Differential diagnosis of chronic diarrheal syndrome in the clinic of infectious diseases (amebiasis, balantydiasis, giardiasis, intestinal helminthiasis – ascariasis, tryhocephalosis, enterobiosis) with chronic diseases of dygestive system. Problem of helminthoses diagnosis in Ukraine. Features of clinical course, diagnosis and differential diagnosis of helminthoses (trichinosis, stronhiloyidosis, toksokarosis, opisthorchosis, himenolepidosis, teniarinhosis, teniosis)
Amebiasis
http://emedicine.medscape.com/article/212029-overview
Acute intestinal infectious disease caused by Entamoeba histolytica. It is most commonly asymptomatic but symptoms ranging from mild diarrhea to dysentery may occur.
Etiology
There are 2 forms of E. histolytica: motile trophozoite and a cyst. The trophozoite, parasitic form, dwells in the bowel lumen, where it feeds on bacteria or tissue. With diarrhea, the fragile trophozoites pass unchanged in the liquid stool and rapidly die. If diarrhea is not present, the organisms usually encyst before leaving the gut.

a b c
Entamoeba histolitica: a – large vegetative form,
b – opening form,
c – cyst
Diagnosis
Stool examination is usually negative and recovery of the trophozoite from pus in uncommon. In patients with amebic liver abscess, therapeutic trial of amebicides may be the single most helpful diagnostic tool.
Serologic tests are positive in almost all patients with amebic liven abscess and in 80 % of those with acute amebic dysentery.
Differential diagnose
Performed with irritable bowel syndrome, regional enteritis, and diver ticulitis. Amebic dysentery may be confused with salmonellosis, schistosomiasis or ulcerative colitis.
Hepatic amebiasis and amebic abscess must be differentiated from other hepatic infections, including abscesses due to bacterial infection and infected echinococcus cysts.
Ulcer colitis in amebiasis
Faeces in case of amebiasis (“raspberry jelly”)
Balantidiasis
http://www.rightdiagnosis.com/b/balantidiasis/intro.htm
Balantidiasis is a protozoan infection caused by infection with Balantidium coli.
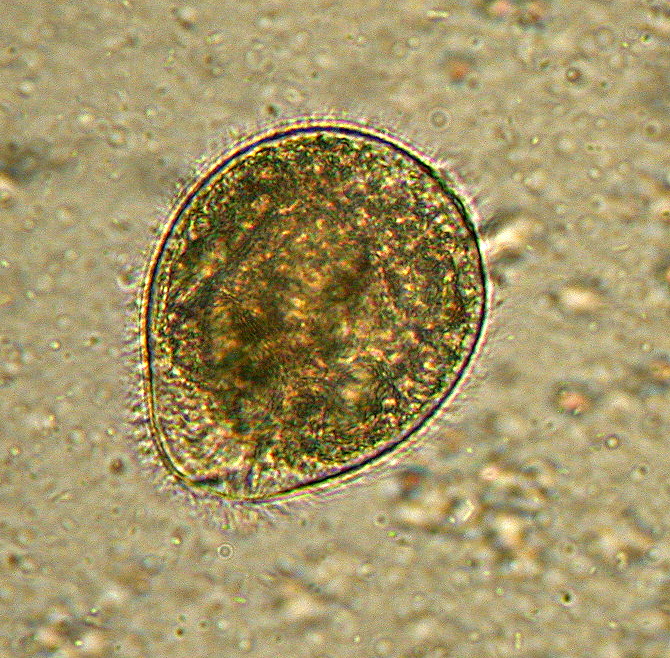
Balantidium coli as seen in a wet mount of a stool specimen. The organism is surrounded by cilia.

A trophozoite of Balantidium coli
Symptoms
Symptoms can be local due to involvement of the intestinal mucosa, or systemic iature and include either diarrhea or constipation.
Treatment
Balantidiasis can be treated with tetracycline, carbarsone, metronidazole, or diiodohydroxyquin.
History and epidemiology
The first study to generate Balantidiasis in humans was undertaken by Cassagrandi and Barnagallo in 1896. However, this experiment was not successful in creating an infection and it was unclear whether Balantidium coli was the actual parasite usedThe first case of Balantidiasis in the Philippines, where it is the most common, was reported in 1904. Currently, Balantidium coli is distributed worldwide but less than 1% of the human population is infected. Pigs are a major reservoir of the parasite, and infection of humans occurs more frequently in areas where pigs comingle with people. This includes places like the Philippines, as previously mentioned, but also includes countries such as Bolivia and Papua New Guinea. But pigs are not the only animal where the parasite is found. In a Japanese study that analyzed the fecal samples in 56 mammalian species, Balantidium coli was found to be present not just in all the wild boars tested (with wild boars and pigs being considered the same species), it was also found in five species of non human primate: Chimpanzee (Pan troglodytes), White-handed gibbon (Hylobates lar), Squirrelmonkey (Saimiri sciurea), Sacred baboon (Comopithecus hamadryas), and Japanese macaque (Macaca fuscata). In other studies, Balantidium coli was also found in species from the orders Rodentia and Carnivora.
Morphology
Balantidium coli exists in either of two developmental stages: Trophozoites and Cysts. In the trophozoite form, they can be oblong or spherical, and are typically 30 to 150 µm in length and 25 to 120 µm in width. It is its size at this stage that allows Balantidium coli to be characterized as the largest protozoan parasite of humans. Trophozoites possess both a macronucleus and a micronucleus, and both are usually visible. The macronucleus is large and sausage-shaped while the micronucleus is less prominent. At this stage, the organism is not infective but it can replicate by transverse binary fission.
Balantidium coli: a –vegetative form,
b – cest form
In its cyst stage, the parasite takes on a smaller, more spherical shape, with a diameter of around 40 to 60 µm.] Unlike the trophozoite, whose surface is covered only with cilia, the cyst form has a tough wall made of one or more layers. The cyst form also differs from the trophozoite form because it is non-motile and does not undergo reproduction. Instead, the cyst is the form that the parasite takes when it causes infection.
Disease diagnosis
The diagnosis of Balantidiasis can be an intricate process, partly because the related symptoms may or may not be present. However, the diagnosis of Balantidiasis can be considered when a patient has diarrhea combined with a probable history of current exposure to amebiasis through travel, contact with infected persons, or anal intercourse. In addition, the diagnosis of Balantidiasis can be made by microscopic examination of stool or tissue samples.
Potential symptoms of balantidiasis include the following:
Diarrhea (watery, bloody, mucoid)
Nausea
Vomiting
Abdominal pain
Anorexia
Weight loss
Headache
Mild colitis
Fever
Severe and marked fluid loss (resembling amebic dysentery)
Physical
Patients with balantidiasis may present with abdominal tenderness, fever, and prolonged diarrhea, which may result in signs of dehydration.
|
|
Ulcerations of the large intestine can be viewed using sigmoidoscopy
Risk factors for balantidiasis include contact with pigs, handling fertilizer contaminated with pig excrement, and living in areas where the water supply may be contaminated by the excrement of infected animals. Poor nutrition, achlorhydria, alcoholism, and immunosuppression may also be contributing factors.
Diagnostic Tests
Since Balantidiasis is not a very common disease, patient history is important in diagnosis. If the patient has recently been exposed to amebiasis (intestinal illness caused by Entamoeba histolytica) through travel or contact with infected individuals combined with diarrheal symptoms, then consider diagnosis of balantidiasis. Also, ask if patient has been in contact with pigs as contact increases the risk of infection.
Balantidiasis can be diagnosed through sampling of the patient’s stools and searching for cysts or trophozoites under a microscope. One can also perform a colonoscopy or sigmoidoscopy to visually examine the intestinal lining and to obtain a biopsy from the large intestines can also provide evidence for the presence of trophozoites.
Giardiasis
http://kidshealth.org/parent/infections/stomach/giardiasis.html
Giardiasis or beaver fever in humans is a diarrheal infection of the small intestine by a single-celled organism called Giardia lamblia. Giardiasis occurs worldwide with a prevalence of 20–30 % in developing countries. In the USA, 20,000 cases are reported to the CDC annually, but the true annual incidence is estimated at 2 million people. Giardia has a wide range of mammalian hosts besides humans, thus making it very difficult to eradicate. For people with compromised immune systems, such as elderly or AIDS patients, giardiasis can be deadly.

Giardia cell, SEM
History of discovery
Antonie van Leeuwenhoek of Delft, Netherlands, described such microorganisms he observed in the stool: “I have sometimes also seen tiny creatures moving very prettily; some of them a bit bigger, others a bit less, than a blood-globule but all of one and the same make. Their bodies were somewhat longer than broad, and their belly, which was flattish, furnished with sundry little paws, wherewith they made such a stir in the clear medium and among the globules, that you might even fancy you saw a woodlouse running up against a wall; and albeit they made a quick motion with their paws, yet for all that they made but slow progress.
Although Leeuwenhoek was the first person to discover G. lamblia, he was not able to provide an informative illustration of the parasite. Further studies and better illustrations of the morphology of the organism in their intestinal environments were made in 1859 by Vilem Lambl, a Czech physician. He also named the organism as Cercomonas intestinalais. Despite his significant contribution, Lambl did not link the diarrheal disease with the Giardia parasite, but rather erroneously assumed that the organism is part of the normal, harmless flora of the intestines.
In 1888, Raphael Anatole Emile Blanchard named the parasite Lamblia intestinalis. In 1915, Charles Wardell Stiles, an American Parasitologist, gave the parasite its current name, Giardia lamblia, to commemorate the work on Giardia by Professor A. Giard in Paris and Dr. Lambl in Prague. Charles Wardell Stiles also suspected a link between Giardia and diarrhea for the first time. The pathogenicity of Giardia was further studied during the First World War, when a large number of soldiers developed diarrhea. Giardia cysts were isolated from their feces and found to cause diarrheal symptoms in laboratory animals. In 1926, a physician in Londoamed Justin Achoo found that Giardia causes malabsorption in some children but not in others. The causal link between Giardia and the disease was finally and conclusively established in 1954 by Dr. Robert Rendroff of the United States. To elucidate the natural history of Giardia, such as the incubation period and the minimal number of cysts needed for infection, Rendroff fed capsules containing knowumbers of Giardia cysts to prisoner volunteers. The incubation period was shown to be 6 to 15 days, and that as few as 10 to 25 cysts were competent to produce infection. Furthermore, Rendroff observed that some patients were cured of Giardia spontaneously without treatment intervention.
Today, Giardia continues to affect large populations of people world wide. In developed nations, Giardia infects 2–5% of the population acutely, people who carry cysts may not know they are infected, as currently there is no treatment for Giardia cysts in the large intestine. In developing countries with poor sanitation and contaminated food or water sources, Giardia may affect up to 20–30 % of the population acutely. It is also the most commonly diagnosed enteric parasite in the United States and Canada.
Transmission
Giardiasis is caused by the ingestion of infective cysts. There are multiple modes of transmission, including person-to-person, water-borne, and venereal. Person-to-person transmission accounts for a majority of Giardia infections and is usually associated with poor hygiene and sanitation. Water-borne transmission is associated with the ingestion of contaminated water. In the U.S. outbreaks typically occur in small water systems using inadequately treated surface water. Venereal transmission happens through fecal-oral contamination. Additionally, diaper changing and inadequate hand washing are risk factors for transmission from infected children. Lastly, food-borne epidemics of Giardia have developed through the contamination of food by infected food-handlers. Giardiasis is spread during periods of heavy rains, such as monsoon runoff.
Symptoms
A range of clinical syndromes may occur, with gastrointestinal syndromes being the most prevalent.
Gastrointestinal
A small number of infected individuals experience an abrupt onset of abdominal cramps, watery diarrhea, vomiting, foul flatus, and fever which may last for 3–4 days before proceeding into a more sub-acute phase. The majority of infected persons develop gradual symptoms that become recurrent or resistant.
In both the acute and insidious onsets of symptoms, stools become greasy and malodorous but do not contain blood or pus because giardiasis does not involve dysenteric symptoms. Watery diarrhea may cycle with soft stools and constipation. Upper GI symptoms including nausea, early satiety, bloating, substernal burning, egg-smelling halitosis, and acid indigestion may be exacerbated by eating and are generally present in the absence of soft stools.
Constitutional
The most common constitutional symptoms are loss of appetite, malaise, and fatigue. Weight loss affects more than 50% of patients. Adults with long lasting malabsorption syndrome and children with failure to thrive may experience chronic illness.
Additional syndromes may include lactose intolerance, biliary tract disease[citatioeeded] and allergic manifestations such as erythema multiforme, bronchospasm and urticaria.
Physical
Abdominal examination may expose nonspecific tenderness even if there is no sign of peritoneal irritation. Rectal examination should expose heme-negative stools and in severe cases, there may be evidence of dehydration.
Long term effects
Studies into the long term effects of giardiasis have not been thoroughly conducted, however, due to inflammation and scarring occurring commonly with giardiasis, possible effects include long term weight loss, malnutrition, failure to thrive, lactose intolerance, as well as chronic inflammation of intestinal lining leading to various forms of cancer. For immunocompromised individuals, these effects can be and often are deadly.
Diagnosis
The most sensitive test for diagnosing giardiasis is ELISA and should be done prior to performing stool ova and parasites (commonly called O&P) and string testing.
It may be found on duodenal biopsies and is in the differential diagnosis of celiac disease.
Treatment
First line of treatment
Metronidazole (Flagyl)
Adult dosage: 250 mg three times a day for 5 days]
Pediatric dosage: 5 mg per kilogram of body weight per dose, 3 times per day, for 5 days
Side effects: Found in 7.1 % of cases. Include unpleasant metallic taste which might cause noncompliance in patients, GI discomfort such as vomiting, nausea, diarrhea, abdominal cramps, pancreatitis, vertigo, headache, CNS toxicity, transient leukemia, dizziness, drowsiness, lassitude, paraethesias, urticaria, and pruritis. It causes mutation in Salmonella and induces tumor in rodents, but mutagenicity has never been observed in humans.
Contraindication: Avoid alcohol while taking metronidazole. Metronidazole causes severe vomiting, headache, and GI discomfort by inhibiting aldehyde dehydrogenase, which breaks down alcohol.
Additional drug facts: Metronidazole is a member of the family of nitroimidazoles, commercially known as Flagyl. The tablets are quickly and completely absorbed by the small intestine and found to have antigiardial effects on the trophozoites both in vivo and in vitro. However, it is ineffective against cysts. The drug is able to penetrate body tissues and could be found in saliva, breast milk, semen, and vaginal fluid. It is metabolized in liver and secreted in urine. Metronidazole targets trophozoites by forming active metabolites, which selectively inhibit DNA segregation in anaerobic protozoa such as Giardia by DNA breakage and cross-linking. It has minimal effects on host cells lining the intestinal lumen. Resistance is induced in laboratory and is correlated with decreased activity of parasite pyruvate.
Tinidazole (Fasigyn)
Adult dosage: 2 g once
Pediatric dosage: 50 mg per kilogram of body weight once (max. 2 g)
Side effects: Side effects similar to metronidazole but appears to be better tolerated and just as effective. Common side effects include bitter taste, vertigo, and GI discomfort. The drug should be taken with food to minimize side effects.
Additional drug facts: Tinidazole was] FDA approved. It is another member of the nitro-imidazole family. Health care providers recommend travelers (especially those traveling to Asian countries) buy the drug at the country of their destination and take it in an event of giardia infection. The drug tablets can also be crushed and mixed with cherry syrup (Humco and others) for children. The syrup suspension can be kept at room temperature for 7 days and should be shaken before use.
Nitazoxanide
Adult dosage: 500 mg two times a day for 3 days
Pediatric dosage: 1–3 yrs: 100 mg every 12 hours for 3 days; 4–11 yrs: 200 mg every 12 hours for 3 days
Side effects: A variety of side effects were reported but they occurred infrequently in all studies. Studies failed to provide sufficiently similar results for a comprehensive analysis of the side effects of nitazoxanide. Some probable adverse effects include abdominal pain, dyspepsia, constipation, yellow discoloration of urine, dysuria and dry mouth, and dizziness. The drug should be taken with food to minimize adverse effects.
Additional drug facts: nitazoxanide is FDA-approved as an oral suspension for treatment of giardiasis. It can be purchased in 500 mg tablets and in oral suspension.
Alternative treatment
Paramomycin (Humatin)
Adult dosage: 25–35 mg per kilogram of body weight per dose, 3 doses per day for 7 days
Pediatric dosage: 25–35 mg per kilogram of body weight per dose, 3 doses per day for 7 days
Side effects: ototoxicity and nephrotoxicity with systemic administration
Contraindication: Patients with impaired kidney function should use paramomycin with caution
Additional drug facts: Paramomycin is a member of the aminoglycoside family. It inhibits Giardia protein synthesis by targeting the 50S and 30S ribosomal subunits. Its activity in vitro is lower thaitroimidazoles; however, because it is poorly absorbed by small intestine, a higher concentration of the drug remains in the lumen to combat giadia organisms. It is also the choice of drug to treat G. lamblia in resistant infection and during pregnancy.
Furazolidone (Furoxone)
Adult dosage: 100 mg four times a day for 7–10 days
Pediatric dosage: 6 mg per kilogram of body weight per dose, 4 doses per day for 7–10 days
Side effects: Gastrointestinal symptoms (nausea, vomiting, diarrhea) are observed in 10% of patients. Other side effects include brown discoloration of urine, and hemolysis in G6PDH-deficient patients.
Additional drug facts: it is a member of the nitrofuran familypenetrate body tissues and could be found in saliva, breast milk, semen and vaginal fluid. Not recommended to treating pregnant patients because it has been shown to cause mammary tumor in rats and mutations in bacteria.
Quinacrine
Adult dosage: 100 mg three times a day for 5 days
Pediatric dosage: 2 mg per kilogram of body weight, three times per day for 5 days (max. 300 mg/d)
Side effects: bitter taste and vomiting observed in 28% of study participants; yellow/orange discoloration of the skin, sclerae, and urine. Other common side effects include nausea, vomiting, headache, dizziness and fever. Drug induced psychosis has been observed but is very rare. Dermatitis and drug-induced retinopathy are also uncommon. The drug also acts with lower efficacy in children because the drug has bitter taste and children are less compliant.
Contraindication: Pregnant patients should avoid taking the drug because quinacrine can cross placenta and it might cause spina bifida and renal agenesis in the infant.
The drug, unlike metronidazole, also target cysts.
This drug cannot be obtained commercially.
Albendazole (Albenza)
Adult dosage: 400 mg once a day for 5 days
Pediatric dosage: 15 mg per kilogram of body weight per day for 5 to 7 days (max. 400 mg)
Mebendazole (Vermox)
Adult dosage: 200–400 mg per day for 5 to 10 days
Side effects for albendazole and mebendazole: common side effects include anorexia and constipation. Rare side effects include reversible neutropenia and elevated liver function tests. Whether they are teratogenic is unclear
Contraindication of albendazole and mebendazole: albendazole should be taken with caution for pregnant patients because there is a possibility that it might induce tumors. However, animal studies did not reveal increased incidences of cancer.
Additional drug facts: albendazole and mebendazole are members of the benzimidazole family. They target G. lamblia by binding to β-tubulin and stopping cytoskeletal formation. It also interferes with glucose uptake of the organism.
Special circumstances in management therapy
Drug use during pregnancy and lactation
Pregnant patients who are infected but asymptomatic are advised not to receive treatment for Giardia because there are underlying risks in current therapies. For instance, metronidazole is rapidly absorbed and easily enters fetal circulation. Studies have shown mixed results regarding the adverse effects of metronidazole on the development of the fetus. One retrospective study involving 1469 women who took Metronidazole during the first trimester of pregnancy showed no adverse effects on the fetus. However, in the Collaborative Perinatal Project with over 50,000 mother-child pairs, the infants of 31 mothers who took metronidazole during the first trimester of pregnancy were found to developed drug-associated malformation. These older studies are nowadays under attack and considered flawed. More recent studies conclude that “the current data do not support a significant increased risk for birth defects or other adverse effects on the fetus.” Paromomycin is the choice of drug for treating pregnant women infected with Giardia because it is poorly absorbed by the mother and excreted almost 100% in feces; hardly any of the drugs would reach the fetus.
Ascariasis
http://www.rightdiagnosis.com/a/ascariasis/intro.htm
Ascariasis is a human disease caused by the parasitic roundworm Ascaris lumbricoides. Perhaps as many as one quarter of the world’s people are infected, with rates of 45% in Latin America and 95% in parts of Africa. Ascariasis is particularly prevalent in tropical regions and in areas of poor hygiene. Other species of the genus Ascaris are parasitic and can cause disease in domestic animals. Certain genes have been identified in human populations that may increase the susceptibility to infection.
Infection occurs through ingestion of food contaminated with feces containing Ascaris eggs. The larvae hatch, burrow through the intestine, reach the lungs, and finally migrate up the respiratory tract. From there they are then reswallowed and mature in the intestine, growing up to 30 cm (12 in.) in length and anchoring themselves to the intestinal wall.
Infections are usually asymptomatic, especially if the number of worms is small. They may however be accompanied by inflammation, fever, and diarrhea, and serious problems may develop if the worms migrate to other parts of the body.
Epidemiology
Roughly 1.5 billion individuals are infected with this worm, primarily in Africa and Asia. Ascariasis is endemic in the United States including Gulf Coast; in Nigeria and in Southeast Asia. One study indicated that the prevalence of ascariasis in the United States at about 4 million (2 %). In a survey of a rural Nova Scotia community, 28.1 % of 431 individuals tested were positive for Ascaris, all of them being under age 20, while all 276 tested in metropolitan Halifax were negative. Deposition of ova (eggs) in sewage hints at the degree of ascariasis incidence. A 1978 study showed about 75 % of all sewage sludge samples sampled in United States urban catchments contained Ascaris ova, with rates as high as 5 to 100 eggs per litre]. In Frankfort, Indiana, 87.5 % of the sludge samples were positive with Ascaris, Toxocara, Trichuris, and hookworm]. In Macon, Georgia, one of the 13 soil samples tested positive for Ascaris]. Municipal wastewater in Riyadh, Saudi Arabia detected over 100 eggs per litre of wastewater and in Czechoslovakia was as high as 240–1050 eggs per litre.
http://upload.wikimedia.org/wikipedia/commons/b/b7/Ascariasis_world_map_-_DALY_-_WHO2002.svg

Disability-adjusted life year for ascariasis per 100,000 inhabitants in 2002.
Ascariasis can often be measured by examining food for ova. In one field study in Marrakech, Morocco, where raw sewage is used to fertilize crop fields, Ascaris eggs were detected at the rate of 0.18 eggs/kg in potatoes, 0.27 eggs/kg in turnip, 4.63 eggs/kg in mint, 0.7 eggs/kg in carrots, and 1.64 eggs/kg in radish. A similar study in the same area showed that 73% of children working on these farms were infected with helminths, particularly Ascaris, probably as a result of exposure to the raw sewage.
Signs and symptoms
Adult worms (1) live in the lumen of the small intestine. A female may produce approximately 200,000 eggs per day, which are passed with the feces (2). Unfertilized eggs may be ingested but are not infective. Fertile eggs embryonate and become infective after 18 days to several weeks (3), depending on the environmental conditions (optimum: moist, warm, shaded soil). After infective eggs are swallowed (4), the larvae hatch (5), invade the intestinal mucosa, and are carried via the portal, then systemic circulation and/or lymphatics to the lungs . The larvae mature further in the lungs (6) (10 to 14 days), penetrate the alveolar walls, ascend the bronchial tree to the throat, and are swallowed (7). Upon reaching the small intestine, they develop into adult worms (8). Between 2 and 3 months are required from ingestion of the infective eggs to oviposition by the adult female. Adult worms can live 1 to 2 years.
Patients can remain asymptomatic for very long periods of time. As larval stages travel through the body, they may cause visceral damage, peritonitis and inflammation, enlargement of the liver or spleen, toxicity, and pneumonia. A heavy worm infestation may cause nutritional deficiency; other complications, sometimes fatal, include obstruction of the bowel by a bolus of worms (observed particularly in children) and obstruction of the bile or pancreatic duct. More than 796 Ascaris lumbricoides worms weighing up to 550 g [19 ounces] were recovered at autopsy from a 2-year-old South African girl. The worms had caused torsion and gangrene of the ileum, which was interpreted as the cause of death.
Ascaris takes most of its nutrients from the partially digested host food in the intestine. There is limited evidence that it can also pierce the intestinal mucous membrane and feed on blood, but this is not its usual source of nutrition. As a result, Ascaris infection does not produce the anemia associated with some other roundworm infections.[citatioeeded]
In Canada in 1970, a postgraduate student tainted his roommates’ food with Ascaris lumbricoides. Four of the victims became seriously ill; two of these suffered acute respiratory failure.
Diagnosis
The diagnosis is usually incidental when the host passes a worm in the stool or vomit. Stool samples for ova and parasites will demonstrate Ascaris eggs. Larvae may be found in gastric or respiratory secretions in pulmonary disease. Blood counts may demonstrate peripheral eosinophilia. On X-ray, 15–35 cm long filling defects, sometimes with whirled appearance (bolus of worms).
Treatment
Main article: Ascaricide
Pharmaceutical drugs that are used to kill roundworms are called ascaricides and include:
Mebendazole (Vermox) (C16H13N3O2). Causes slow immobilization and death of the worms by selectively and irreversibly blocking uptake of glucose and other nutrients in susceptible adult intestine where helminths dwell. Oral dosage is 100 mg 12 hourly for 3 days.
Piperazine (C4H10N2.C6H10O4). A flaccid paralyzing agent that causes a blocking response of ascaris muscle to acetylcholine. The narcotizing effect immobilizes the worm, which prevents migration when treatment is accomplished with weak drugs such as thiabendazole. If used by itself it causes the worm to be passed out in the feces. Dosage is 75 mg/kg (max 3.5 g) as a single oral dose.
Pyrantel pamoate (Antiminth, Pin-Rid, Pin-X) (C11H14N2S.C23H16O6) Depolarizes ganglionic block of nicotinic neuromuscular transmission, resulting in spastic paralysis of the worm. Spastic (tetanic) paralyzing agents, in particular pyrantel pamoate, may induce complete intestinal obstruction in a heavy worm load. Dosage is 11 mg/kg not to exceed 1 g as a single dose.
Albendazole (C12H15N3O2S) A broad-spectrum antihelminthic agent that decreases ATP production in the worm, causing energy depletion, immobilization, and finally death. Dosage is 400 mg given as single oral dose (contraindicated during pregnancy and children under 2 years).
Thiabendazole. This may cause migration of the worm into the esophagus, so it is usually combined with piperazine.
Hexylresorcinol effective in single dose, mentioned in : Holt, Jr Emmett L, McIntosh Rustin: Holt’s Diseases of Infancy and Childhood: A Textbook for the Use of Students and Practitioners. Appleton and Co, New York,11th edition
Santonin, more toxic than hexylresorcinol, mentioned in : Holt, Jr Emmett L, McIntosh Rustin: Holt’s Diseases of Infancy and Childhood: A Textbook for the Use of Students and Practitioners. Appleton and Co, New York,, 11th edition
Oil of chenopodium, more toxic than hexylresorcinol, mentioned in : Holt, Jr Emmett L, McIntosh Rustin: Holt’s Diseases of Infancy and Childhood: A Textbook for the Use of Students and Practitioners. Appleton and Co, New York, 11th edition
Also, corticosteroids can treat some of the symptoms, such as inflammation.
Native Americans have traditionally used epazote (Chenopodium ambrisioides) for treatment, which was not as powerful as pharmaceutical compounds, but spontaneous passage of Ascarids provided some proof of efficacy.
Prevention
Prevention includes: use of toilet facilities; safe excreta disposal; protection of food from dirt and soil; thorough washing of produce; and hand washing.
Food dropped on the floor should never be eaten without washing or cooking, particularly in endemic areas. Fruits and vegetables should always be washed thoroughly before consumption.
Enterobiasis
http://www.drugs.com/cg/enterobiasis.html
A pinworm infection or enterobiasis is a human parasitic disease and one of the most common childhood parasitic worm infections in the developed world. It is caused by infestation with the parasitic roundworm Enterobius vermicularis, commonly called the human pinworm. Infection usually occurs through the ingestion of pinworm eggs, either through contaminated hands, food, or less commonly, water. The chief symptom is itching in the anal area.

Pinworms (Enterobius vermicularis).
The incubation time from ingestion of eggs to the first appearance of new eggs around the anus is 4 to 6 weeks. Pinworms are usually considered a nuisance rather than a serious disease. Treatment is straightforward in uncomplicated cases, however, elimination of the parasite from a family group or institution often poses significant problems—either due to an incomplete cure or reinfection. Pinworm infection has no association with any socioeconomic level, race or culture.
Signs and symptoms
One third of individuals with pinworm infection are totally asymptomatic. The main symptoms are pruritus ani and perineal pruritus, i.e., itching in and around the anus and around the perineum. The itching occurs mainly during the night, and is caused by the female pinworms migrating to lay eggs around the anus. Both the migrating females and the clumps of eggs are irritating, but the mechanisms causing the intense pruritus have not been explained. The intensity of the itching varies, and it can be described as tickling, crawling sensations, or even acute pain. The itching leads to continuously scratching the area around the anus, which further results in tearing of the skin and complications such as secondary bacterial infections, including bacterial dermatitis (i.e., skin inflammation) and folliculitis (i.e., hair follicle inflammation). General symptoms are insomnia (i.e., persistent difficulties to sleep) and restlessness. A considerable proportion of children suffer from anorexia (i.e., loss of appetite), weightloss, irritability, emotional instability, and enuresis (i.e., inability to control urination). Pinworms cannot damage the skin, and they do not normally migrate through tissues. However, in women they may move onto the vulva and into the vagina, from there moving to external orifice of the uterus, and onwards to the uterine cavity, fallopian tubes, ovaries, and peritoneal cavity. This can cause vulvovaginitis, i.e. an inflammation of the vulva and vagina. This causes vaginal discharge and pruritus vulvae, i.e., itchiness of the vulva. The pinworms can also enter the urethra, and presumably, they carry intestinal bacteria with them. According to Gutierrez (2000), a statistically significant correlation between pinworm infection and urinary tract infections has been shown, however Burkhart & Burkhart (2005) maintain that the incidence of pinworms as a cause of urinary tract infections remains unknown. Incidentally, one report indicated that 36 % of young girls with urinary tract infection also had pinworms. Dysuria (i.e., painful urination) has been associated with pinworm infection.
Pinworm life cycle.
The relationship between pinworm infestation and appendicitis has been researched, but there is a lack of clear consensus in the matter: while Gutierres (2005) maintains that there exists a consensus that pinworms do not produce the inflammatory reaction, Cook (1994) states that it is controversial whether pinworms are causatively related to acute appendicitis, and Burkhart & Burkhart (2004) state that pinworm infection causes symptoms of appendicitis to surface.
Diagnosis
Diagnosis depends on finding the eggs or the adult pinworms. Individual eggs are invisible to the naked eye, but they can be seen using a low-power microscope. On the other hand, the light-yellowish thread-like adult pinworms are clearly visually detectable, usually during the night when they move near the anus, or on toilet paper. Transparent adhesive tape (e.g. Scotch Tape) applied on the anal area will pick up deposited eggs, and diagnosis can be made by examining the tape with a microscope. This test is most successful if done every morning for several days, because the females do not lay eggs every day, and the number of eggs vary. Pinworms do not lay eggs in the feces, but sometimes eggs are deposited in the intestine. As such, routine examination of fecal material gives a positive diagnosis in only 5 to 15 % of infected subjects, and is therefore of little practical diagnostic use. In a heavy infection, female pinworms may adhere to stools that pass out through the anus, and they may thus be detected on the surface on the stool. Adult pinworms are occasionally seen during colonoscopy. On a microscopic level, pinworms have an identifying feature of alae (i.e., protruding ridges) running the length of the worm.
High magnification micrograph of a pinworm in cross section in the appendix.
Treatment
http://www.drugs.com/cg/enterobiasis.html
Although hygiene plays a role, medication is the chief treatment. Because the pharmaceutical drugs kill the adult pinworms but not the eggs, retreatment is recommended in two weeks. If one household member spreads the eggs to another, it will be a matter of two or three weeks before those eggs become adult worms and thus amenable to treatment. The benzimidazole compounds albendazole (brand names e.g., Albenza, Eskazole, Zentel and Andazol) and mebendazole (brand names e.g., Ovex, Vermox, Antiox and Pripsen) are the most effective. They work by inhibiting the microtubule function in the pinworm adults, causing glycogen depletion, thereby effectively starving the parasite. A single 100 milligram dose of mebendazole with one repetition after a week, is considered the safest, and is usually effective with cure rate of 96 %. Mebendazole has no serious side effects, although abdominal pain and diarrhea have been reported. Pyrantel pamoate (also called pyrantel embonate, brand names e.g., Reese’s Pinworm Medicine, Pin-X, Combantrin, Anthel, Helmintox, and Helmex) kills adult pinworms through neuromuscular blockade and is considered as effective as the benzimidazole compounds. Other medications are piperazine, which causes flaccid paralysis in the adult pinworms, and pyrvinium pamoate (also called pyrvinium embonate), which works by inhibiting oxygen uptake of the adult pinworms. Pinworms located in the genitourinary system (in this case, female genital area) may require other drug treatments.
Regardless of the medication used, reinfection is frequent. Asymptomatic infections, often in small children, can serve as reservoirs of infection, and therefore the entire household should be treated regardless of whether or not symptoms are present. Total elimination of the parasite in a household may require repeated doses of medication for up to a year or more.
Diseases due to helminths (Helminthiases)
Diseases due to helminths or worms are caused by unique infectious agents of humans because of their size, their prevalence, the complexity of their life cycles and migration within the host, their ability to undergo direct replication in the definitive human host. The helminths are divided into three groups – the nematodes (round worms) and two groups of flat worms: the trematodes (flukes) and the cestodes (tapeworms).
Trematodes (Schistosomiasis) and other flukes
http://emedicine.medscape.com/article/228392-overview
Flukes and parasitic worms of class Trematoda. The classic shape of digenetic trematode is that of thick, oval leaf, although there are many variations in both shape and size. The length of different fluke species varies from less than 1 mm to several centimetres. All species parasitic in humans belong to the digenetic group in which sexual reproduction in the adult worms is followed by multiplication in the larve stages.
Shistosomiasis (dermatitis, Katayama fever, chronic fibroobstructive sequelae).
Opisthorchiasis. Fascioliasis.
Intestinal flukes – fasciolopsiasis, heterophyiasis.
Lung flukes – paragonimiasis.
Cestodes (Tapeworms).
Segmented worms or tapeworms, cause illness in humans in either or the two stages of their life cycle; the adult stage, which causes signs and symptoms referable to the gastrointestinal tract, where the adult tapeworms resides, and the larval stage, which causes signs and symptoms secondary to enlarging larval cysts in various tissues of the mammalian host.

Skin vesicles on the forearm, created by the penetration of Schistosoma.
Calcification of the bladder wall on a plain x-ray image of the pelvis, in a sub-Saharan man of 44 years old. This is due to urinary schistosomiasis.
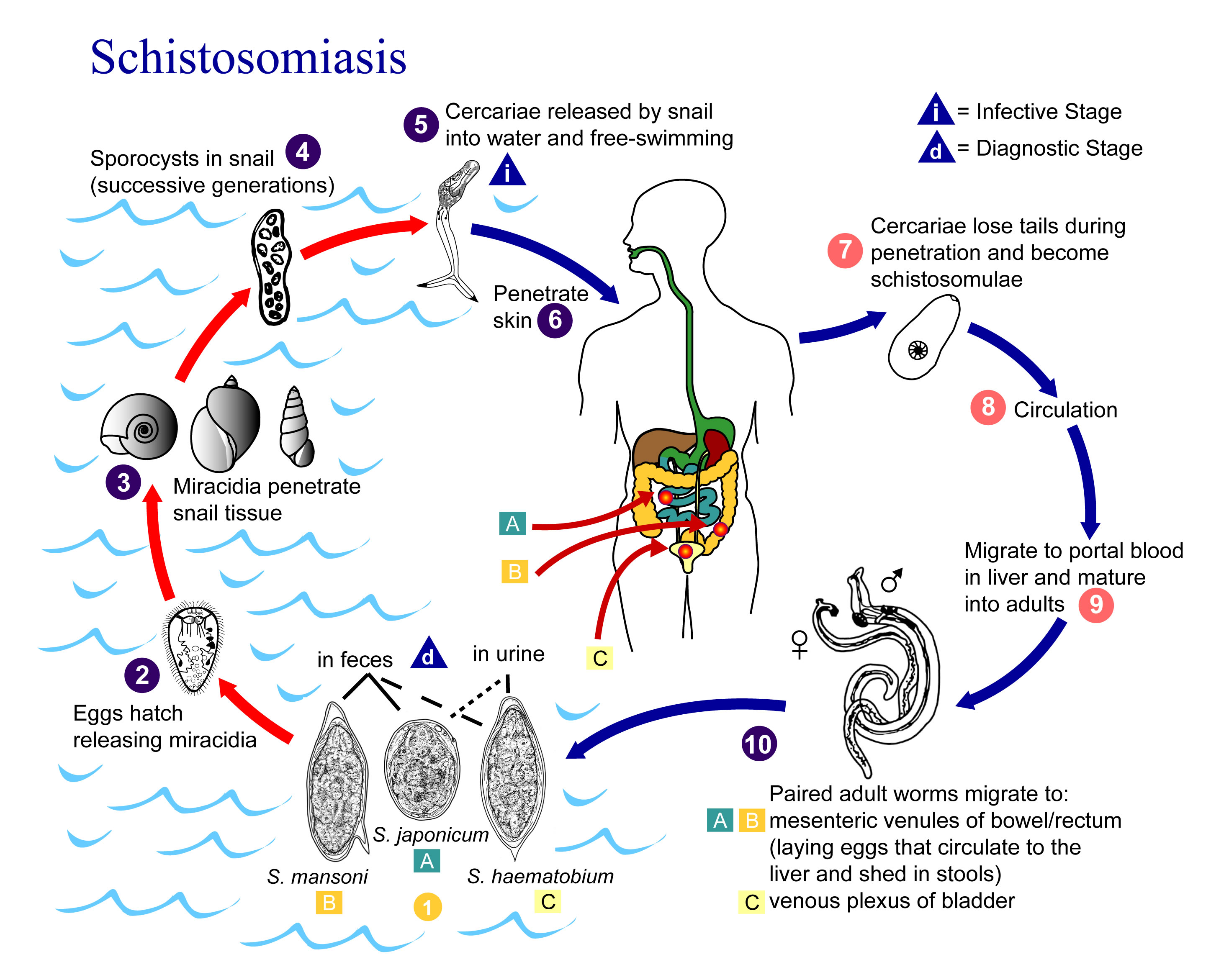
Schistosoma life cycle.
Ethiopian children treated for schistosoma mansoni

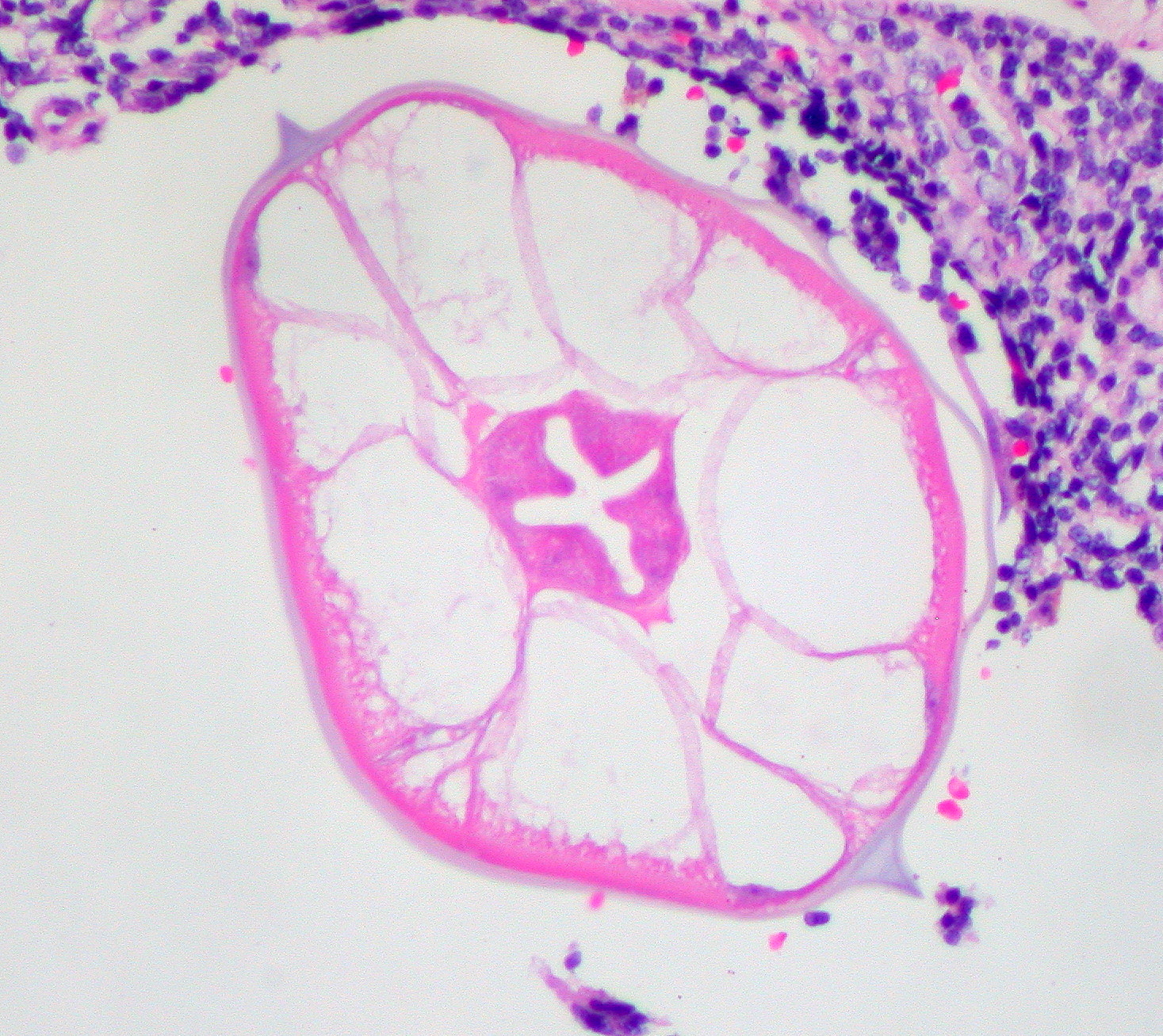
Photomicrography of bladder in S. hematobium infection, showing clusters of the parasite eggs with intense eosinophilia
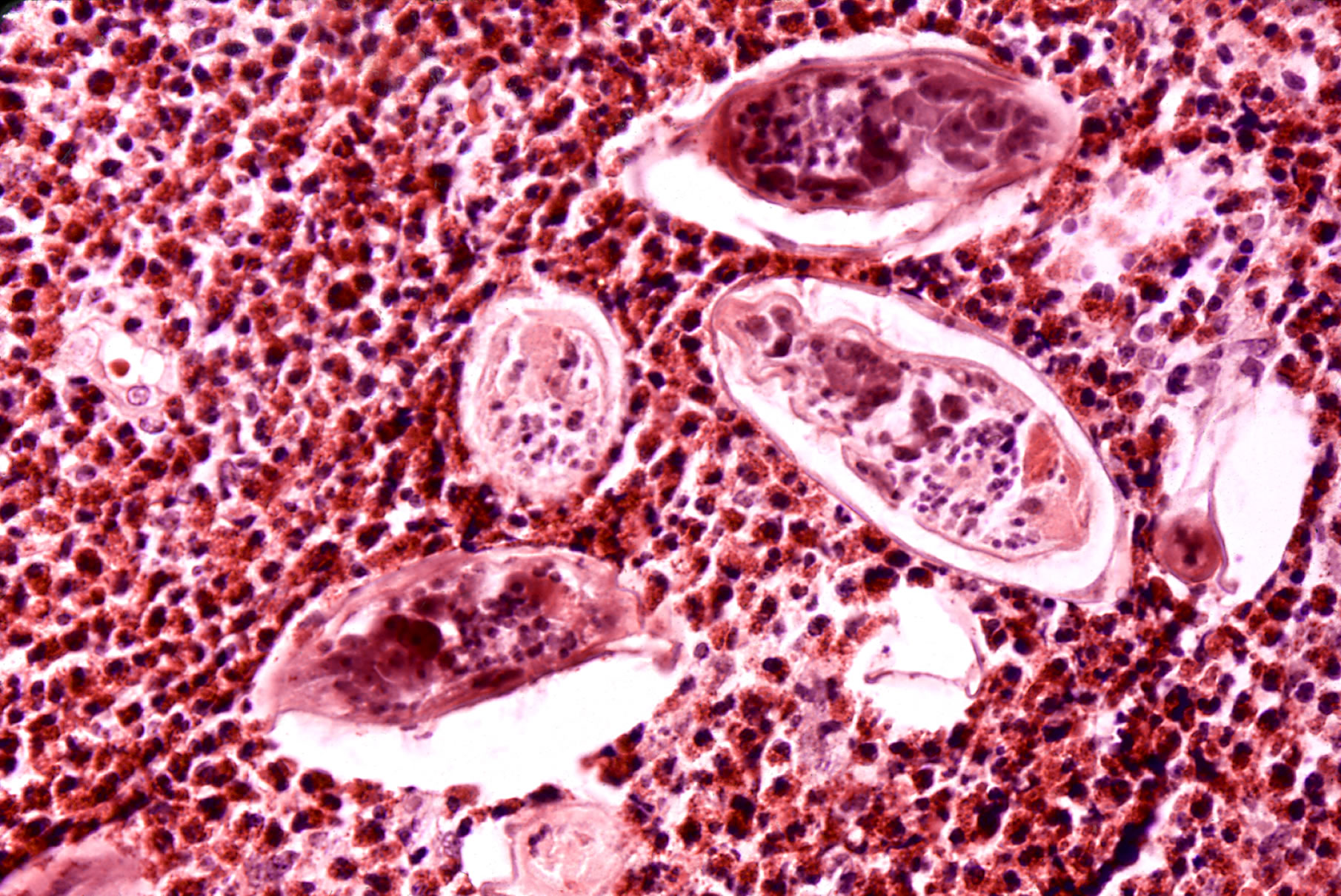
High powered detailed micrograph of Schistosoma parasite eggs in human bladder tissue.

S. japonicum eggs in hepatic portal tract.
Fish tapeworm (Diphyllobothrium latum)
Humans acquire infection with the fish tapeworm by the ingestion of raw freshwater fish. The infection is generally symptomless, but if the worm fixes at the upper end of the jejunum it may successfully compete for the host’s dietary vitamin B12 and a megaloblastic anaemia may occur. The diagnosis is made by the finding of ova in the faeces.
Proglottids of D. latum
Diphyllobothrium is a genus of tapeworm which can cause Diphyllobothriasis in humans through consumption of raw or undercooked fish. The principal species causing diphyllobothriosis is Diphyllobothrium latum, known as the broad or fish tapeworm, or broad fish tapeworm. D. latum is a pseudophyllid cestode that infects fish and mammals. D. latum is native to Scandinavia, western Russia, and the Baltics, though it is now also present in North America, especially the Pacific Northwest. In Far East Russia, D. klebanovskii, having Pacific salmon as its second intermediate host, was identified. Other members of the genus Diphyllobothrium include Diphyllobothrium dendriticum (the salmon tapeworm), which has a much larger range (the whole northern hemisphere), D. pacificum, D. cordatum, D. ursi, D. lanceolatum, D. dalliae, and D. yonagoensis, all of which infect humans only infrequently. In Japan, the most common species in human infection is D. nihonkaiense, which was only identified as a separate species from D. latum in 1986. More recently, a molecular study found D. nihonkaiense and D. klebanovskii to be a single species.
Life cycle
Adult tapeworms may infect humans, canids, felines, bears, pinnipeds, and mustelids, though the accuracy of the records for some of the nonhuman species is disputed. Immature eggs are passed in feces of the mammal host (the definitive host, where the worms reproduce). After ingestion by a suitable freshwater crustacean such as a copepod (the first intermediate host), the coracidia develop into procercoid larvae. Following ingestion of the copepod by a suitable second intermediate host, typically a minnow or other small freshwater fish, the procercoid larvae are released from the crustacean and migrate into the fish’s flesh where they develop into a plerocercoid larvae (sparganum). The plerocercoid larvae are the infective stage for the definitive host (including humans).
Because humans do not generally eat undercooked minnows and similar small freshwater fish, these do not represent an important source of infection. Nevertheless, these small second intermediate hosts can be eaten by larger predator species, for example, trout, perch, and walleyed pike. In this case, the sparganum can migrate to the musculature of the larger predator fish and mammals can acquire the disease by eating these later intermediate infected host fish raw or undercooked. After ingestion of the infected fish, the plerocercoids develop into immature adults and then into mature adult tapeworms which will reside in the small intestine. The adults attach to the intestinal mucosa by means of the two bilateral grooves (bothria) of their scolex. The adults can reach more than 10 m (up to 30 ft) in length in some species such as D. latum, with more than 3,000 proglottids. One or several of the tape-like proglottid segments (hence the name tape-worm) regularly detach from the main body of the worm and release immature eggs in fresh water to start the cycle over again. Immature eggs are discharged from the proglottids (up to 1,000,000 eggs per day per worm) and are passed in the feces. The incubation period in humans, after which eggs begin to appear in the feces is typically 4–6 weeks, but can vary from as short as 2 weeks to as long as 2 years. The tapeworm can live up to 20 years.

Life cycle of D. latum.
Clinical symptoms, including occasional parasite-induced B12 deficiency
Symptoms of diphyllobothriasis are generally mild, and can include diarrhea, abdominal pain, vomiting, weight loss, fatigue, constipation and discomfort. Approximately four out of five cases are asymptomatic and may go many years without being detected. In a small number of cases, this leads to severe vitamin B12 deficiency due to the parasite absorbing 80% or more of the host’s B12 intake, and a megaloblastic anemia indistinguishable from pernicious anemia. The anemia can also lead to subtle demyelinative neurological symptoms (subacute combined degeneration of spinal cord). Infection for many years is ordinarily required to deplete the human body of vitamin B-12 to the point that neurological symptoms appear.
Treatment
The standard treatment for diphyllobothriasis, as well as many other tapeworm infections is a single dose of Praziquantel, 5–10 mg/kg PO once for both adults and children. An alternative treatment is Niclosamide, 2 g PO once for adults or 50 mg/kg PO once. One should note that Praziquantel is not FDA approved for this indication and Niclosamide is not available for human use in the United States. Another interesting potential diagnostic tool and treatment is the contrast medium, Gastrografin, introduced into the duodenum, which allows both visualization of the parasite, and has also been shown to cause detachment and passing of the whole worm.
Beef tapeworm (Taenia saginata or Taeniarhynchus saginata)
Taenia saginata, also known as Taeniarhynchus saginata, or the beef tapeworm, is part of the order Cyclophyllidea and is a parasite of both cattle and humans, causing taeniasis in humans. Taenia saginata occurs where cattle are raised by infected humans maintaining poor hygiene, human feces are improperly disposed of, meat inspection programs are poor, and where meat is eaten without proper cooking. The disease is found worldwide but is relatively common in Africa, some parts of Eastern Europe, Southeast Asia, and Latin America.
T. saginata is normally 4 m to 10 m in length, but can become very large, over 12 m long in some situations. Like all other cestodes, T. saginata is flattened dorso-ventrally and segmented. The body consists of three portions:scolex, neck and strobila. The body is whitish in colour, divided into the anterior unarmed scolex. Armature is not needed on the scolex since there are four suckers present but no hooks. The neck is the shortest part of the body. It consists of immature segments called proglottids. The strobila is made of mature proglottids that eventually lead to the gravid proglottids. T. saginata is the largest of genus Taenia, consisting between 1000 to 2000 proglottids, and can also have a lifespan of 25 years in a host’s intestine. The mature proglottid contains the tubular unbranched uterus, ovary, genital pore, testes, and vitelline gland. It does not have a digestive system, mouth, anus, or digestive tract. It is also an acoelomate, meaning it does not have a body cavity. In the gravid proglottid, the uterus contains up to 15 side branches filled with eggs. The gravid segments detach and the eggs are released. Each of these segments can act as a worm. When they dry up, the proglottid ruptures, and the eggs are released. The egg can only infect cattle, the intermediate host. Inside the cow’s duodenum, the oncosphere hatches with the help of the gastric and intestinal secretions, and migrates through the blood to the muscle. There it develops into infective cysticercoid cysticerci.
The life cycle is indirect and complicated, and is completed in humans as the definitive host and cattle as the intermediate host. Cattle will eat the eggs and the oncospheres will hatch in the duodenum under the influence of gastric juices. It will envaginate into the intestinal walls and travel via the general circulatory system. The embryos will disseminate all over the body and develop cysticercus in striated muscles of the cow within 70 days. Humans contract T. saginata by eating raw or undercooked meat containing larvae. It takes about 5 to 12 weeks for the worm to mature into adulthood in the human intestine. Usually only a single worm is present at at time. However, multiple worms have been known to inhabit the human body.The larvae gets digested out of the beef in the human intestinal system. The worm then attaches on the intestinal mucosa of the upper small intestine by the scolex. Fertilized eggs are released through the faeces along with the gravid proglottid which gets detached from the strobila. Cattle ingest the infective embryo while grazing. The digestive enzymes will break the thick shell of the egg and allow formation of the zygotes called “oncospheres”. These zygotes then penetrate the mucous layer of the digestive tract and enter the circulation of the host. This is where the young larval stages form a pea-sized, fluid filled cyst, also known as “Cysticercus bovis” and these cysts seem to form in the muscular fibers and are sometimes seen in specific organs like the lungs and liver. The digestive enzymes break down the cysticercus and the larval cyst is released and the inverted scolex is able to come out and attach to the host’s intestine. Proglottids are motile and will shed eggs as it moves. These eggs (containing the oncosphere) can remain viable for several days to weeks in sewage, rivers, and pastures.
Humans are the only definitive hosts of this worms, and they acquire the infection by eating the undercooked flesh of the cow, the common intermediate host. The infection is usually symptomless but may cause great anxiety to the patient, as the detached, whitish-yellow, opaque segments are motile and may emerge spontaneously from the anus. Infection is common in tropical countries.

The life cycle of Taenia saginata
T. saginata is normally 4 m to 10 m in length, but can become very large, over 12 m long in some situations. Like all other cestodes, T. saginata is flattened dorso-ventrally and segmented. The body consists of three portions:scolex, neck and strobila. The body is whitish in colour, divided into the anterior unarmed scolex. Armature is not needed on the scolex since there are four suckers present but no hooks. The neck is the shortest part of the body. It consists of immature segments called proglottids. The strobila is made of mature proglottids that eventually lead to the gravid proglottids. T. saginata is the largest of genus Taenia, consisting between 1000 to 2000 proglottids, and can also have a lifespan of 25 years in a host’s intestine. The mature proglottid contains the tubular unbranched uterus, ovary, genital pore, testes, and vitelline gland. It does not have a digestive system, mouth, anus, or digestive tract. It is also an acoelomate, meaning it does not have a body cavity. In the gravid proglottid, the uterus contains up to 15 side branches filled with eggs. The gravid segments detach and the eggs are released. Each of these segments can act as a worm. When they dry up, the proglottid ruptures, and the eggs are released. The egg can only infect cattle, the intermediate host. Inside the cow’s duodenum, the oncosphere hatches with the help of the gastric and intestinal secretions, and migrates through the blood to the muscle. There it develops into infective cysticercoid cysticerci.

Taenia saginata

Taenia saginata proglottid stained to show uterine branches. The pore on the side identifies T. saginata as a cyclophyllid cestode.
Diagnosis
The basic diagnosis is done from a stool sample. Feces are examined to find parasite eggs. The eggs look like other eggs from the family Taeniidae, so it is only possible to identify the eggs to the family, not to the species level. Since it is difficult to diagnose using eggs alone, looking at the scolex or the gravid proglottids can help identify it as Taenia saginata. Proglottids sometimes trickle down the thighs of infected humans and are visible with unaided eye, so can aid with identification. Observation of scolex help distinguish between T. saginata, T. solium and T. asiatica. When the uterus is injected with India ink, its branches become visible. Counting the uterine branches enables some identification (Taenia saginata uteri have 12 or more branches on each side, while other species such as Taenia solium only have five to 10).
Differentiation of the species from other species of Taenia, such as T. solium and T. asiatica, is notoriously difficult because of their close morphological resemblance, and their eggs are more or less identical. Identification often requires histological observation of the uterine branches and PCR detection of ribosomal 5.8S gene. T. saginata’s uterus stems out from its center to form 12 to 20 branches, but in contrast to its closely related Taenia species, the branches are much less iumber and comparatively thicker; in addition, the ovaries are bilobed and testes are twice as many.
Eosinophilia and elevated IgE levels are chief hematological findings. Also Ziehl–Neelsen stain can be used to differentiate between mature Taenia saginata and Taenia soium, in most cases Taenia saginata will stain while Taenia solium will not, however the method is not strict.
Pork tapeworm (Taenia solium)
Taenia solium, also called the pork tapeworm, is a cyclophyllid cestode in the family Taeniidae. It infects pigs and humans in Asia, Africa, South America, parts of Southern Europe and pockets of North America. In the larval stage, it causes cysticercosis, which is a major cause of epilepsy in humans. Like all cyclophyllid cestodes, T. solium has four suckers on its scolex (“head”). T. solium also has two rows of three hooks.

Scolex of Taenia solium
Description
T. solium , commonly known as a tapeworm, is a triploblastic acoelomate. It is normally 2 to 3 m in length, but can become very large, over 50 m long in some situations.
T. solium has a very similar life cycle to Taenia saginata. Cysticerci have three morphologically distinct types. The common one is the ordinary “cellulose” cysticercus, which has a fluid-filled bladder 0.5 cm to 1.5 cm in length and an invaginated scolex. The intermediate form has a scolex, while the “racemose” has no evident scolex but is believed to be larger and much more dangerous. They are 20 cm in length and have 60 ml of fluid, and 13% of patients might have all three types in the brain. Humans are usually infected through eating infected pork, fostering adult tapeworms in the intestine, and passing eggs through feces, but autoinfection is also possible. In that case, a cysticercus (a larva sometimes called a “bladder worm”) develops in the human, who acts as an intermediate host. This happens if eggs get to the stomach, usually as a result of contaminated hands, but also due to retroperistalsis. Cysticerci often occur in the central nervous system, which can cause major neurological problems, such as hydrocephalus, paraplegy, meningitis, convulsions and even death. The condition of having cysticerci in one’s body is called cysticercosis.
Eggs can be diagnosed only to the family level, but if a proglottid‘s uterus is stained with India ink, the number of visible uterine branches can help identify the species; unlike the Taenia saginata uteri, T. solium uteri have only five to 10 uterine branches on each side.
Infection with T. solium adults is treated with niclosamide, which is one of the most popular drugs for adult tapeworm infections, as well as for fluke infections. As cysticercosis is a major risk, it is important to wash one’s hands before eating and to suppress vomiting if a patient may be infected with T. solium. If neurocysticercosis occurs, the drug of choice is either albendazole or praziquantel. These drugs damage the parasites’ skin internally, causing it to disintegrate and is then removed by the host’s immune system.
Infection may be prevented with proper disposal of human feces around pigs, cooking meat thoroughly and/or freezing the meat at −10°C for 5 days. Most cases occur because infected food handlers contaminate the food.
Humans are the only definitive hosts, and they acquire the infection by eating undercooked “measly” pork or raw pork sausages. The adult worm infection usually causes no symptoms other than vague abdominal complaints.
Epidemiology
T. solium is found worldwide, but is more common in cosmopolitan areas. Because pigs are intermediate hosts of the parasite, completion of the life cycle occurs in regions where humans live in close contact with pigs and eat undercooked pork. Cysticercosis is often seen in areas where poor hygiene allows for contamination of food, soil or water supplies. Prevalence rates in the United States have shown immigrants from Mexico, Central and South America and Southeast Asia account for most of the domestic cases of cysticercosis. Taeniasis and cysticercosis are very rare in predominantly Muslim countries, as Islam forbids the consumption of pork. Human cysticercosis is acquired by ingesting T. solium eggs shed in the feces of a human tapeworm carrier via gravid proglottids, so can occur in populations that neither eat pork nor share environments with pigs, although the completion of the life cycle can occur only where humans live in close contact with pigs and eat pork.
In 1990 and 1991, four unrelated members of an Orthodox Jewish community in New York City developed recurrent seizures and brain lesions, which were found to have been caused by T. solium. In keeping with their religion, none of the patients ate pork; additionally, none had any history of recent foreign travel. Several immediate family members of these four patients with seizures were found to have cysticercus antibodies. The families of the four patients had all employed housekeepers from Latin American countries, and one of the housekeepers tested positive for cysticercus antibodies, leading to the conclusion that the housekeepers were the most likely source of the infections.

Stained T. solium proglottid
Life cycle
This infection is caused by ingestion of eggs shed in the feces of a human tapeworm carrier. Pigs and humans become infected by ingesting eggs or gravid proglottids. Humans are infected either by ingestion of food contaminated with feces containing eggs, or by autoinfection. In the latter case, a human infected with adult T. solium can ingest eggs produced by that tapeworm, either through fecal contamination or, possibly, from proglottids carried into the stomach by reverse peristalsis. Once eggs are ingested, oncospheres hatch in the intestine, invade the intestinal wall, and migrate to striated muscles, as well as the brain, liver, and other tissues, where they develop into cysticerci. In humans, cysts can cause serious sequelae if they localize in the brain, resulting in neurocysticercosis. The parasite life cycle is completed, resulting in human tapeworm infection, when humans ingest undercooked pork containing cysticerci. Cysts evaginate and attach to the small intestine by their scolices. Adult tapeworms develop, (up to 2 to 7 m in length and produce less than 1000 proglottids, each with approximately 50,000 eggs) and reside in the small intestine for years.
Life cycle of T. solium
Pathogenesis
Ingestion of T. solium eggs or proglottid rupture within the host intestine can cause larvae to migrate into host tissue and cause cysticercosis. This is the most frequent and severe disease caused by T. solium. In symptomatic cases, a wide spectrum of symptoms may be expressed, including headaches, dizziness and occasional seizures. In more severe cases, dementia or hypertension can occur due to perturbation of the normal circulation of cerebrospinal fluid. (Any increase in intracranial pressure will result in a corresponding increase in arterial blood pressure, as the body seeks to maintain circulation to the brain.) The severity of cysticercosis depends on location, size and number of parasite larvae in tissues, as well as the host immune response. Other symptoms include sensory deficits, involuntary movements, and brain system dysfunction. In children, ocular location of cysts is more common than cystation in other locations of the body. Heavy infection with T. solium can lead to neurocysticercosis, which can lead to epilepsy, seizures, lesions in the brain, blindness, tumor-like growths, and low eosinophil levels.
Diagnosis and treatment
Infection with beef or pork tapeworms is diagnosed by the identification of the segments or ova in faeces.
Differentiation between the two can only be made by examining the morphology of the head (scolex) or egg-bearing segments (proglottids)

Taenia solium adult
All intestinal tapeworms are readily destroyed by niclosamide (Yomesan). A saline purge 1 hour after treatment should be given in T. solium to prevent regurgitation of eggs into the stomach, which may lead to cysticercosis. Occasionally, worms are not eradicated, ova or segments reappear in the faeces and retreatment is necessary. Identification of the head in the faeces after treatment confirms cure.
Prevention. Measures include the treatment of human cases, treatment of raw sewage, inspection of meat and pork in slaughterhouses, adequate cooking of fish, beef and pork, deep-freezing which kills the larval worms.
Intestinal nematodes (Roundworms)
The phylum Nematoidea, or round worms, is the second largest phylum in the animal kingdom, encompassing as many as 500.000 species. Members of this phylum are elongated, with bilaterally symmetric bodies containing an intestinal tract and a large body cavity. Few of them are parasites of humans. The life cycle of parasitic nematodes is important clinically because some of these infections can be transmitted directly from infected to uninfected people whereas in others eggs must undergo a process of maturation outside the human host and in a third category the parasites may spend a part of their life cycle in the soil before becoming infective to humans.
Enterobiasis (Enterobius vermicularis)
A pinworm infection or enterobiasis is a human parasitic disease and one of the most common parasitic worm infections in the developed world. It is caused by infestation of the parasitic roundworm Enterobius vermicularis, commonly called the human pinworm. Infection usually occurs through the ingestion of pinworm eggs, either through contaminated hands, food, or less commonly, water. The chief symptom is itching in the anal area. The incubation time from ingestion of eggs to the first appearance of new eggs around the anus is 4 to 6 weeks. Pinworms are usually considered a nuisance rather than a serious disease. Treatment is straightforward in uncomplicated cases, however, elimination of the parasite from a family group or institution often poses significant problems—either due to an incomplete cure or reinfection.
Worldwide prevalence, this is the most common worm infection, usually affecting children. Often several members of household of institution are infected.
Pinworms (Enterobius vermicularis)
Cycle of infection
Adult worms are present in the colon and rectum, from where the gravid female emerges at night to deposit eggs in the perianal skin. These eggs are then carried by the hands, clothing or dust to be ingested by the same person or by new hosts. Swallowed eggs change to larvae in the intestine, maturing into adults which than breed, completing the cycle in about 1 month.
Clinical features and diagnosis
One third of individuals with pinworm infection are totally asymptomatic. The main symptoms are pruritus ani and perineal pruritus, i.e., itching in and around the anus and around the perineum. The itching occurs mainly during the night, and is caused by the female pinworms migrating to lay eggs around the anus. Both the migrating females and the clumps of eggs are irritating, but the mechanisms causing the intense pruritus have not been explained. The intensity of the itching varies, and it can be described as tickling, crawling sensations, or even acute pain. The itching leads to continuously scratching the area around the anus, which can further result in tearing of the skin and complications such as secondary bacterial infections, including bacterial dermatitis (i.e., skin inflammation) and folliculitis (i.e., hair follicle inflammation). General symptoms are insomnia (i.e., persistent difficulties to sleep) and restlessness. A considerable proportion of children suffer from loss of appetite, weight loss, irritability, emotional instability, and enuresis (i.e., inability to control urination).
Pinworms cannot damage the skin, and they do not normally migrate through tissues. However, in women they may move onto the vulva and into the vagina, from there moving to external orifice of the uterus, and onwards to the uterine cavity, fallopian tubes, ovaries, and peritoneal cavity. This can cause vulvovaginitis, i.e. an inflammation of the vulva and vagina. This causes vaginal discharge and pruritus vulvae, i.e., itchiness of the vulva. The pinworms can also enter the urethra, and presumably, they carry intestinal bacteria with them. According to Gutierrez (2000), a statistically significant correlation between pinworm infection and urinary tract infections has been shown, however Burkhart & Burkhart (2005) maintain that the incidence of pinworms as a cause of urinary tract infections remains unknown. Incidentally, one report indicated that 36% of young girls with urinary tract infection also had pinworms. Dysuria (i.e., painful urination) has been associated with pinworm infection.
Pinworm life cycle.
The relationship between pinworm infestation and appendicitis has been researched, but there is a lack of clear consensus in the matter: while Gutierres (2005) maintains that there exists a consensus that pinworms do not produce the inflammatory reaction, Cook (1994) states that it is controversial whether pinworms are causatively related to acute appendicitis, and Burkhart & Burkhart (2004) state that pinworm infection causes symptoms of appendicitis to surface.
Perianal itching during egg deposition is the only symptom; white, slightly motile, gravid female thread-like worms may be visible in the faeces. “Persisting” or relapsing infections are always due to reinfection, as adult worms can live only for 6 weeks. Confirmation is by microscopic demonstration of trapped eggs on a sticky cellophane tape applied to the perianal skin in early morning and then placed on a glass slide.
Diagnosis
Diagnosis depends on finding the eggs or the adult pinworms. Individual eggs are invisible to the naked eye, but they can be seen using a low-power microscope. On the other hand, the light-yellowish thread-like adult pinworms are clearly visually detectable, usually during the night when they move near the anus, or on toilet paper. Transparent adhesive tape (e.g. Scotch Tape) applied on the anal area will pick up deposited eggs, and diagnosis can be made by examining the tape with a microscope. This test is most successful if done every morning for several days, because the females do not lay eggs every day, and the number of eggs vary.
Pinworms do not lay eggs in the feces, but sometimes eggs are deposited in the intestine. As such, routine examination of fecal material gives a positive diagnosis in only 5 to 15% of infected subjects, and is therefore of little practical diagnostic use. In a heavy infection, female pinworms may adhere to stools that pass out through the anus, and they may thus be detected on the surface on the stool. Adult pinworms are occasionally seen during colonoscopy. On a microscopic level, pinworms have an identifying feature of alae (i.e., protruding ridges) running the length of the worm.
High magnification micrograph of a pinworm in cross section in the appendix.
Prevention
Pinworm infection cannot be totally prevented under most circumstances. This is due to the prevalence of the parasite and the ease of transmission through soiled night clothes, airborne eggs, contaminated furniture, toys and other objects. Infection may occur in the highest strata of society, where hygiene and nutritional status are typically high. The stigma associated with pinworm infection is hence considered a possible over-emphasis. Counselling is sometimes needed for upset parents that have discovered their children are infected, as they may not realize how prevalent the infection is.
Preventative action revolves around personal hygiene and the cleanliness of the living quarters. The rate of reinfection can be reduced through hygienic measures, and this is recommended especially in recurring cases. The main measures are keeping fingernails short, and washing and scrubbing hands and fingers carefully, especially after defecation and before meals. Under ideal conditions, bed covers, sleeping garments, and hand towels should be changed daily. Simple laundering of clothes and linen disinfects them. Children should wear gloves while asleep, and the bedroom floor should be kept clean. Food should be covered to limit contamination with dust-borne parasite eggs. Household detergents have little effect on the viability of pinworm eggs, and cleaning the bathroom with a damp cloth moistened with an antibacterial agent or bleach will merely spread the still-viable eggs. Similarly, shaking clothes and bed linen will detach and spread the eggs.
Treatment
Medication is the primary treatment for pinworm infection. The existing pharmaceutical drugs against pinworms are so effective that many medical scientists regard hygienic measures as impractical. However, reinfection is frequent regardless of the medication used. Total elimination of the parasite in a household may require repeated doses of medication for up to a year or more. Because the drugs kill the adult pinworms, but not the eggs, the first retreatment is recommended in two weeks. Also, if one household member spreads the eggs to another, it will be a matter of two or three weeks before those eggs become adult worms and thus amenable to treatment. Asymptomatic infections, often in small children, can serve as reservoirs of infection, and therefore the entire household should be treated regardless of whether or not symptoms are present.
The benzimidazole compounds albendazole (brand names e.g., Albenza, Eskazole, Zentel and Andazol) and mebendazole (brand names e.g., Ovex, Vermox, Antiox and Pripsen) are the most effective. They work by inhibiting the microtubule function in the pinworm adults, causing glycogen depletion, thereby effectively starving the parasite. A single 100 milligram dose of mebendazole with one repetition after a week, is considered the safest, and is usually effective with cure rate of 96%. Mebendazole has no serious side effects, although abdominal pain and diarrhea have been reported. Pyrantel pamoate (also called pyrantel embonate, brand names e.g., Reese’s Pinworm Medicine, Pin-X, Combantrin, Anthel, Helmintox, and Helmex) kills adult pinworms through neuromuscular blockade, and is considered as effective as the benzimidazole compounds. Other medications are piperazine, which causes flaccid paralysis in the adult pinworms, and pyrvinium pamoate (also called pyrvinium embonate), which works by inhibiting oxygen uptake of the adult pinworms. Pinworms located in the genitourinary system (in this case, female genital area) may require other drug treatments.
Garlic has been treatment used as a natural antibiotic throughout history in the ancient cultures of China, India, Egypt, and Greece. Hippocrates (459–370 BC) mentioned garlic as a remedy against intestine parasites. German botanist Lonicerus (1564) recommended garlic against parasitic worms. The action of garlic is manifold. Because of allicin and other sulfur compounds, garlic has antibiotic, antibacterial and antimycotic action, which has been testified by in vitro studies. It can be concluded that administration of garlic should not be avoided; on the contrary, its intake should be as much as possible. Crushed garlic cloves and tea tree oil mixture can be applied (over isolation layer like vaseline) to the anus to cessate itching.
Strongyloidiasis (Strongyloides stercoralis)
http://emedicine.medscape.com/article/229312-overview
This small roundworm is found in all tropical and subtropical countries. It has two distinctive life cycles. In humans, the cycle is similar to that of hookworm, except that the female parasites is parthenogenetic. Also, ova mature into larvae within the intestine rather than outside. This may lead to autoinfection. Free-living life cycle in soil, involving both adult male and female parasite.
Clinical features, diagnosis
Often asymptomatic, but in some cases larvae may penetrate the skin around the anus producing urticarial skin eruption and migratory serpiginous rash extending rapidly over the thighs and trunk (larva currans). In immunocompromised hosts, intestinal autoinfection may lead to heavy worm-load, causing chronic diarrhoea and malabsorbtion; also disseminated disease with wasting and pulmonary involvement may develop, which may be fatal. Eosinophilia is common during visceral migration and in chronic infection. Diagnosis is by demonstration larvae in fresh stools, duodenal aspirate or sputum (rarely).
Tissue nematodes
The tissue dwelling roundworms constitute a major global health problem. They are widely scattered around the world, especially in the tropics, and infect millions of people. Some are parasites of humans only, while others have an animal reservoir. All these parasites have complex life cycles involving arthropod intermediate hosts except for Trichinella spiralis, which is transmitted directly from one host to the next by ingestion of infective larvae.
Trichiniasis
http://hairremoval.ygoy.com/2010/04/29/what-is-trichiasis/
This is a disease caused by the larvae of nematode Trichinella spiralis, which infect and reside in the flesh, as encysted larvae, of a wide range of animals including domestic pigs, rats and wild animals. Ingestion of infected flesh leads to liberation of these larvae which mature into adults within the small intestinal mucosa. Breeding and larval production invasion of flesh then follow. Undercooked pork wild animal-meat is the main sources of human infection. There is a variable incidence worldwide dependent on animal rearing/feeding practices and wildlife meat eating.
Clinical features, diagnosis and treatment
Initially there is abdominal pain and diarrhea (during larval migration into intestinal mucosa), followed by systemic larval invasion. 1 week later muscle and joint pains and fever occur. After recovery, the visceral larvae are absorbed but the encysted muscle larvae may calcify after several years. Intense eosinophilia is common during the acute stage. Serology is positive by the 3rd week. Muscle biopse will show the encysted worms, often in considerable numbers. Corticosteroids during the acute stage help, and thiabendazole is often used to kill the larvae.

