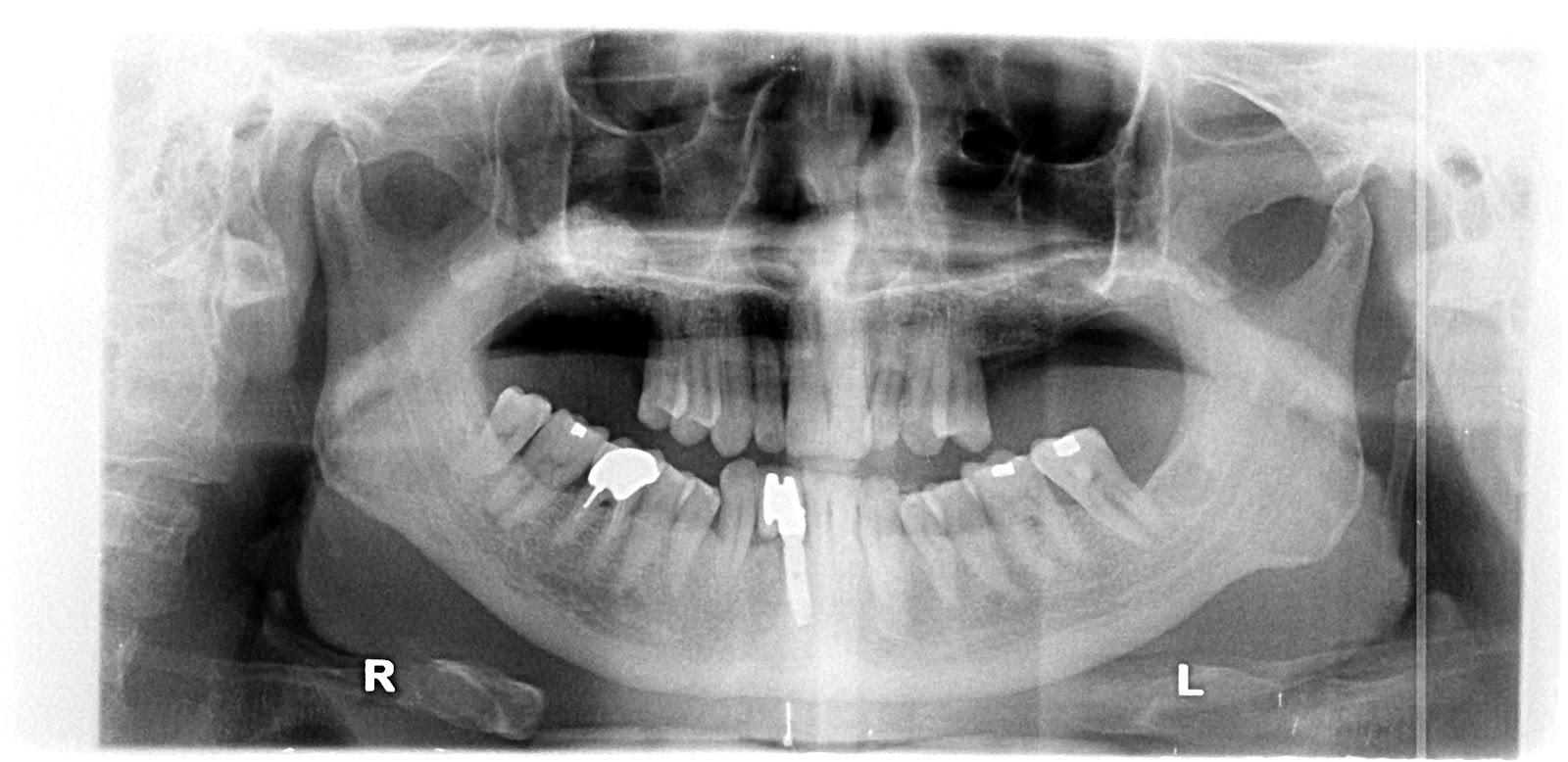
Prior to commencement of surgery, careful and detailed planning is required to identify vital structures such as the inferior alveolar nerve or the sinus, as well as the shape and dimensions of the bone to properly orient the implants for the most predictable outcome. Two-dimensional radiographs, such as orthopantomographs or periapicals are often taken prior to the surgery. Sometimes, a CT scan will also be obtained. Specialized 3D CAD/CAM computer programs may be used to plan the case.
Whether CT-guided or manual, a ‘stent’ may sometimes be used to facilitate the placement of implants. A surgical stent is an acrylic wafer that fits over either the teeth, the bone surface or the mucosa (when all the teeth are missing) with pre-drilled holes to show the position and angle of the implants to be placed. The surgical stent may be produced using stereolithography following computerized planning of a case from the CT scan. CT guided surgery may double the cost compared to more commonly accepted approaches.
Basic procedure
In its most basic form, the placement of an implant requires a preparation into the bone using either hand osteotomes or precision drills with highly regulated speed to prevent burning or pressure necrosis of the bone. After a variable amount of time to allow the bone to grow on to the surface of the implant (osseointegration), a crown or crowns can be placed on the implant. Unlike conventional dental implants, Mini dental implants may be loaded immediately and still have a high survival rate (94%). The amount of time required to place an implant will vary depending on the experience of the practitioner, the quality and quantity of the bone and the difficulty of the individual situation.
Detail procedure
At edentulous (without teeth) jaw sites, a pilot hole is bored into the recipient bone, taking care to avoid the vital structures (in particular the inferior alveolar nerve or IAN and the mental foramen within the mandible). Drilling into jawbone usually occurs in several separate steps. The pilot hole is expanded by using progressively wider drills (typically between three and seven successive drilling steps, depending on implant width and length). Care is takeot to damage the osteoblast or bone cells by overheating. A cooling saline or water spray keeps the temperature of the bone to below 47 degrees Celsius (approximately 117 degrees Fahrenheit). The implant screw can be self-tapping, and is screwed into place at a precise torque so as not to overload the surrounding bone (overloaded bone can die, a condition called osteonecrosis, which may lead to failure of the implant to fully integrate or bond with the jawbone). Typically in most implant systems, the osteotomy or drilled hole is about 1mm deeper than the implant being placed, due to the shape of the drill tip. Surgeons must take the added length into consideration when drilling in the vicinity of vital structures.
Surgical incisions
Straumann guide pin in place to visualize positioning, angulation and depth prior to implant placement. Implant is being placed as a flapless procedure because it was clinically and radiographically evident that there is adequate bone in all dimensions.
Traditionally, an incision is made over the crest of the site where the implant is to be placed. This is referred to as a ‘flap’. Some systems allow for ‘flapless’ surgery where a piece of mucosa is punched-out from over the implant site. Proponents of ‘flapless’ surgery believe that it decreases recovery time while its detractors believe it increases complication rates because the edge of bone cannot be visualized. Because of these visualization problems flapless surgery is often carried out using a surgical guide constructed following computerized 3D planning of a pre-operative CT scan.
Healing time
The amount of time required for an implant to become osseointegrated is a hotly debated topic. Consequently the amount of time that practitioners allow the implant to heal before placing a restoration on it varies widely. In general, practitioners allow 2–6 months for healing but preliminary studies show that early loading of implant may not increase early or long term complications. Minimally invasive methods of early dental implant placement reduce the cost of installed implants and shortens the implant-prosthetic rehabilitation time with 4–6 months. If the implant is loaded too soon, it is possible that the implant may move which results in failure. For conventional implants, the subsequent time to heal, possibly graft, and eventually place a new implant may take up to eighteen months. For this reason many are reluctant to push the envelope for healing.
One-stage, two-stage surgery
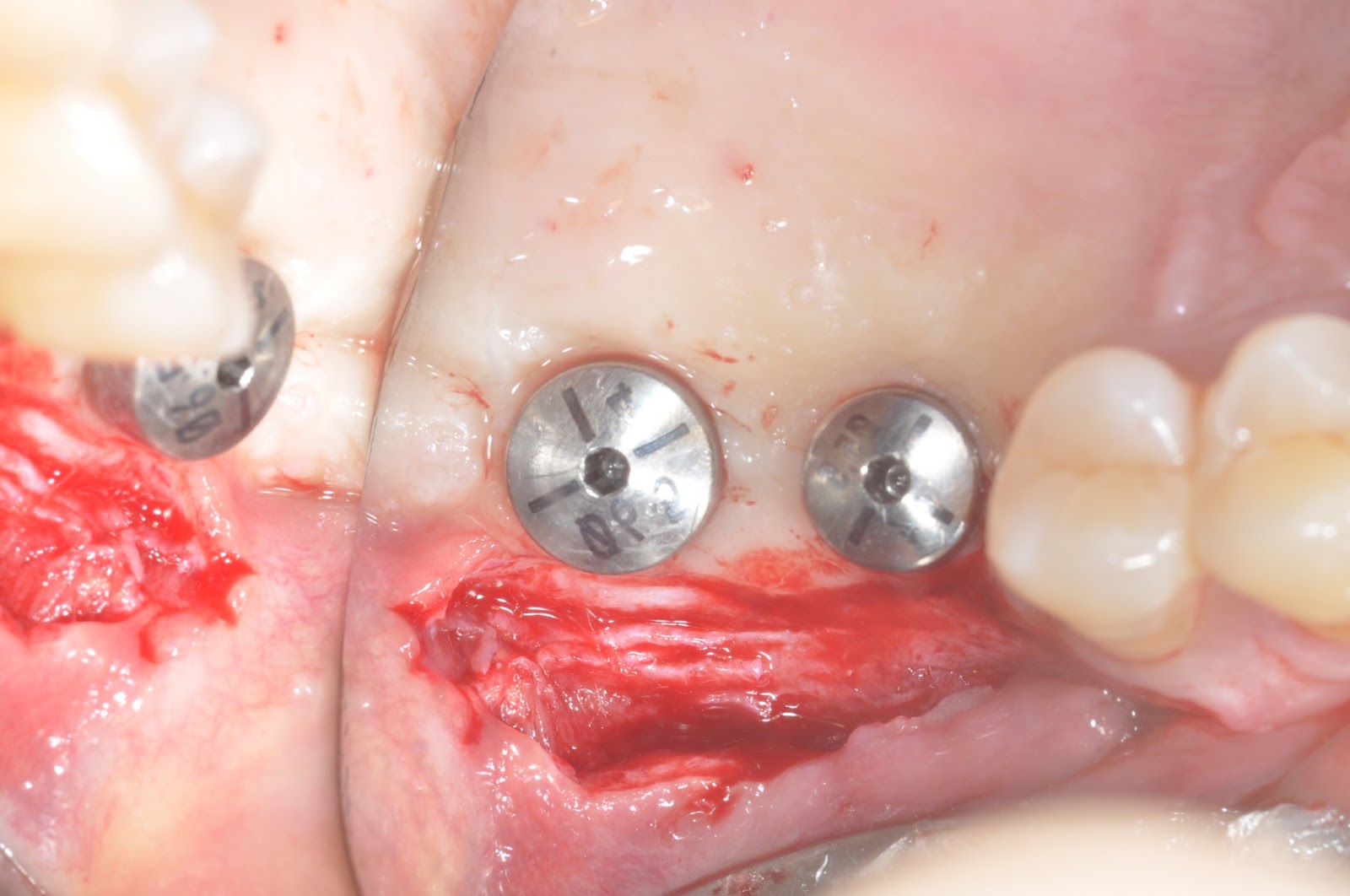
When an implant is placed either a ‘healing abutment’, which comes through the mucosa, is placed or a ‘cover screw’ which is flush with the surface of the dental implant is placed. When a cover screw is placed the mucosa covers the implant while it integrates then a second surgery is completed to place the healing abutment.
Two-stage surgery is sometimes chosen when a concurrent bone graft is placed or surgery on the mucosa may be required for esthetic reasons. The latter is usually important where an implant is placed in the “esthetic zone”. This allows more control over the healing and as a result the predictability of the final result[26]. Some implants are one piece so that no healing abutment is required.
In carefully selected cases, patients can be implanted and restored in a single surgery, in a procedure labeled “Immediate Loading”. In such cases a provisional prosthetic tooth or crown is shaped to avoid the force of the bite transferring to the implant while it integrates with the bone.
Surgical timing
There are different approaches to place dental implants after tooth extraction. The approaches are:
1. Immediate post-extraction implant placement.
2. Delayed immediate post-extraction implant placement (2 weeks to 3 months after extraction).
3. Late implantation (3 months or more after tooth extraction).
According to the timing of loading of dental implants, the procedure of loading could be classified into:
1. Immediate loading procedure.
2. Early loading (1 week to 12 weeks).
3. Delayed loading (over 3 months)
4.
Immediate placement
An increasingly common strategy to preserve bone and reduce treatment times includes the placement of a dental implant into a recent extraction site. In addition, immediate loading is becoming more common as success rates for this procedure are now acceptable. This can cut months off the treatment time and in some cases a prosthetic tooth can be attached to the implants at the same time as the surgery to place the dental implants. Because one of three implants requires a minimum addition of bone tissue, surgical techniques for underlying bone augmentation are currently under a large scale development.
Most data suggests that when placed into single rooted tooth sites with healthy bone and mucosa around them, the success rates are comparable to that of delayed procedures with no additional complications.
Teeth in a Day
“Teeth in a day”, “All-on-four”, “Fast and fixed” are similar surgical concepts whereby implants are placed on the same day and a fixed prosthesis is attached to them. This allows the patient to leave with a fixed solution as opposed having to make do with a removal temporary prosthesis whilst the implant osseointegrate with the bone. This concept is appropriate for completely edentulous jaws where either the teeth are to be extracted or have already been removed.
Use of CT scanning
CT scan of the lower jaw. This shows eight dental implants superimposed over the lower jaw in areas of maximum bone and four teeth that will be extracted.
When computed tomography or, more specifically, cone beam computed tomography or CBCT (3D X-ray imaging) is used preoperatively to accurately pinpoint vital structures including the inferior alveolar canal, the mental foramen, and the maxillary sinus, the chances of complications might be reduced as is chairtime and number of visits. Cone beam CT scanning, when compared to traditional medical CT scanning, utilizes less than 2% of the radiation, provides more accuracy in the area of interest, and is safer for the patient. CBCT allows the surgeon to create a surgical guide, which allows the surgeon to accurately angle the implant into the ideal space.
Complementary procedures
Sinus lifting is a common surgical intervention. A dentist or specialist with proper training such as an oral surgeon, periodontist, general dentist or prosthodontist, thickens the inadequate part of atrophic maxilla towards the sinus with the help of bone transplantation or bone expletive substance. This results in more volume for a better quality bone site for the implantation. Prudent clinicians who wish to avoid placement of implants into the sinus cavity pre-plan sinus lift surgery using the CBCT X-ray, as in the case of posterior mandibular implants discussed earlier.
Bone grafting will be necessary in cases where there is a lack of adequate maxillary or mandibular bone in terms of front to back (lip to tongue) depth or thickness; top to bottom height; and left to right width. Sufficient bone is needed in three dimensions to securely integrate with the root-like implant. Improved bone height—which is very difficult to achieve—is particularly important to assure ample anchorage of the implant’s root-like shape because it has to support the mechanical stress of chewing, just like a natural tooth.
Typically, implantologists try to place implants at least as deeply into bone as the crown or tooth will be above the bone. This is called a 1:1 crown to root ratio. This ratio establishes the target for bone grafting in most cases. If 1:1 or more cannot be achieved, the patient is usually advised that only a short implant can be placed and to not expect a long period of usability.
A wide range of grafting materials and substances may be used during the process of bone grafting / bone replacement. They include the patient’s own bone (autograft), which may be harvested from the hip (iliac crest) or from spare jawbone; processed bone from cadavers (allograft)Which is demineralised; bovine bone or coral (xenograft); or artificially produced bone-like substances (calcium sulfate with names like Regeneform; and hydroxyapatite or HA, which is the primary form of calcium found in bone) or calcium phosphosilicate which is available in a mouldable putty form. The HA is effective as a substrate for osteoblasts to grow on. Some implants are coated with HA for this reason, although the bone forming properties of many of these substances is a hotly debated topic in bone research groups. Alternatively the bone intended to support the implant can be split and widened with the implant placed between the two halves like a sandwich. This is referred to as a ‘ridge split’ procedure.
Bone graft surgery has its own standard of care. In a typical procedure, the clinician creates a large flap of the gingiva or gum to fully expose the jawbone at the graft site, performs one or several types of block and onlay grafts in and on existing bone, then installs a membrane designed to repel unwanted infection-causing microbiota found in the oral cavity. Then the mucosa is carefully sutured over the site. Together with a course of systemic antibiotics and topical antibacterial mouth rinses, the graft site is allowed to heal (several months).
The clinician typically takes a new radiograph to confirm graft success in width and height, and assumes that positive signs in these two dimensions safely predict success in the third dimension; depth. Where more precision is needed, usually when mandibular implants are being planned, a 3D or cone beam radiograph may be called for at this point to enable accurate measurement of bone and location of nerves and vital structures for proper treatment planning. The same radiographic data set can be employed for the preparation of computer-designed placement guides.
Correctly performed, a bone graft produces live vascular bone which is very much like natural jawbone and is therefore suitable as a foundation for implants.
Considerations
Chrome–cobalt disc with bridges and crowns for dental implants manufactured using WorkNC Dental CAD/CAM
For dental implant procedure to work, there must be enough bone in the jaw, and the bone has to be strong enough to hold and support the implant. If there is not enough bone, more may need to be added with a bone graft procedure discussed earlier. Sometimes, this procedure is called bone augmentation, or guided bone regeneration. Mini dental implants are particularly useful in the endentulous arch with minimal remaining bone facio-lingually.[34] In addition, natural teeth and supporting tissues near where the implant will be placed must be in good health.
In all cases careful consideration must be given to the final functional aspects of the restoration, such as assessing the forces which will be placed on the implant. Implant loading from chewing and parafunction (abnormal grinding or clenching habits) can exceed the biomechanic tolerance of the implant bone interface and/or the titanium material itself, causing failure. This can be failure of the implant itself (fracture) or bone loss, a “melting” or resorption of the surrounding bone.
The dentist must first determine what type of prosthesis will be fabricated. Only then can the specific implant requirements including number, length, diameter, and thread pattern be determined. In other words, the case must be reverse engineered by the restoring dentist prior to the surgery. If bone volume or density is inadequate, a bone graft procedure must be considered first. The restoring dentist may consult with the oral surgeon, periodontist, endodontist, or another trained general dentist to co-treat the patient. Usually, physical models or impressions of the patient’s jawbones and teeth are made by the restorative dentist at the implant surgeons request, and are used as physical aids to treatment planning. If not supplied, the implant surgeon makes his own or relies upon advanced computer-assisted tomography or a cone beam CT scan to achieve the proper treatment plan.
Computer simulation software based on CT scan data allows virtual implant surgical placement based on a barium impregnated prototype of the final prosthesis. This predicts vital anatomy, bone quality, implant characteristics, the need for bone grafting, and maximizing the implant bone surface area for the treatment case creating a high level of predictability. Computer CAD/CAM milled or stereolithography based drill guides can be developed for the implant surgeon to facilitate proper implant placement based on the final prosthesis’ occlusion and aesthetics.
Treatment planning software can also be used to demonstrate “try-ins” to the patient on a computer screen. When options have been fully discussed between patient and surgeon, the same software can be used to produce precision drill guides. Specialized software applications such as ‘SimPlant’ (simulated implant) or ‘NobelGuide’ use the digital data from a patient’s CBCT to build a treatment plan. A data set is then produced and sent to a lab for production of a precision in-mouth drilling guide.
Success rates
Dental implant success is related to operator skill, quality and quantity of the bone available at the site, and the patient’s oral hygiene. The consensus is that implants carry a success rate of around 75%.
One of the most important factors that determine implant success is the achievement and maintenance of implant stability. The stability is presented as an ISQ (Implant Stability Quotient) value. Other contributing factors to the success of dental implant placement, as with most surgical procedures, include the patient’s overall general health and compliance with post-surgical care.
Failure
Failure of a dental implant is often related to the failure of the implant to osseointegrate correctly with the bone, or vice-versa. A dental implant is considered to be a failure if it is lost, mobile or shows peri-implant (around the implant) bone loss of greater than 1.0 mm in the first year and greater than 0.2 mm a year after.
Dental implants are not susceptible to dental caries but they can develop a condition called peri-implantitis. This is an inflammatory condition of the mucosa and/or bone around the implant which may result in bone loss and eventual loss of the implant. The condition is usually, but not always, associated with a chronic infection. Peri-implantitis is more likely to occur in heavy smokers, patients with diabetes, patients with poor oral hygiene and cases where the mucosa around the implant is thin.
Currently there is no universal agreement on the best treatment for peri-implantitis. The condition and its causes is still poorly understood.
Risk of failure is increased in smokers. For this reason implants are frequently placed only after a patient has stopped smoking as the treatment is very expensive. More rarely, an implant may fail because of poor positioning at the time of surgery, or may be overloaded initially causing failure to integrate. If smoking and positioning problems exist prior to implant surgery, clinicians often advise patients that a bridge or partial denture rather than an implant may be a better solution.
Failure may also occur independently of the causes outlined above. Implants like any other object suffers from wear and tear. If the implant(s)in question are replacing commonly used teeth, then these may suffer from wear and tear and after years may crack and break up, although this is a very rare occurrence. The only way to minimize the risk of this happening is to visit your local dentist for regular reviews.
In the majority of cases where an implant fails to integrate with the bone and is rejected by the body the cause is unknown. This may occur in around 5% of cases. To this day we still do not know why bone will integrate with titanium dental implants and why it does not reject the material as a ‘foreign body’. Many theories have been postulated over the last five decades. A recent theory argues that rather than being an active biological tissue response, the integration of bone with an implant is the lack of a negative tissue response. In other words, for unknown reasons the usual response of the body to reject foreign objects implanted into it does not function correctly with titanium implants. It has further been postulated that an implant rejection occurs in patients whose bone tissues actually react as they naturally should with the ‘foreign body’ and reject the implant in the same manner that would occur with most other implanted materials.
Contraindications
There are few absolute contraindications to implant dentistry. However, there are some systemic, behavioral, and anatomic considerations that should be assessed.
Particularly for mandibular (lower jaw) implants, in the vicinity of the mental foramen (MF), there must be sufficient alveolar bone above the mandibular canal also called the inferior alveolar canal or IAC (which acts as the conduit for the neurovascular bundle carrying the inferior alveolar nerve or IAN).
Failure to precisely locate the IAN and MF invites surgical insult by the drills and the implant itself. Such insult may cause irreparable damage to the nerve, often felt as a paresthesia (numbness) or dysesthesia (painful numbness) of the gum, lip and chin. This condition may persist for life and may be accompanied by unconscious drooling.
Uncontrolled Type II diabetes is a significant relative contraindication as healing following any type of surgical procedure is delayed due to poor peripheral blood circulation. Anatomic considerations include the volume and height of bone available. Often an ancillary procedure known as a block graft or sinus augmentation are needed to provide enough bone for successful implant placement.
There is new information about intravenous and oral bisphosphonates (taken for certain forms of breast cancer and osteoporosis, respectively) which may put patients at a higher risk of developing a delayed healing syndrome called osteonecrosis. Implants are contraindicated for some patients who take intravenous bisphosphonates.
The many millions of patients who take an oral bisphosphonate (such as Actonel, Fosamax and Boniva) may sometimes be advised to stop the administration prior to implant surgery, then resume several months later. However, current evidence suggests that this protocol may not be necessary. As of January 2008, an oral bisphosphonate study reported in the February 2008 Journal of Oral and Maxillofacial Surgery, reviewing 115 cases that included 468 implants, concluded “There is no evidence of bisphosphonate-associated osteonecrosis of the jaw in any of the patients evaluated in the clinic and those contacted by phone or e-mail reported no symptoms.”
The American Dental Association had addressed bisphosphonates in an article entitled “Bisphosphonate medications and your oral health,” In an Overview, the
Bruxism (tooth clenching or grinding) is another consideration which may reduce the prognosis for treatment. The forces generated during bruxism are particularly detrimental to implants while bone is healing; micromovements in the implant positioning are associated with increased rates of implant failure. Bruxism continues to pose a threat to implants throughout the life of the recipient. Natural teeth contain a periodontal ligament allowing each tooth to move and absorb shock in response to vertical and horizontal forces. Once replaced by dental implants, this ligament is lost and teeth are immovably anchored directly into the jaw bone. This problem can be minimized by wearing a custom made mouthguard (such an NTI appliance) at night.
Postoperatively, after implants have been placed, there are physical contraindications that prompt rapid action by the implantology team. Excessive or severe pain lasting more than three days is a warning sign, as is excessive bleeding. Constant numbness of the gingiva (gum), lip and chin—usually noticed after surgical anesthesia wears off—is another warning sign. In the latter case, which may be accompanied by severe constant pain, the standard of care calls for diagnosis to determine if the surgical procedure insulted the IAN. A 3D cone beam X-ray provides the necessary data, but even before this step a prudent implantologist may back out or completely remove an implant in an effort to restore nerve function because delay is usually ineffective. Depending upon the evidence visible with a 3D X-ray, patients may be referred to a specialist ierve repair. In all cases, speed in diagnosis and treatment are necessary.
Market
In the
Any practitioner who carries out implant treatment, whether in the surgical insertion or the final provision of the prosthesis, must be adequately trained. Legal training requirements differ between countries.
In
The fast growing demand for prosthetic solutions based upon dental implants caused the birth of literally hundreds of different brands available on the market, about
Prices
Due to high prices of implants – complete implant with a crown & an abutment in
However dental tourism is not the best option for everyone. If you are suffering from other medical difficulties apart from your dental situation such as heart, blood, respiratory or mobility problems, it may be a safer choice to stay closer to home. But, if you’re ieed of a major dental restoration or reconstruction involving dental implants, a bone graft or a full smile makeover, then you can certainly make great savings and have potentially better access to excellent dental doctors and top-level facilities.
Mini dental implant
Mini dental implants (MDIs) are small diameter dental implants.
Dental implants may be split into two separate categories based on the diameter of the device. Small diameter dental implants, most often referred to as ‘Mini Implants’, are those with a diameter less than three millimeters (3mm.) Likewise, standard or conventional implants are those implants larger than 3mm in diameter, but most commonly 4- 5mm. As a rule of thumb, Mini Dental Implants are at least half the price of conventional implants and sometimes a quarter of the price of conventional implants.
Mini dental implants, or MDIs, are sometimes referred to as SDIs (small diameter implants), as well as NDIs (narrow body implants). Although mini dental implant is actually a trade name for the most widely used small diameter implant, the 3M™ ESPE™ MDI Mini Dental Implant, the dental industry has adopted the term to describe this class of implants. Some small diameter implants are used as anchors in orthodontic cases and are called TADs, or temporary anchorage devices. One example of a TAD is the Unitek™ Temporary Anchorage Device System. These differ from the more common mini dental implants in that they are removed after they are no longer needed and orthodontic treatment is completed.
Mini Dental Implants are constructed of various titanium alloys. The same applies to traditional implants.

![]()
Mini Dental Implant by 3M ESPE
Design
Currently, mini dental implants have a diameter of 1.8mm to 2.9mm and are offered in various lengths. It is important to note that the pull out strength of an implant has been shown to be based on its length rather than its diameter. Multiple tip, thread, body and head designs are available across the category as well. Most tip designs are sharp or slightly blunted to provide self tapping ability of the implant through the medullary bone. Some blunted designs taut a compression of the bone as an advantage. Thread designs vary from thin to thick and thread spacing is also variable. The design variations allow for use of the implants in the different densities of bone (D1-very dense, D2, and D3-soft) found throughout the mouth. The body connects the tip with the prosthetic head and can be a parallel sided cylinder or a progressively tapered cone. The aforementioned design elements contribute to enhancing initial stability. The choice depends again on the bone density encountered in the desired implant location. For one piece dental implants such the minis, the concept of initial (mechanical) stability is paramount for success. This is based on mechanical retention of the implant in the bone (See the osseointegration page), as well as the strength of the implant. There can be statistically significant differences in the strength of the implant. According to Binon, adequate mechanical characteristics are needed for an implant to resist functional occlusal loads.
The prosthetic head allows the dental prosthesis to connect to the implant and anchor it to the bone. It also connects to the implant driver during placement. Square, rectangular, or o-ball heads are common and connect easily to a simple set of corresponding drivers. Fixed crowns or bridges can be cemented directly to the square or cubic head of the mini. Subsequently, a sphere was milled into the square portion of the head allowing for a more elegant restorative solution. This ‘o-ball’ design became a popular solution to secure loose dentures. Other standard prosthetic options for removable and fixed solutions do exist and custom options are available from various dental labs.
Uses
Mini dental implants are extremely valuable for endentulous patients that have loose lower dentures and want an easy solution to secure them in place. Most denture patients have highly resorbed jawbones (Mandible and/or maxillary bones) and bone augmentation, aka bone graft, is required for a standard dental implant solution. Moreover, health status of many senior citizens contraindicates invasive dental treatment, such as a conventional implant. In contrast to conventional implants, a survey of 200 clinicians indicated that a flap procedure was mostly (80% of the time) unnecessary for placing MDIs. Healing time is decreased, as the ability to avoid flap surgery aids in healing (the periosteum is left undisturbed) and immediate satisfaction achieved with this minimally invasive approach. The shorter treatment time translates to lower costs as well; an important factor because implants are not typically covered by dental insurance programs.
Although not as widely utilized, many MDIs are FDA approved to be used for fixed crown and bridge installations as well.[9][10] Proper case selection is critical but the available literature has demonstrated success that rivals standard implants. This means if you are missing a tooth or multiple teeth, a mini implant may be placed and a crown fabricated to cement on to the head of the implant.
Another important indication for Mini Dental Implants is the transitional stabilization indication. In this instance, Mini Dental Implants are used to give temporary support to the denture while the conventional implants and bone graft are healing.[9]
Procedure
Mini dental implants are placed in a flapless and minimally invasive procedure under local anesthetic. This is in sharp contrast to conventional implants, which are often placed in a procedure requiring a flap, bone graft, and/or significant healing time[13]. In the
Pilot hole being drilled for MDI placement
Four 3M™ ESPE™ MDI Mini Dental Implants in mandible
Osseointegration
Osseointegration derives from the Greek osteon, bone, and the Latin integrare, to make whole. The term refers to the direct structural and functional connection between living bone and the surface of a load-bearing artificial implant. Osseointegration has enhanced the science of medical bone and joint replacement techniques.
Osseointegration may also be defined as:
1. Osseous integration, the apparent direct attachment or connection of osseous tissue to an inert alloplastic material without intervening connective tissue.
2. The process and resultant apparent direct connection of the endogenous material surface and the host bone tissues without intervening connective tissue.
3. The interface between alloplastic material and bone.
History

![]()
Titanum implant (black) integrated into bone (red): Histologic section
In 1952, Per-Ingvar Brånemark of
In dental medicine the implementation of osseointegration started in the mid-1960s as a result of Brånemark’s work. In 1965 Brånemark, who was at the time Professor of Anatomy at the University of Gothenburg, placed dental implants into the first human patient – Gosta Larsson. This patient had a cleft palate defect and required implants to support a palatal obturator. Gosta Larsson died in 2005, with the original implants still in place after 40 years of function.
In the mid-1970s Brånemark entered into a commercial partnership with the Swedish defense company Bofors to manufacture dental implants and the instrumentation required for their placement. Eventually an offshoot of Bofors, Nobel Pharma, was created to concentrate on this product line. Nobel Pharma subsequently became Nobel Biocare.
Brånemark spent almost 30 years fighting the scientific community for acceptance of osseointegration as a viable treatment. In
Applications
· Dental implants, including Mini dental implants, are by far the main field of application
· Retention of a craniofacial prosthesis such as an artificial ear (ear prosthesis), maxillofacial reconstruction, eye (orbital prosthesis), or nose (nose prosthesis)
· Bone anchored limb prostheses
· Bone anchored hearing conduction amplification (Bone Anchored Hearing Aid)
· Knee and joint replacement
Theories
Two theories regarding the chemical mechanism by which endosteal implants integrate with bone have been proposed. Osseointegration, as defined above, contrasts with fibrosseous integration, in which soft tissues such as fibers and/or cells are interposed between the two surfaces.
Brånemark’s theory of osseointegration
Brånemark proposed that implants integrate such that the bone is laid very close to the implant without any intervening connective tissue. The titanium oxide permanently fuses with the bone, as Brånemark showed in 1950s.
Weiss’ theory of fibro-osseous integration
Weiss’ theory states that there is a fibro-osseous ligament formed between the implant and the bone and this ligament can be considered as the equivalent of the periodontal ligament found in the gomphosis. He defends the presence of collagen fibres at the bone-implant interface. He interpreted it as the peri-implantal ligament with an osteogenic effect. He advocates the early loading of the implant.
Osseointegration versus Biointegration
In 1985, Dr. C. de Putter proposed two ways of implant anchorage or retention as mechanical and bioactive. Mechanical retention can be achieved in cases where the implant material is a metal, for example, commercially pure titanium and titanium alloys. In these cases, topological features like vents, slots, dimples, threads (screws), etc. aid in the retention of the implant. There is no chemical bonding and the retention depends on the surface area: the greater the surface area, the greater the contact.
Bioactive retention can be achieved in cases where the implant is coated with bioactive materials such as hydroxyapatite. These bioactive materials stimulate bone formation leading to a physico-chemical bond. The implant is ankylosed with the bone.
Technique
For osseointegrated dental implants, metallic, ceramic, and polymeric materials have been used, in particular titanium. To be termed osseointegration the connection between the os and the implant need not be 100 percent, and the essence of osseointegration derives more from the stability of the fixation than the degree of contact in histologic terms. In short it represents a process whereby clinically asymptomatic rigid fixation of alloplastic materials is achieved, and maintained, in bone during functional loading. When osseointegration occurs, the implant is tightly held in place by the bone. The process typically takes several weeks or months to occur which is well enough for the implant dentist to complete the restorations. The fact is that the degree of osseointegration of implants is a matter of time. First evidence of integration occurs after a few weeks, while more robust connection is progressively effected over the next months or years. Though the osseointegrated interface becomes resistant to external shocks over time, it may be damaged by prolonged adverse stimuli and overload, which may result in implant failure. In studies performed using 3M™ ESPE™ MDI Mini dental implants, it was noted that the absence of micromotion at the bone-implant interface was necessary to enable proper osseointegration. Further, it was noted that there is a critical threshold of micromotion above which a fibrous encapsulation process occurs, rather than osseointegration. Already Brånemark stated that the implant should not be loaded and left out of function during the healing period for osseous integration to occur.
Other complications may arise even in the absence of external impact. One issue is the growing of cement. Iormal cases, the absence of cementum on the implant surface prevents the attachment of collagen fibers. This is normally the case due to the absence of cementum progenitor cells in the area receiving the implant. However, when such cells are present, cement may form on or around the implant surface, and a functional collagen attachment may attach to it.
Advances in materials engineering: metal foams
Since
The process of osseointegration in metal foams is similar to that in bone grafts. The porous bone-like properties of the metal foam contribute to extensive bone infiltration, allowing osteoblast activity to take place. In addition, the porous structure allows for soft tissue adherence and vascularization within the implant. These materials are currently deployed in hip replacement, knee replacement and dental implant surgeries.
Osseoincorporation
Osseoincorporation refers to the healing potential of bone onto an implant surface and into an implant structure. Three dimensional, porous implantable materials utilized in the orthopedic and dental implant industries offer the potential for ingrowth as well as ongrowth or osseoincorporation.
Conventional textured or coated implant surfaces are designed to achieve bone-to-implant contact, or ongrowth. Per-Ingvar Brånemark defined this ongrowth phenomenon, osseointegration, as “the direct structural and functional connection between ordered, living bone and the surface of a load-carrying implant.” In the case of dental implants, they osseointegrate. Porous implantable materials are designed for bone to grow not only onto the material but also into its pores, and in some cases interconnecting within the material’s structure, in a process called osseoincorporation.
In some cases, the patient has periodontal defects (damaged or poor bone structure) which hinder osseointegration. Guided tissue and/or bone regeneration may be necessary before the bone can osseointegrate with the dental implant. In this case a combination of barrier membranes, bone tacks, and supplemental autogenous bone may be required to promote proper osseointegration. In addition, implant surface modification has been studied and now integrated, thus promoting an optimal tissue-implant interface (i.e. osseointegration, implant-gingival seal).
Dental Implants: Consultation, Procedure, Recovery and Aftercare
Dental implants are artificial tooth replacements used to replace a missing tooth or teeth, helping to stop or prevent jaw bone loss. The dental implant procedure is categorized as a form of prosthetic (artificial replacement) dentistry, though it also is a form of cosmetic dentistry.
By replacing missing tooth roots, implants offer more than an esthetic enhancement, providing people with the strength and durability required to eat all the foods they love, without struggling to chew. Although you have a number of restorative options for the treatment of missing teeth, none have proven to be as functionally effective and durable as implants.
In many cases, dental implants may be the only logical choice for the restoration of all necessary functionality of the teeth and supporting structures.
Tooth Loss
Teeth are lost because of:
· Root canal failure
· Gum disease (Periodontitis)
· Trauma to the mouth (tooth injury)
· Excessive wear and tear
· Congenital defects
People who have lost teeth might feel too self-conscious to smile or talk. Additionally, biting irregularities caused by tooth loss can have a negative effect on eating habits and this can lead to secondary health problems like malnutrition. Regardless of the nature of problems related to tooth loss, dental implants may provide a simple remedy with proven results.
Dental Implants Consultation and Treatment Planning
To determine if implants are right for you, a consultation with your dentist, oral surgeon, and/or periodontist or prosthodontist is needed. During this appointment, your dental professional will conduct a thorough examination of your teeth and gums. This may involve a combination of X-rays and computer tomography scans (CT scans) to ensure that sufficient bone structure exists for placing the implant(s), and to determine the exact location the implant should be placed.
Based on the condition of your oral tissues, oral hygiene and personal habits, and your commitment to follow your dentist’s aftercare instructions, your dentist will advise you of your most appropriate dental implant treatment plan. Some patients with insufficient bone or gum tissue require bone or soft tissue grafts, and/or the use of small diameter implants (also called mini implants).
Your treatment plan could involve the immediate placement of an implant and restoration at the same appointment, or require separate procedures to place the implant, allow healing and then place the restoration. In some instances, a series of procedures may be required to place tissue and bone grafting materials, allow time for healing, place the implant and allow it to integrate with your bone, and then place the restoration. Depending on your situation, your dental professional will advise you of how long the entire treatment process will take, how many appointments will be necessary and what you can expect after each procedure.
Oral Surgery
Can oral surgery correct your functional dental concern?
The consultation also will include discussion of options for local anesthesia (to numb the affected and surrounding areas) and sedation dentistry, if necessary.
The Dental Implant Procedure
Today’s dental implants are virtually indistinguishable from other teeth. This appearance is aided in part by the structural and functional connection between the dental implant and the living bone. Implants are typically placed in a single sitting but require a period of osseointegration.
Osseointegration is the process by which direct anchorage of a dental implant root and the bone of the jaw occurs. Osseointegrated implants are the most commonly used and successful type of dental implant. An osseointegrated implant takes anywhere from three to six months to anchor and heal, at which point your dentist can complete the procedure with the placement of a crown. Once the implant has anchored with the jawbone, artificial prosthesis may be attached and the process is done. If osseointegration does not occur, the implant will fail.
Detailed procedural steps are as follows:
Preparing the Jaw for Implantation: A dental implant restoration is commonly composed of a titanium material screw and a crown. A small-diameter hole (pilot hole) is drilled at edentulous (where there is no tooth) jaw sites in order to guide the titanium screw that holds a dental implant in place. To avoid damaging vital jaw and face structures like the inferior alveolar nerve in the mandible (lower jaw), a dentist must use great skill and expertise when boring the pilot hole and sizing the jaw bone.
Placement of the Implant: After the initial pilot hole has been drilled into the appropriate jaw site, it is slowly widened to allow for placement of the implant screw. Once in place, surrounding gum tissue is secured over the implant and a protective cover screw is placed on top to allow the site to heal and osseointegration to occur. After up to six months of healing, your dentist will uncover the implant and attach an abutment (which holds the crown or tooth-like replacement) to the implant. In some cases, the abutment may be attached during the initial procedure. When the abutment is in place, your dentist then will create a temporary crown. The temporary crown serves as a template around which the gum grows and shapes itself in a natural way. The process is completed when the temporary crown is replaced with a permanent crown.
Dental Implants Recovery and Aftercare
Gingival Sculpting
Reinvent your smile with gum tissue contouring.
Dental implant recovery depends on a number of factors, including the various procedures required to complete your treatment. However, it is generally recognized that once an implant has been placed, maintaining diligent oral hygiene habits is required to ensure proper fusing of the implant and bone structure. Failure to floss and brush is a leading cause of implant failure, and infection can occur if the implant and surrounding areas are not cleaned properly. Smoking also is attributed to high failure rates with dental implants and should be avoided following implant procedures.
When dental implants are used to support crown restorations (like individual teeth), the entire treatment procedure may take anything from three to nine months to complete.
Healing from the surgical procedure to place the dental implant(s) takes up to six months, while the fitting and seating of the crown(s) can take up to two months. Again, this timeframe depends on individual cases and treatments. Follow-up appointments with your treatment coordinators are essential for monitoring your progress. Additionally, even after the abutment and crown, bridge or implant-supported denture have been placed, routine follow-up appointments and cleanings still are required with your dentist and hygienist to ensure the longevity of your treatment.
If cared for properly, an implant restoration can remain in place for more than 40 years. It is generally recognized that once an implant has been placed, maintaining diligent oral hygiene habits is required to ensure proper fusing of the implant and bone structure. Failure to floss and brush is a leading cause of implant failure, and infection can occur if the implant and surrounding areas are not cleaned properly.
Dental Spa
Say goodbye to anxiety & dental phobias.
Implant Surgery Follow-up Care
After the initial surgical procedure, discomfort should be minimal. Swelling of your gums and face may occur, as well as minor bleeding and bruising of the implant site. Prescription pain medications may be prescribed by your dentist to relieve any pain or discomfort you feel after the procedure.
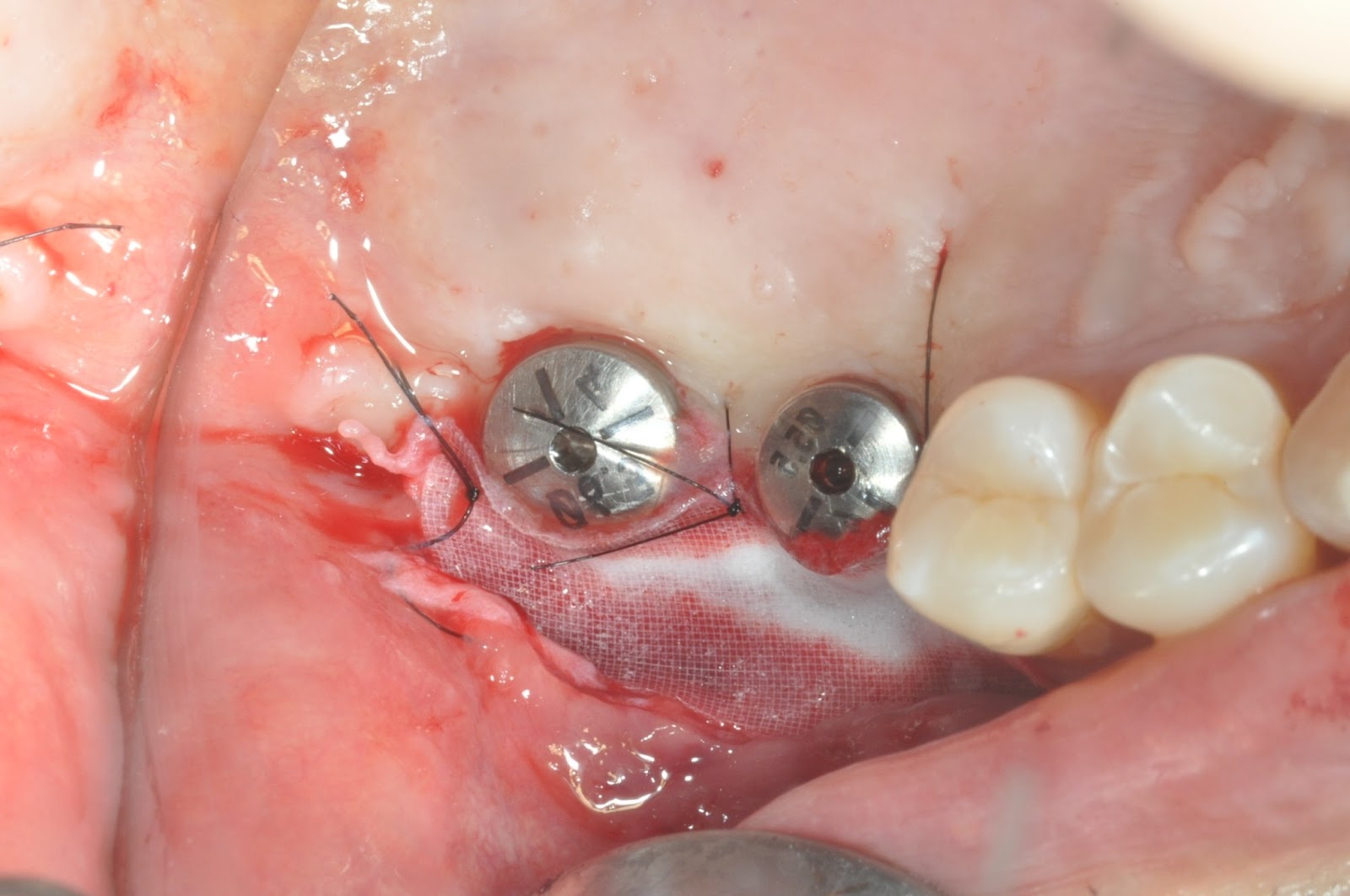
For five to seven days after surgery, your diet should be restricted to soft foods. If stitches are present, they may need to be removed by your dentist; however, self-dissolving stitches that do not require removal are typically used.
If provisional restorations were placed along with the dental implant, it will be important to clean them as you would your natural teeth to ensure the best possible healing and fusing of the implant. ![]()
A dental implant is an artificial tooth root that a periodontist places into your jaw to hold a replacement tooth or bridge. Dental implants are an ideal option for people in good general oral health who have lost a tooth or teeth due to periodontal disease, an injury, or some other reason.
While high-tech iature, dental implants are actually more tooth-saving than traditional bridgework, since implants do not rely oeighboring teeth for support.
Dental implants are so natural-looking and feeling, you may forget you ever lost a tooth.You know that your confidence about your teeth affects how you feel about yourself, both personally and professionally. Perhaps you hide your smile because of spaces from missing teeth. Maybe your dentures don’t feel secure. Perhaps you have difficulty chewing. If you are missing one or more teeth and would like to smile, speak and eat again with comfort and confidence, there is good news! Dental implants are teeth that can look and feel just like your own! Under proper conditions, such as placement by a periodontist and diligent patient maintenance, implants can last a lifetime. Long-term studies continue to show improving success rates for implants.
What Dental Implants Can Do?
Replace one or more teeth without affecting bordering teeth.
Support a bridge and eliminate the need for a removable partial denture.
Provide support for a denture, making it more secure and comfortable.
Types of Implants in Use Today
Endosteal (in the bone): This is the most commonly used type of implant. The various types include screws, cylinders or blades surgically placed into the jawbone. Each implant holds one or more prosthetic teeth. This type of implant is generally used as an alternative for patients with bridges or removable dentures.
Subperiosteal (on the bone): These are placed on top of the jaw with the metal framework’s posts protruding through the gum to hold the prosthesis. These
types of implants are used for patients who are unable to wear conventional dentures and who have minimal bone height.
Advantages of Dental Implants Over Dentures or a Bridge
Every way you look at it, dental implants are a better solution to the problem of missing teeth.
Esthetic Dental implants look and feel like your own teeth! Since dental implants integrate into the structure of your bone, they prevent the bone loss and gum recession that often accompany bridgework and dentures. No one will ever know that you have a replacement tooth.
Tooth-saving Dental implants don’t sacrifice the quality of your adjacent teeth like a bridge does because neighboring teeth are not altered to support the implant. More of your own teeth are left untouched, a significant long-term benefit to your oral health!
Confidence Dental implants will allow you to once again speak and eat with comfort and confidence! They are secure and offer freedom from the irksome clicks and wobbles of dentures. They’ll allow you to say goodbye to worries about misplaced dentures and messy pastes and glues.
Reliable The success rate of dental implants is highly predictable. They are considered an excellent option for tooth replacement.
Are You a Candidate for Dental Implants?
The ideal candidate for a dental implant is in good general and oral health. Adequate bone in your jaw is needed to support the implant, and the best candidates have healthy gum tissues that are free of periodontal disease.
Dental implants are intimately connected with the gum tissues and underlying bone in the mouth. Since periodontists are the dental experts who specialize in precisely these areas, they are ideal members of your dental implant team. Not only do periodontists have experience working with other dental professionals, they also have the special knowledge, training and facilities that you need to have teeth that look and feel just like your own. Your dentist and periodontist will work together to make your dreams come true.
What Is Treatment Like?
This procedure is a team effort between you, your dentist and your periodontist. Your periodontist and dentist will consult with you to determine where and how your implant should be placed. Depending on your specific condition and the type of implant chosen, your periodontist will create a treatment plan tailored to meet your needs. Click for more information about the treatment options described below.
Replacing a Single Tooth If you are missing a single tooth, one implant and a crown can replace it. A dental implant replaces both the lost natural tooth and its root.
Replacing Several Teeth If you are missing several teeth, implant-supported bridges can replace them. Dental implants will replace both your lost natural teeth and some of the roots.
Replacing All of Your Teeth If you are missing all of your teeth, an implant-supported full bridge or full denture can replace them. Dental implants will replace both your lost natural teeth and some of the roots.
Sinus Augmentation A key to implant success is the quantity and quality of the bone where the implant is to be placed. The upper back jaw has traditionally been one of the most difficult areas to successfully place dental implants due to insufficient bone quantity and quality and the close proximity to the sinus. Sinus augmentation can help correct this problem by raising the sinus floor and developing bone for the placement of dental implants.
Ridge Modification Deformities in the upper or lower jaw can leave you with inadequate bone in which to place dental implants. To correct the problem, the gum is lifted away from the ridge to expose the bony defect. The defect is then filled with bone or bone substitute to build up the ridge. Ridge modification has been shown to greatly improve appearance and increase your chances for successful implants that can last for years to come.
What Can I Expect After Treatment?
As you know, your own teeth require conscientious at-home oral care and regular dental visits. Dental implants are like your own teeth and will require the same care. In order to keep your implant clean and plaque-free, brushing and flossing still apply!
After treatment, your periodontist will work closely with you and your dentist to develop the best care plan for you. Periodic follow-up visits will be scheduled to monitor your implant, teeth and gums to make sure they are healthy.
Picture #1
An animated image of the case.
Notice: the implant already in the jaw bone, the abutment that will be mounted on the implant and finally the implant tooth will be built around the abutment.
The dental implant is placed in the jaw bone and revealed after a few months. In this case during the dental implant surgery the dentist placed a healing cap immediately. During the healing of the gums the gingiva formed a nice shape around the healing cap. This will enable an esthetic finish when placing the final restored tooth.
The abutment is connected to the dental implant.
The final result a beautiful restored dental implant tooth. Notice how the gingiva surrounds the tooth perfectly making it impossible to notice that this is a false tooth!
A single dental implant being inserted into the gum using a special wrench.
Open Wall Sinus lift And Bone Graft Procedure:
The following pictures show the sequence of an open wall sinus lift. The sinus is eached from the outer (buccal) side of the jaw. The gum is cut open and the outer wall of the upper jaw is exposed.
An opening is cut in the bone
The “window” is pushed in – exposing the inner part of the bone and the lower part of the sinus .(The membrane separating the jaw bone from the sinus space is – the sinus membrane.)
Bone graft material is placed in the space and slowly the sinus ceiling is pushed up and more bone graft material is filled into the new space.
Finally the area is stitched up after suficiant bone graft material has been applied into the area.
What are the advantages of Dental Implants
Dental implants restore missing teeth to their most natural condition. The concept behind dental implants is exactly the same as natural teeth. Implant teeth, like natural teeth, anchor to the jaw bone. This is the most important difference between implant teeth and other methods of teeth replacement such as dentures and bridges.
Traditionally missing teeth were replaced with either dentures or bridges. Today, replacing teeth with dentures or bridges is no longer the best option or even an acceptable one. Dental problems associated with these kinds of restorations are complex and varied.
To make a bridge for 1 missing tooth, the 2 adjacent teeth should be drilled down to half the size. This is a destructive process and results in tooth sensitivity and decay on those 2 teeth. In reality 2 healthy teeth are destroyed to replace one missing tooth. The final restoration is a 3 tooth bridge that connects one drilled down tooth to another, with one artificial tooth in the middle. Using dental implant technology, the same missing tooth can be easily replaced with one dental implant, and without any damage to any other teeth in the mouth. The restored implant tooth is individually supported and is not connected to adjacent teeth.
Dentures are also associated with numerous problems. They are bulky, and unstable in the mouth. Because they constantly move during chewing, they are inefficient in masticating solid foods. People using dentures are forced to limit their diet to soft food. They avoid vegetables, fruits, nuts, meat and other essential nutrients that are important for their health and well being. This results in systemic disorders such as digestive and cardiovascular disease.
Because dentures are bulky and cover a lot of surfaces in the mouth, including the palate (roof
of the mouth), they interfere with speech and block the sensation of taste. Dentures often have a clicking sound during chewing which may be embarrassing for people who have them.
People wearing dentures should remove them from their mouth after each use to clean them. This reminds them every day that they have artificial teeth. The emotional and psychological impact of this is profound. Use of denture adhesives to hold dentures in the mouth is quite uncomfortable and has an adverse physical and psychological impact.
These are some of the problems associated with dentures, but by far the most serious problem is facial bone loss and premature aging. This bone loss results in collapse of facial structures, and make the person look much older.
Dental implant advantages are:
With dental implants you can eat all the food you like. Eating with implant teeth is just like natural teeth. Your diet will not be limited to just soft food.
Implant teeth feel, function, and look like natural teeth.
Unlike bulky dentures, implant teeth have the exact size and anatomy as natural teeth
Unlike bridges, implant teeth are not attached to, and do not damage other natural teeth.
Maintenance of facial bone. Dental implants prevent bone loss. This is due to stimulation of the jawbone by the chewing forces transmitted by inserted implants.
Improved chewing ability. Dental implants provide a solid and stable foundation for new teeth. Patients are able to eat without worrying about moving or loose dentures.
Improved phonetics. Eliminating bulky, loose dentures, improves phonetics significantly. Dental implants feel like natural teeth and patients actually forget they have missing teeth.
Improved psychological health. Having dental implants is like having a new set of natural teeth. With all the comfort of eating, talking, and socializing without the fear of embarrassment, the individual’s self image is tremendously enhanced.
Improved esthetics. By preventing bone loss, often through bone repair and replacement, implant procedures significantly improve facial esthetics
Regained chewing awareness. Dental implants directly transmit chewing forces to the jawbone, which helps patient’s chewing awareness. With dentures, the roof of the mouth (palate) and all gum surfaces are covered, which prevents taste and chewing reception.
Maintenance of muscles of chewing and facial expression. A sound, healthy bone structure is vital for intact overlying facial muscles. By preventing facial bone loss, dental implants maintain the integrity of facial muscles.
Increased retention and stability of dentures. With dental implants, loose, instable dentures can effectively be anchored to jawbone and provide stability and retention.
By using dental implants, the use of denture adhesives can be eliminated.
The long term success rate of dental implants is impressively high (close to 100%)
From the replacement of a single missing tooth to extensive reconstruction and replacement of several or even all teeth, we offer the healthiest and most intelligent treatment solutions.
VISTA for single upper anterior tooth + GBR

Pre-OP

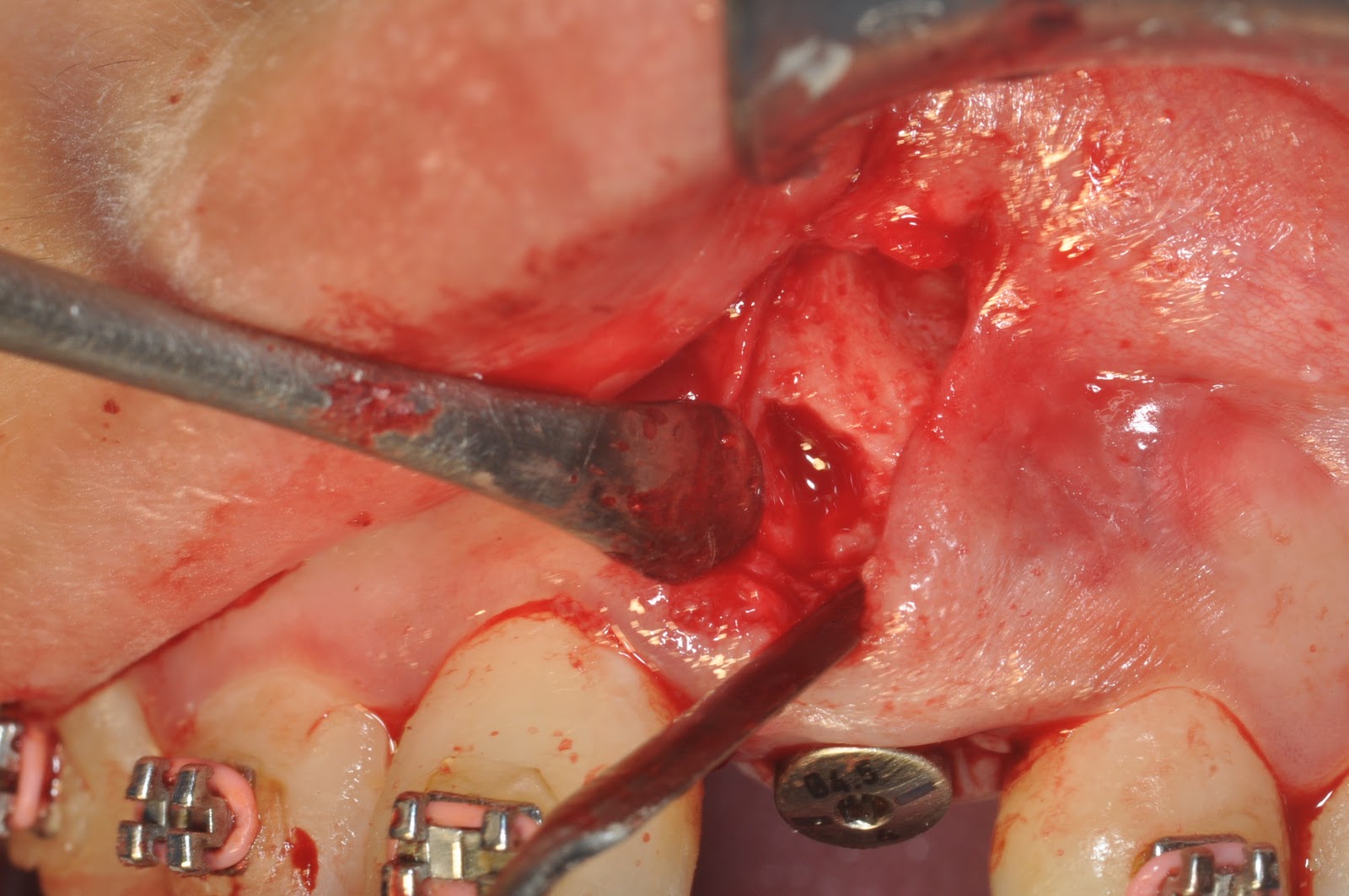
Osseous defects
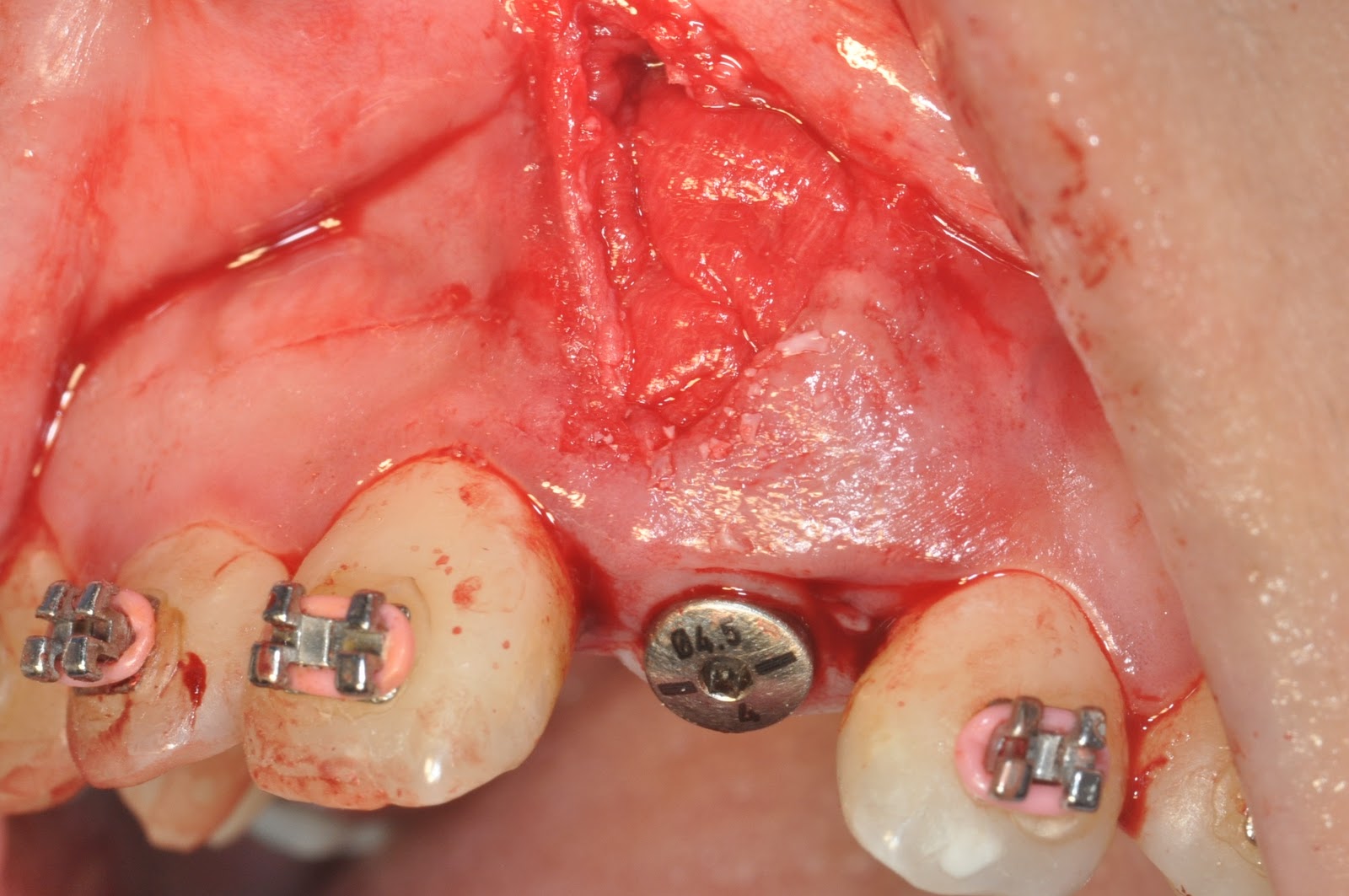
Bio-Oss(L) + Bio-Glide

Suturings
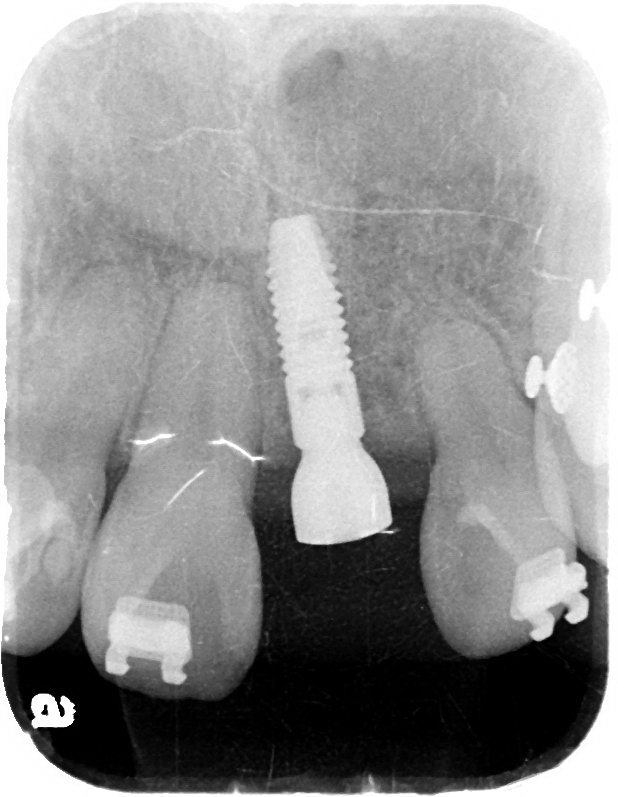

Final restoration(2012.07.27)


PreOP
PostOP

4 wks’ healing

6 mo healing

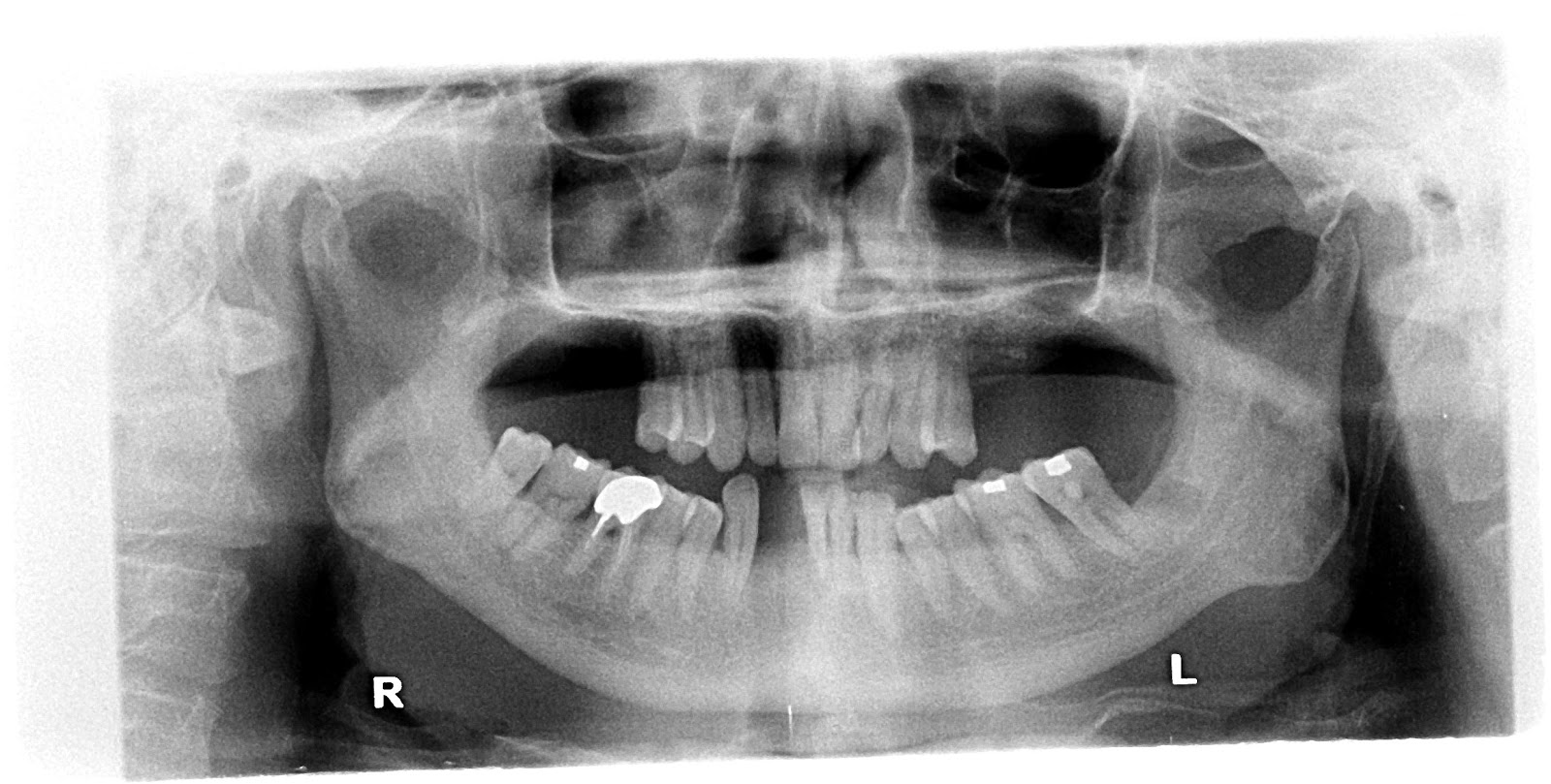
Post dental implantation.
Bone resorption after extraction

