General characteristics of maxillofacial apparatus and their classification. Transportation splints. Ligature binding teeth, indications, contraindications. Possible mistakes and complications.
Injuries to Facial and Oral Structures
When soft tissue injuries such as lacerations occur in the mouth or on the face, they are typically repaired using sutures (stitches). In addition to our goal of the best cosmetic result possible, care is taken to make sure any functional problems of the mouth and teeth are addressed.
Fractures of the bones of the jaws and face are treated in a manner similar to the fractures in other parts of the body. Simple jaw fractures can be stabilized or splinted by wiring the jaws together. More severe fractures of the jaw require placement of small bone plates to stabilize the bones. This allows you to return to normal function more quickly.

Injuries to the Teeth
Injuries to teeth are quite common and can usually be treated in our office, avoiding the inconvenience and cost of an emergency room visit.
If teeth are displaced or loosened, they are carefully repositioned and stabilized with wires attached to adjacent teeth.
If a permanent tooth is avulsed (knocked out) it should immediately be placed in cold milk, or better yet, back into the socket – the sooner the better for the survival of the tooth. Call our office immediately. If injured teeth cannot be saved, dental implants are the best choice for replacement.
A high percentage of tooth injuries in sports can be prevented by the use of a properly fitted mouthguard. The boil-and-bite mouthguards available at sporting goods stores are better than nothing, but the custom fitted appliance from your dentist offers the best protection and breathing during sports.
Transport immobilization
|
Stiff head-chin strap by D.O.Entin. The main standard bandage by Y.M.Zbarzh |
The chin cup is fixed with the help of rubber rings to the head cup. |
|
|
applying gauze bandage for wounds. |
Cross-course bandage in frontoparietal area, primary applying bandage before and behind the ears. |
In case of lower jaw fractures one caot applytightening dressingas it may cause additional displacement of fractions and the threat of suffocation. |
|
ligature binding of jaws(take off no longer than 3-5 days). |
The presence of the at least two standing teeth on the fractions of the jaw |
Contraindications: the threat of asphyxia, bleeding from the mouth, vomiting. |
|
By Ivy` |
A wire(aluminum-bronze 0,5-0,7 mm, 12-15 sm length) is bent pin-like, twisted forming a loop. Put both ends into interdental space. Separatetheends so that theyseizetheadjacent teeth, and take them out. The distal end is traced through the loop and both ends get twisted. In the antagonist teeth the wire is passed through the loop and gets twisted. |
The wire is twisted clockwise |
|
By Limberg |
With a wire of 5-6 sm length one tooth gets twisted. Twists of the upper and lower ligature are twisted together. Ends are cut off and bent medially, not traumatizing mucosa. |
|
Cosmetic Jaw Surgery
Orthognathic (Jaw) Surgery
This implies surgery to straighten the jaws. Cases are planned with an Orthodontist who treats the frequent malocclusion present in such a way that the dental occlusion will be correct following the surgical procedure.
Presurgical orthodontic treatment often involves fixed brace treatment lasting
18-24 months, and is essential for the stability of the result.
Invisible Orthodontics
At NCAFOS Clinics we shall have access to “invisible” brace treatment which is suitable for some patients. This is carried out using fix braces placed on the tongue (lingual) sides of the teeth or by using a series of transparent dental splints (Invisalign®) http://www.invisalign.com/GB/index.html which fit over the teeth like a boxers gum shield.
At the end of an average of 12 – 18 months of orthodontic treatment, the surgical plan is confirmed with computer analysis of skull x-rays. Digital photographs are manipulated on screen (Photomorphanalysis) to predict the cosmetic appearance following surgery to one or both jaws (osteotomy).
Surgical (Instant) Orthodontics
An osteotomy is a controlled surgical fracture of bone, and is usually carried out with saws and instruments which can split the bone along its natural “grain”. Combined with Invisible Orthodontic treatment, and planned using Engineering Assisted Surgery techniques and customised jigs, precision osteotomy bone cuts between the tooth roots may be used to mobilise teeth so that they may be orthodontically moved into the correct position using treatment lasting a few days or weeks – instead of months or years. This concept is a major breakthrough in the treatment of misaligned teeth.
Computer Simulated Segmental Osteotomy
illustrating the mobilisation of two lower teeth
Jaw Surgery (Osteotomy) Procedures
a) Mandibular Sagittal Split Osteotomy
The back of the lower jaw is split bilaterally under general anaesthetic in the region of the wisdom teeth, which are generally removed in a separate operation at least 6 months prior to corrective surgery.
The procedure is carried out in about 1.5 hours and permits the lower jaw to be advanced or pushed back with adequate bone contact for healing.
The bone is fixed in its new position by screws which are inserted through tiny external skin incisions which are located at the angle of the jaw. These heal with minimal external scarring.
Mandibular Sagittal Split Osteotomy and Genioplasty (Chin Surgery)
The mandible has been pushed backwards and surgery has been carried out to the chin (Genioplasty)Sensory Nerves to the lower lip pass through the jaw and are coloured blue
Whilst day case treatment is practiced in the USA, it is common practice in the UK to spend one night as an in-patient.
Some adjustment to the position of the dental occlusion (bite) is not uncommon following surgery. This is achieved by joining the upper and lower jaws together with elastic band traction for a week or two.
Facial swelling is variable and is controlled with intravenous steroid injections over the first 24 hours. Patients require a liquidised diet if the jaws are held together with elastics – or soft diet for the first two weeks, after which time more solid food can be introduced.
Specific Complications:
The Mandibular Sagittal Split Osteotomy
The sensory nerves to the lower lip are coloured blue
Screw fixation is demonstrated on one side. Screws are placed above and below the nerve
Sensory Nerves
The sensory nerve to the lower lip (inferior dental nerve) runs in the lower jaw in the region of the osteotomy bone cuts. Immediately following the surgery all patients should expect numbness of the lower lip, which improves over a period of months. A degree of permanent altered sensation remains in about 30% of patients and affects one or both sides of the lower lip. This may range from complete numbness as experienced with a dental injection to mild tingling. Male patients may not feel if they cut themselves whilst shaving. The majority of patients, who experience permanent altered sensation to the lower lip, find that it is of little significance, and have no regrets about surgery. Reports of psychological problems and or depression related to sexual activity and altered/reduced pleasure from kissing in particular have been reported but are rare. Similarly the condition of painful numbness (dysthesia) has been reported but is rare. Repair of an injured inferior dental nerve is possible but technically difficult. Such a repair is not guaranteed to restore normal sensation.
The sensory nerve to the tongue lies close to the osteotomy cuts in the soft tissue and is retracted away from the operation site. Altered sensation associated with this traction is rare and usually temporary.
Motor Nerves
Motor nerves are nerve that make muscles contract. Injury to the facial nerve supplying movement for the lower lip has been reported as a result of insertion of screws through the small external skin incisions. This may produce some weakness of the lower lip – more noticeable on smiling and may be permanent. This is a very rare complication.
Relapse
Long term complications include relapse, which may occur if the jaw is advanced or if the jaw is retracted. The cause is controversial. It is thought to be related to continued growth in some patients – seen when the jaw is pushed back, and muscle pull – when the jaw is advanced large distances to accentuate a small chin. It is therefore important to carry out such operations when growth has ceased. Muscles inserted into the chin may be divided in the floor of mouth in cases of large jaw advancement – circa 1cm (myotomy). The majority of cases of relapse are noticed by slight changes in the dental occlusion only noticed by the clinician. It is very rare for relapse to adversely affect the cosmetic improvement achieved.
Chin Surgery – Genioplasty
The position of the chin is critical and influences the facial height, facial centre-lines and cosmetic appearance of the nose. Patients seeking rhinoplasty may discover that their perceived cosmetic problem lies elsewhere – the chin. The effect of both rhinoplasty and/or genioplasty may be demonstrated to the patient on screen during the initial consultation using computer technology.
The chin may be moved backward / forwards / upwards / downwards with an intraoral incision behind the lower lip, to correct an abnormal position. It may also be moved to the facial centre line in cases of facial asymmetry.
Post surgery a pressure dressing is applied to the chin for about 72 hours. This reduces bruising which may sometimes travel down the tissue planes into the neck and even onto the chest. Such bruising is not necessarily related to surgical technique and may be related to a tendency for blood vessels to ooze following surgery.
c) Liposuction and Liposculpture
A “double chin” is a common feature and may be treated alone or in combination with the chin and lower jaw. Liposuction may be carried out through a tiny skin incision under the chin. The removal of fatty tissue is carried out using suction (Liposuction) which may be carried out laterally in the neck to provide a better jaw line and for the treatment of jowling (Liposculpture), through additional skin incisions near the angle of the jaw.
The effects pf liposuction / liposculpture may be simulated on screen with computer technology at the time of initial consultation.
d) Upper Jaw – Maxilla
Maxillary osteotomy surgery may be advised when an abnormally positioned jaw is giving rise to cosmetic problems. The jaw can be moved upwards / downwards / forwards and rarely backwards.
The critical aspect of where to place the maxilla in the anteroposterior plane is determined by computer analysis of skull x-rays and computer simulation using digital photography (photomorphanalysis™). This illustrates the movement and its permits effect on other structures to be calculated e.g. the nose.
The position of the maxilla in the vertical plane is determined by the amount of upper incisor tooth visible below the upper lip at rest and when smiling.
Rotation of the maxilla may be required on occasion to centralise the position of the front teeth. This has a temporary effect on the central position of the nose, which initially looks “off centre” – this usually corrects itself over a 3 month period.
Surgery to the maxilla is carried out at three levels named after a French Surgeon Renй Le Fort.
Le Fort I Osteotomy
Sensory nerves to the upper lip and cheeks are coloured blue
The Le Fort I osteotomy involves separating the maxilla and the palate from the skull above the roots of the upper teeth through an incision inside the upper lip. The maxilla is fixed in its new position with titanium screws and plates. Surgery time is around three hours. The operation is frequently carried out with the mandibular Sagittal split osteotomy when it is termed a Bimaxillary Osteotomy.
Bimaxillary osteotomies take around five hours to complete and may be carried out in conjunction with chin surgery and liposuction/liposculpture. Blood transfusion is required. On occasions bone grafting is required in the Le Fort I osteotomy to ensure bone healing and union across the bone cuts. The graft is frequently harvested from the hip. Bone graft material may be harvested from the chin or lower jaw in bimaxillary cases – leaving the hip intact.
Cosmetic improvement is startling for those individuals requiring these procedures, and with proper planning it is unusual for patients not to be delighted with outcome.
Le Fort II Osteotomy
Sensory nerves to the cheeks and forehead are coloured blue
The Le Fort II Osteotomy is an uncommon procedure used when there has been a problem with growth in the centre of the face and the upper jaw and nose requires movement together. This is a major surgical operation, and involves incisions in the mouth, cosmetic incisions behind the lower eyelids (transconjunctival) or through the skin below the lower eyelids (blepharoplasty). The nose is approached with a cosmetic incision over the top of the head from ear to ear (bicoronal approach) and the scalp is raised forwards to get access to the nasal bones. Sensory nerves to the forehead require to be freed from bony canals (illustrated). Hip grafts (illustrated in red) are needed to fill in any gaps after the upper jaw and nose have been moved (usually forwards).
Surgery time is around 8 hours; blood transfusions are required and the patient is nursed in a high dependency unit overnight following the operation. Suction drains are placed in the scalp to reduce bruising. Patients may have considerable facial swelling and black eyes following this procedure. Aesthetic improvement is startling for those patients requiring this type of surgery.
Le Fort III Osteotomy
The Le Fort III Osteotomy is used to correct generalised growth failure of the midface involving the upper jaw nose and cheek bones (zygomas). The surgical approach and post operative management is similar as for the Le Fort II procedure. Brow lift procedures may be carried out at the same time as Le Fort II and Le Fort III osteotomies.
Le Fort III Osteotomy lateral view
The lateral view of the Le Fort III osteotomy illustrates the use of an additional plate and bone grafting in the region of the Zygomatic arch.
Mandible fractures are a frequent injury because of the mandible’s prominence and relative lack of support. As with any facial fracture, consideration must be given for the need of emergency treatment to secure the airway or to obtain hemostasis if necessary before initiating definitive treatment of the fracture.
History of the Procedure
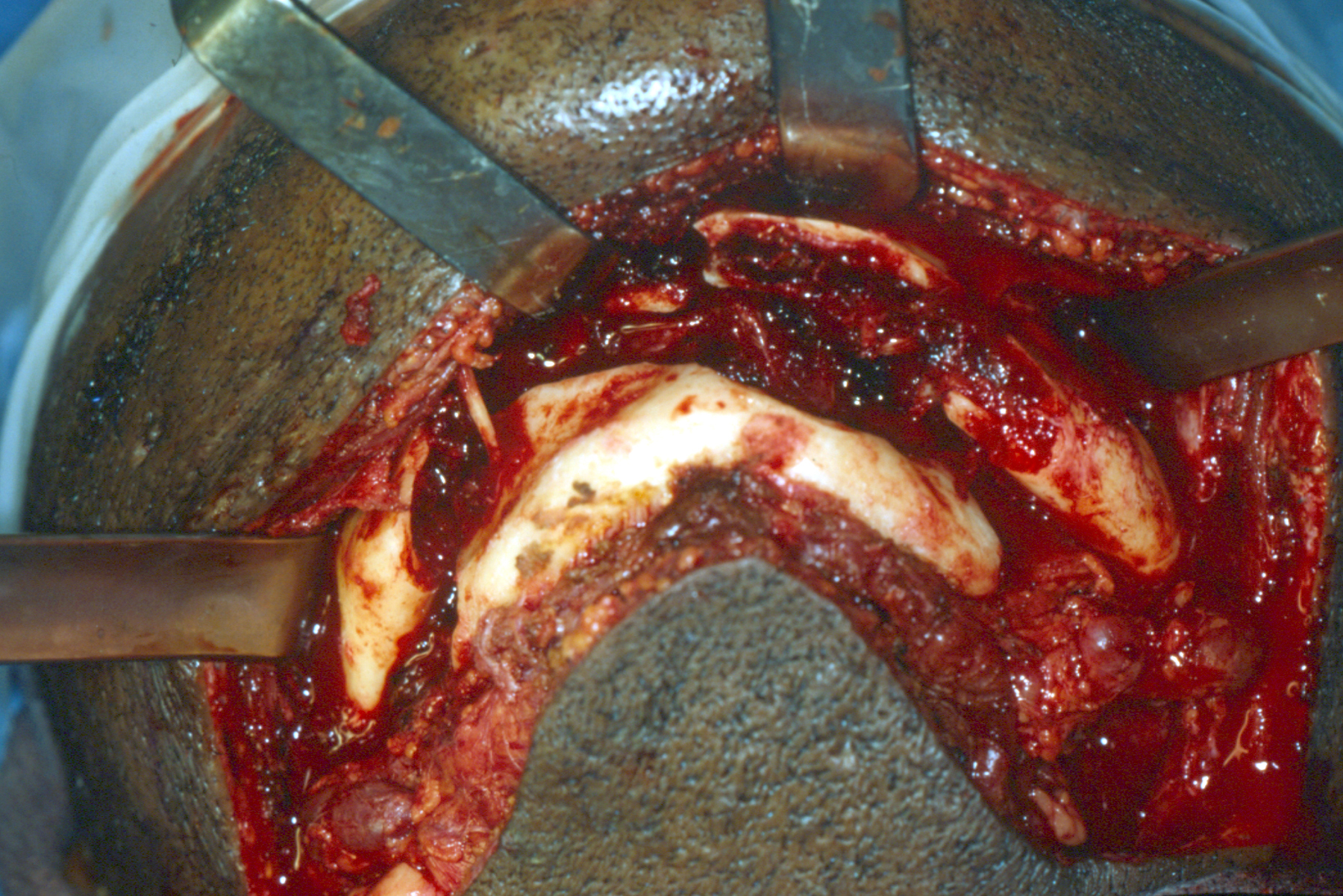
Comminuted mandibular fracture
The first description of mandibular fracture was as early as 1650 BC, when an Egyptian papyrus described the examination, diagnosis, and treatment of mandible fractures. Many patients received either improper treatment or no treatment and, subsequently, died. Hippocrates was the first to describe reapproximation and immobilization through the use of circumdental wires and external bandaging. The importance of establishing proper occlusion first was described in a textbook written in Salerno, Italy, in 1180. Maxillomandibular fixation was first mentioned in 1492, in an edition of the book Cirugia printed in Lyons. Chopart and Desault used dental prosthetic devices to immobilize fracture segments.
Most fracture treatment, however, involved some form of external bandage or wrap, occasionally used in conjunction with a bridle wire, until the 19th century, when Gilmer reformed the treatment of fractures by fixated full arch bars on the mandible and the maxilla. In 1888, Schede was the first to use a solid steel plate held by 4 screws for fixation.
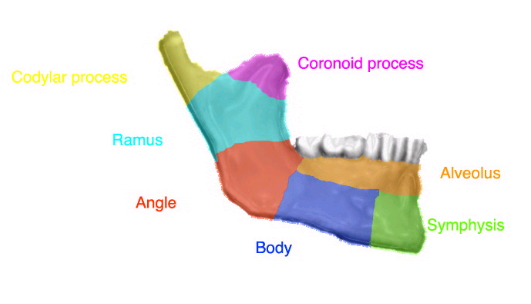
Classification of mandibular fractures based on their locations
The technique of rigid internal fixation was developed and popularized by Arbeitsgemeinschaft fur Osteosynthesefragen/Association for the Study of Internal Fixation (AO/ASIF) in Europe in the 1970s. The basic principles of the AO, outlined by Spiessl, call for primary bone healing under conditions of absolute stability. Rigid internal fixation must neutralize all forces (tension, compression, torsion, shearing) developed during functional loading of the mandible to allow for immediate function. This is accomplished by interfragmentary compression plates. Use an inferior border plate to counter compression forces and a superior border plate or arch bars to counter traction or tension forces at the superior border.
AO reconstruction plates also impacted the management of comminuted and infected mandibular fractures; Ellis reported a 7.5% infection rate in treatment of mandibular angle fractures with an AO reconstruction plate without intermaxillary fixation (IMF).
During the same time that Spiessl was expounding the AO doctrine, Champy et al in France were developing the concept of adaptive osteosynthesis. Champy advocated transoral placement of small, thin, malleable, stainless steel miniplates with monocortical screws along an ideal osteosynthesis line of the mandible. Champy believed that compression plates were unnecessary because of masticatory forces that produce a natural strain of compression along the inferior border.

Right parasymphysis fracture
These 2 changes of AO rigid internal fixation and the Champy method of monocortical miniplates revolutionized the treatment approach to mandibular fractures. Many fractures previously treated with closed reduction or open reduction with wire osteosynthesis are now commonly treated with open reduction with plate and screw fixation. An example of this evolution is the treatment of comminuted mandibular fractures. These were thought to be treated best by closed reduction to minimize stripping of the periosteum of small bone fragments. Although this treatment modality is still used, rigid fixatioow enables the clinician to avoid closed reduction with the use of reconstruction plates and good soft tissue coverage.
Classification of mandibular fractures
• Simple or closed – Fracture that does not produce a wound open to the external environment, whether it be through the skin, mucosa, or periodontal membrane
• Compound or open – Fracture in which an external wound, involving skin, mucosa, or periodontal membrane, communicates with the break in the bone
• Comminuted – Fracture in which the bone is splintered or crushed
• Greenstick – Fracture in which one cortex of the bone is broken and the other cortex is bent
• Pathologic – Fracture occurring from mild injury because of preexisting bone disease
• Multiple – Variety in which two or more lines of fracture on the same bone are not communicating with one another
• Impacted – Fracture in which one fragment is driven firmly into the other
• Atrophic – Fracture resulting from severe atrophy of the bone, as in edentulous mandibles
• Indirect – Fracture at a point distant from the site of injury
• Complicated or complex – Fracture in which considerable injury to the adjacent soft tissues or adjacent parts occurs; may be simple or compound
Classification by anatomic region

Right condylar fracture
• Symphysis – Fracture in the region of the central incisors that runs from the alveolar process through the inferior border of the mandible
• Parasymphyseal – Fractures occurring within the boundaries of vertical lines distal to the canine teeth
• Body – From the distal symphysis to a line coinciding with the alveolar border of the masseter muscle (usually including the third molar)
• Angle – Triangular region bounded by the anterior border of the masseter muscle to the posterosuperior attachment of the masseter muscle (usually distal to the third molar)
• Ramus – Bounded by the superior aspect of the angle to two lines forming an apex at the sigmoid notch
• Condylar process – Area of the condylar process superior to the ramus region
• Coronoid process – Includes the coronoid process of the mandible superior to the ramus region
• Alveolar process – Region that normally contains teeth
Posted in Oral Surgery Tagged angle, arch bars, body, compound fracture, fixation, greenstick fracture, mandibular fracture, multiple fracture, parasymphysis, simple fracture
Share this post, let the world know
Resection prostheses
Structures of forming devices
|
Classification of devices |
Forming |
Fixing |
substituting |
|
Indications for use |
For mouth and chin layer |
For lower jaw layer |
for resections of jaws |
|
Type of prosthesis |
Direct replacement |
Early replacement |
Delayedreplacement |
|
Structures |
Both jaws have teeth |
There are teeth on one jaw |
There are teeth on one side of a lower or an upper jaw. No teeth on both jaws |
|
Advantages |
improves hemostasis, form a prosthetic bed |
Protectfromfragmentsorfractions shifting, promote fasterrecovery of functions |
Less traumaticfor patient’s psyche |
|
Stages of making |
1.obtaining impressions 2. creating a fixing part 3.obtaining an impression by a fixing plate |
4. Making a resection part
5. Joining separate parts of the prosthesis |
6. Making an obturating part 7. Producing the prosthesis just after the operation |
Approximate card for self-processing of literature by students
|
List of questions |
Instructions to complete the task Short answers |
|
Types of prostheses for jaw resection.
|
The two types: direct and delayed Fordirescttypetheprosthesisismadebeforetheoperationandisapplied on the operating table, and the further prosthetics is done after the operation. |
|
Listthebasicindicationsformakingdirect prostheses |
For lower jaw resection (of thefrontal area, a half or complete removing) and upper jaw resection (one-sided or double-sided) |
|
Name the main stages of making direct prostheses |
Obtaining impressions, making the fixing part, Obtaining impressions, with the fixing part, making the resection part ,joining separate parts of the prosthesis,Submit the prosthesis on the operating table, making an obturative part of the prosthesis for the upper jaw(after the operation).
|
|
Give a comparative rating ofdirectprosthesesadvantages |
Directprosthesespreventfromfragmentsdisplacement, improve hemostasis, form a prosthetic bed. Duringsofttissueshealing, preventthemfromfallingin, promote fasterrecoveryof speech, are less traumaticfor patient’s psyche |
Tasks for obtained knowledge.testing
Classification of prosthetic devices after operations in maxillofacial area.
Structures of devices for chin resection with presence of teeth on both or one of the sides of the lower jaw.
Structuresofdevicesforresectionofhalfoflowerjawwith or without teeth on another side.
Formingandsubstitutingprosthesesforcomplete resection of the lower jaw depending on time of use.
Clinical and laboratory stages of making forming and substituting postresection prosthesis by Oksman.
Tasks for knowledge testing
Etiology of congenital and acquired defects of the palate.
Clinical features of congenital defects of the palate.
`Clinical features of acquired defects of the palate.
Orthopedic devices used in treatment of congenital defects ofthepalate..
Method of makingafloating obturator.
Orthopedic devices used in treatmentofacquired defects of the palate.
Method of making obturating prosthesesfor defects of the palate
|
Palate defects classification |
congenital |
acquired |
|
Etiology |
Takeplaceasaresultofnonunionofthesoftpalateandpalatine processesduring the process of face forming at early embryogenesis(7-8 weeks) the average is1% of100 newborn. |
1.asaresultofdeceases (osteomyelitis, syphilis) 2. asaresultofinjures (shotgun). 3. after surgical interventions (tumor) |
|
clinical picture |
Acrackinthemiddleofthepalateisobserved, mouth and nose are connected, that disturbs breathing and eating and further speaking |
There is ahole or a crack of various localisation. Ifitisimpossibletorestorethepalatebyasurgicalintervention, orthopedic methods are used |
|
Types of obturators |
Ambroise Paré andPier Foshar were the first to suggest obturators . In 1820Dellabarre suggested an obturators for the soft and the hard palate. This field was developed byKingsley(1864), Suersen(1966), Kaz, Varnenkroz, Shieldskyatal. Thedifferencebetweenthesuggestedobturatorsisinmethodsofjoiningfixingandobturatingparts. In the obturator by Suersen these parts are joined immovably. Normallydisjoininginmouthfromnosehappenswith a reduction of the upper pharyngeal constrictorcalled Passavant’s torus. Inobturator byKaztwopartsarejointwithaspring, in theobturatorby Varnerkrozit is done with a hinge, and Shieldsky joined them with a metal plate. In1902 Kazofferedaso-called“floating” obturatorthat consists only of an obturating part. Itsedgeshaveagroove-likeshapethatexactlycovertheedgesofthedefect. That’swhyitiskeptinmouth. Z.I.Chasovskaapplies obturatorby Kaz for infants |
|
|
Methods of making Obturator by Kaz |
Obtainanimpressionwithstens, whatisput on a S-shapedspatula.Stens soften in hot water is sticked to concavesurface of the narrow spatula and form it as a roller of an appropriate size. Therolleronthespatulaisenteredtothepatient’smouthandimpressionofthedefect is obtained.Stens remains are removed and the impression is plastered in the cuvette. Stens is changed to plastics. More ready obturator is adapted by rapidly polymerizing plastic |
|
ClassificationbyB.Y.Kurliandsky
(dependingon defectlocalization andpresence of teeth)
1. Defect of the hard palate with abutment teeth on both sides of the jaw.
2. Defect of thehard palate with abutment teeth on half of the jaw.
3. Defect of the hard palate and absence of teeth on the jaw.
4. Defect of thehard and soft palate.
Jaw fracture treatment
Injuries to the face, by their very nature, impart a high degree of emotional, as well as physical trauma to patients. The science and art of treating these injuries requires special training involving a “hands on” experience and an understanding of how the treatment provided will influence the patient’s long term function and appearance.
Oral and Maxillofacial Surgeons deliver emergency room coverage for facial injuries, which include the following conditions:
• Facial lacerations
• Intra-oral lacerations
• Avulsed (knocked out) teeth
• Fractured facial bones (cheek, nose or eye socket)
• Fractured jaws (upper and lower jaw)
Description
Maxillofacial trauma includes injuries to any of the bony or fleshy structures of the face. Any part of the face may be affected. Teeth may be knocked out or loosened. The eyes and their muscles, nerves, and blood vessels may be injured as well as the eye socket (orbit), which can be fractured by a forceful blow. The lower jaw (mandible) may be dislocated by force. Although anchored by strong muscles for chewing, the jaw is unstable in comparison with other bones and is easily dislocated from the temporomandibular joints that attach it to the skull. A fractured nose or jaw may affect the ability to breathe or eat. Any maxillofacial injury may also prevent the passage of air or be severe enough to cause a concussion or more serious brain damage.
Symptoms:
• Changes in sensation and feeling over the face
• Deformed or uneven face or facial bones
• Difficulty breathing through the nose due to swelling and bleeding
• Double vision
• Missing teeth
• Swelling around the eyes that may cause vision problems
• Bleeding from the nose, eyes, or mouth, or nasal blockage
• Breaks in the skin (lacerations)
Bruising around the eyes or widening of the distance between the eyes, which may mean injury to the bones between the eye sockets
The following may suggest bone fractures:
• Abnormal sensations on the cheek and irregularities that can be felt
• An upper jaw that moves when the head is still
The Nature of Maxillofacial Trauma
There are a number of possible causes of facial trauma such as motor vehicle accidents, accidental falls, sports injuries, interpersonal violence and work related injuries. Types of facial injuries can range from injuries of teeth to extremely severe injuries of the skin and bones of the face. Typically, facial injuries are classified as soft tissue injuries (skin and gums), bone injuries (fractures), or injuries to special regions (such as the eyes, facial nerves or the salivary glands).
Soft Tissue Injuries of the Maxillofacial Region
When soft tissue injuries such as lacerations occur on the face, they are repaired by suturing. In addition to the obvious concern of providing a repair that yields the best cosmetic result possible, care is taken to inspect for and treat injuries to structures such as facial nerves, salivary glands and salivary ducts (or outflow channels).
Bone Injuries of the Maxillofacial Region
Fractures of the bones of the face are treated in a manner similar to the fractures in other parts of the body. The specific form of treatment is determined by various factors, which include the location of the fracture, the severity of the fracture, the age and general health of the patient. When an arm or a leg is fractured, a cast is often applied to stabilize the bone to allow for proper healing. Since a cast cannot be placed on the face, other means have been developed to stabilize facial fractures.
One of these options involves wiring the jaws together for certain fractures of the upper and/or lower jaw. Certain other types of fractures of the jaw are best treated and stabilized by the surgical placement of small plates and screws at the involved site. This technique of treatment can often allow for healing and obviates the necessity of having the jaws wired together. This technique is called “rigid fixation” of a fracture. The relatively recent development and use of rigid fixation has profoundly improved the recovery period for many patients, allowing them to return to normal function more quickly.
The treatment of facial fractures should be accomplished in a thorough and predictable manner. More importantly, the patient’s facial appearance should be minimally affected. An attempt at accessing the facial bones through the fewest incisions necessary is always made. At the same time, the incisions that become necessary, are designed to be small and, whenever possible, are placed so that the resultant scar is hidden.
Fractures (or breaks in the bones) are common problems. Any individual really has the tendency of suffering from a fractured arm, finger, or any other parts of the body. There are also main types of fractures: open, closed, complete, and incomplete fracture. Even more, there are really some instances that we cannot avoid which would lead to fracture injury. Because of this, it is necessary to understand the causes, knowing fracture symptoms, and even identifying different ways on how to treat bone fracture. Information is readily accessible through the Web, there is no more reason for us to keep ignoring vital details that may be a lot of help for us later in life when it comes to complete or incomplete fracture of a bone. After all, no one else will greatly benefit from this information other than us and the people around us.
As for this article, we will be talking about jaw fracture or mandibular fracture. Like specific forms of fracture like Jones fracture and kneecap fracture, is specific to certain part of the body. As its name indicates, this form of fracture causes broken jaw. Fractured or dislocated jaw is second to nose dislocation when it comes to facial injuries since it is the nose that is usually fractured. Still, this condition is the 10th most common fracture in the human body. There is no need for us to dig into the details of the types of bone fracture especially this one. We will just go through with the basics for our benefit and easy understanding.
Definition and Overview of Jaw Fracture
A fractured jaw is more clinically known as mandibular fracture because it the mandible (jawbone in a layman’s term) that is broken or cracked. The mandible is the bone that is attached to the skull which allows opening of the mouth. When there is a broken mandible, there are certain problems that would be caused by this.
The demographics of the people who are most likely to suffer from jaw fracture are those male that are between the ages 20 and 29. Still, women have the tendency to have jaw injuries but the likelihood to have one is low. The ratio for jaw problems relating to fractured jaw between men and women is 4:1.
In most cases, the lower jaw is the common area where the jaw bone fracture occurs. However, there are already instances wherein the upper jaw also suffers from fracture or dislocation. Upper jaw fracture can still be similar with lower jaw fracture in many cases and causes. The need for a coastal jaw surgery is required in this kind of jaw fracture.
Causes of Jaw Fracture
Like any forms of fracture, fracture jaw is caused by sudden impact that is brought to the mandible or jawbone. The most common fracture diagnosis that results to jaw dislocation and fracture are vehicular accidents, assaults, injuries from sports, and even fall with great impact. These are the reasons why it is men that are usually the victims of jaw fractures. Still, there can be other causes of mandibular fracture which are all caused by a great impact. Jaw fracture from tooth extraction can also be another cause of this form of fracture though not commonly occurring.
When an individual suffers from one or two of these, there is a need to check out for some symptoms (which will be discussed below) so that proper procedure on how to heal this kind of injury can be done immediately.
Symptoms and Diagnosis
The most common among the broken jaw symptoms is the jaw pain. Just like any other forms of fracture, jaw injury results to pain as well. In addition to this, there is also a misalignment of the teeth. As an individual start feeling that his/her teeth are not anymore in a normal alignment is another possibility of fractured jaw bone. This can be observed by anyone since it will really feel awkward. Other fractured jaw symptoms are bleeding inside the teeth, difficulty in talking and breathing, and swelling of the fractured part.
Still, there are more symptoms of broken jaw bones that we should be careful about. Immediately as an individual encounters the abovementioned causes, the need to check out for sudden changes in the jawbone or its functions is a must. When there is any, seeing the doctor is the first course of action that one needs to do. This way, fracture complications can be avoided. Most importantly, it is the doctor that best knows the procedures that should be done.
Care and Treatment
In immediate instances wherein an individual faces a forceful impact on his/her jawbone, the need for a first aid treatment is a necessity. This first aid treatment would include cold compress to avoid swelling and taking of some prescribed drugs to reduce pain. These are just of the basic things that we need to do to treat jaw fracture. When there are already observed abnormality (as already discussed earlier), it is recommended to consider an X-ray test so that a proper jaw reconstruction surgery can also be planned out afterwards and if needed. Of course, this latter course of action would need the assistance and opinion of a doctor especially the one who specializes on jaw injury.
More importantly, a specialized jaw fracture treatment would be needed to ensure full recovery and quick return to normal state. This is to avoid further complication that may just make it hard to correct the problem. In addition, there are also certain medicines that need to be taken when there are already swelling and pain especially when jaw fracture symptoms are already surfacing.
Though our body is capable of its own jaw reconstruction, there is still a need to use advanced means to correct the problem. The basic and most common fractured jaw treatment is fracture surgery. This is a corrective jaw surgery that aims to normalize the jawbone and bring it back to its natural function which includes the standard state of the teeth, breathing, and speech. The jaw surgery is the best way to secure that an individual does not have to suffer from further problems caused by the fractured bone. In addition, when an individual is suffering from an upper jaw fracture another form of jaw fracture surgery would be needed. They call an upper jaw surgery as the maxillofacial jaw surgery which only focuses on the upper jaw that has been broken or dislocated due to similar causes stated earlier. Jaw surgery recovery may actually take some time but it would really be worth the wait. During the process of rehabilitation, it is also at this point that fractured jaw recovery can be achieved. The fracture healing time would vary on the capability and metabolism of the individual. Being impatient and not waiting for the jaw fracture recovery time to be complete will do you no good. Instead, it is best to wait until all jaw injuries are healed before resuming your usual activities.
When the jaw fracture surgery is done, there would be a need for special fracture jaw diet. This is due to the fact that there is still a need to immobilize the fractured area to avoid fracture complications and more jaw pain. In addition, this would help in the recovery time of the individual to become quick. Though the body is naturally curing itself from conditions such as fracture, there is still the need to wear brace/braces to align the bone fracture. A fracture cast is only one of the necessary things that an individual should have to have a full recovery from the condition.
Still, there are yet to learn about this form of fracture. Just like any classification of fracture, it is necessary that we learn the basics so that we would also know the bone fracture treatment that we have to go through. Most importantly in the case of jaw fracture, we need to know and prepare ourselves with the broken jaw surgery that we might have to undergo is faced in a certain condition.
Mandibular fracture, also known as fractures of the jaw, are breaks through the mandibular bone. They usually occur due to trauma and are often associated with other facial trauma. The types of mandibular fractures include fractures at the symphyseal area, horizontal ramus, mandibular angle and condylar neck.
Classification
There are various classification systems of mandibular fractures in use.
Location

Photo of the mandible demonstrating the frequency of mandibular fractures by location.
This is the most useful classification, because both the signs and symptoms, and also the treatment are dependent upon the location of the fracture. The mandible is usually divided into the following zones for the purpose of describing the location of a fracture (see diagram): condylar, coronoid process, ramus, angle of mandible, body (molar and premolar areas), parasymphysis and symphysis.
Alveolar
This type of fracture involves the alveolus, also termed the alveolar process of the mandible.
Condylar
Condylar fractures are classified by location compared to the capsule of ligaments that hold the temporomandibular joint (intracapsular or extracapsular), dislocation (whether or not the condylar head has come out of the socket (glenoid fossa) as the muscles (lateral pterygoid) tend to pull the condyle anterior and medial) and neck of the condyle fractures. E.g. extracapsular, non-displaced, neck fracture. Pediatric condylar fractures have special protocols for management.
Coronoid
Because the coronoid process of the mandible lies deep to many structures, including the zygomatic complex (ZMC), it’s rare to be broken in isolation. It usually occurs with other mandibular fractures or with fracture of the zygomatic complex or arch. Isolated fractures of the coronoid process should be viewed with suspicion and fracture of the ZMC should be ruled out.
Ramus
Ramus fractures are said to involve a region inferiorly bounded by an oblique line extending from the lower third molar (wisdom tooth) region to the posteroinferior attachment of the masseter muscle, and which could not be better classified as either condylar or coronoid fractures.
Angle
The angle of the mandible refers to the angle created by the arrangement of the body of the mandible and the ramus. Angle fractures are defined as those that involve a triangular region bounded by the anterior border of masseter muscle and an oblique line extending from the lower third molar (wisdom tooth) region to the posteroinferior attachment of the masseter muscle.
Body
Fractures of the mandibular body are defined as those that involve a region bounded anteriorly by the parasymphysis (defined as a vertical line just distal to the canine tooth) and posteriorly by the anterior border of the masseter muscle.
Parasymphysis
Parasymphyseal fractures are defined as mandibular fractures that involve a region bounded bilaterally by vertical lines just distal to the canine tooth.
Symphysis
Symphyseal fractures are a linear fractures that run in the midline of the mandible (the symphysis).
Fracture type
Mandibular fractures are also classified according to categories that describe the condition of the bone fragments at the fracture site and also the presence of communication with the external environment.
Greenstick
Greenstick fractures are incomplete fractures of flexible bone, and for this reason typically occur only in children. This type of fracture generally has limited mobility.
Simple
A simple fracture describes a complete transection of the bone with minimal fragmentation at the fracture site.
Comminuted
The opposite of a simple fracture is a comminuted fracture, where the bone has been shattered into fragments, or there are secondary fractures along the main fracture lines. High velocity injuries (e.g. those caused by bullets, improvised explosive devices, etc…) will frequently cause comminuted fractures.
Compound
A compound fracture is one that communicates with the external environment. In the case of mandibular fractures, communication may occur through the skin of the face or with the oral cavity. Mandibular fractures that involve the tooth-bearing portion of the jaw are by definition compound fractures,[4] because there is at least a communication via the periodontal ligament with the oral cavity and with more displaced fractures there may be frank tearing of the gingival and alveolar mucosa.
Involvement of dentition
When a fracture occurs in the tooth bearing portion of the mandible, whether or not it’s dentate or edentulous will affect treatment. Wiring of the teeth helps stabilize the fracture (either during placement of osteosynthesis or as a treatment by itself), so the lack of teeth will guide treatment. When an edentulous mandible (no teeth) is less than 1 cm in height (as measured on panoramic radiograph or CT scan) addition risks apply because the blood flow from the marrow (endosseous) is minimal and the healing bone must rely on blood supply from the periosteum surrounding the bone. If a fracture occurs in a child with mixed dentition different treatment protocols are needed.
Other fractures of the body, are classified as open or closed. Because fractures that involve the teeth, by definition, communicate with the mouth this distinction is largely lost in mandible fractures. Condylar, ramus, coronoid process and ramus fractures are generally closed whereas angle, body and parasymphsis fractures are generally open.

multiple mandible fractures of a patient in the right condyle (extracapsular/neck/not dislocated), right body (vertically unfavourable) and left coronoid process
Displacement
The degree to which the segments are separated. The larger the separation, the more difficult it is to bring them back together (approximate the segments)
Favorablity
For angle and posterior body fractures, when the angle of the fracture line is angled back (more posterior at the top of the jaw and more anterior at the bottom of the jaw) the muscles tend to bring the fracture segments together. This is called favorable. When the angle of the fractures is pointing to the front, it’s unfavorable.
Age of the fracture
While mandible fractures have similar complication rates whether treated immediately or days later, older fractures are believed to have higher non-union and infection rates although the data on this makes it difficult to draw firm conclusions.
Signs and symptoms
General
By far, the two most common symptoms described are pain and the feeling that teeth no longer correctly meet (traumatic malocclusion, or disocclusion). The teeth are very sensitive to pressure (proprioception), so even a small change in the location of the teeth will generate this sensation. Patients will also been very sensitive to touching the area of the jaw that is broken, or in the case of condylar fracture the area just in front of the tragus of the ear.
Other symptoms may include loose teeth (teeth on either side of the fracture will feel loose because the fracture is mobile), numbness (because the inferior alveolar nerve runs along the jaw and can be compressed by a fracture) and trismus (difficulty opening the mouth).
Outside the mouth, signs of swelling, bruising and deformity can all be seen. Condylar fractures are deep, so it’s rare to see significant swelling although, the trauma can cause fracture of the bone on the anterior aspect of the external auditory meatus so bruising or bleeding can sometimes be seen in the ear canal. Mouth opening can be diminished (less than 3 cm). There can be numbness or altered sensation (anesthesia/paraesthesia in the chin and lower lip (the distribution of the mental nerve).
Intraorally, if the fracture occurs in the tooth bearing area, a step may seen between the teeth on either side of the fracture or a space can be seen (often mistaken for a lost tooth) and bleeding from the gingiva in the area. There can be an open bite where the lower teeth, no longer meet the upper teeth. In the case of a unilateral condylar fracture the back teeth on the side of the fracture will meet and the open bite will get progressively greater towards the other side of the mouth.
Sometimes bruising will develop in the floor of the mouth (sublingual eccymosis) and the fracture can be moved by moving either side of the fracture segment up and down. For fractures that occur in the non-tooth bearing area (condyle, ramus, and sometimes the angle) an open bite is an important clinical feature since little else, other than swelling, may be apparent.
Condylar
This type of fractured mandible can involve one condyle (unilateral) or both (bilateral). Unilateral condylar fracture may cause restricted and painful jaw movement. There may be swelling over the temporomandibular joint region and bleeding from the ear because of lacerations to the external auditory meatus. The hematoma may spread downwards and backwards behind the ear, which may be confused with Battle’s sign (a sign of a base of skull fracture), although this is an uncommon finding so if present, intra-cranial injury must be ruled out. If the bones fracture and overlie each other there may be shortening of the height of the ramus. This results in gagging of the teeth on the fractured side (the teeth meet too soon on the fractured side, and not on the non fractured side, i.e. “open bite” that becomes progressively worse to the unaffected side). When the mouth is opened, there may be deviation of the mandible towards the fractured side. Bilateral condylar fractures may cause the above signs and symptoms, but on both sides. Malocclusion and restricted jaw movement are usually more severe. Displacement of the condyle through the roof of glenoid fossa and into the middle cranial fossa is rare.
Epidemiology
Mandible fracture causes vary by the time period and the region studied. In North America, blunt force trauma (a punch) is the leading cause of mandible fracture where as in India, motor vehicle collisons are now a leading cause. On battle grounds, it’s more likely to be high velocity injuries (bullets and shrapnel). Prior to the routine use of seat belts, airbags and modern safety measures, motor vehicle collisions where a leading cause of facial trauma. The relationship to blunt force trauma explains why 80% of all mandible fractures occur in males. Mandibular fracture is a rare complication of third molar removal, and may occur during the procedure or afterwards. With respect to trauma patients, roughly 10% have some sort of facial fracture, the majority of which come from motor vehicle collisions. When the person is unrestained in a car, the risk of fracture rises 50% and when an unhelmeted motorcyclist the risk rises 4-fold.
Diagnosis
Imaging
Plain film radiography
Traditionally, plain films of the mandible would be exposed but had lower sensitivity and specificity owing to overlap of structures. Views included AP (for parasymphsis), lateral oblique (body, ramus, angle, coronoid process) and Towne’s (condyle) views. Condylar fractures can be especially difficult to identify, depending on the direction of condylar displacement or dislocation so multiple views of it are usually examined with two views at perpendicular angles.
Panoramic radiography
Panoramic radiographs are tomograms where the mandible is in the focal trough and show a flat image of the mandible. Because the curve of the mandible appears in a 2-dimensional image, fractures are easier to spot leading to an accuracy similiar to CT except in the condyle region. In addition, broken, missing or malaligned teeth can often be appreciated on a panormic image which is frequently lost in plain films. Medial/lateral displacement of the fracture segements and especially the condyle are difficult to gauge so the view is sometimes augmented with plain film radiography or computed tomography for more complex mandible fractures.
Computed tomography
Computed tomography is the most sensitive and specific of the imaging techniques. The facial bones can be visualized as slices through the skeletal in either the axial, coronal or sagittal planes. Images can be reconstructed into a 3-dimensional view, to give a better sense of the displacement of various fragments. 3D reconstruction, however, can mask smaller fractures owing to volume averaging, scatter artifact and surrounding structures simply blocking the view of underlying areas.
Research has shown that panoramic radiography is similiar to computed tomography in it’s diagnostic accuracy for mandible fractures and both are more accurate than plain film radiograph. The indications to use CT for mandible fracture vary by region, but it does not seem to add to diagnosis or treatment planning except for comminuted or avulsive type fractures, although, there is better clinician agreement on the location and absence of fractures with CT compared to panoramic radiography.

Panoramic radiograph of a simple mandible fracture of the right mandibular body, minimally displaced. Note that the teeth to the left of the fracture do not touch

lateral oblique image demonstrating a fractured mandible.

Towne’s view of a bilateral condyle fracture. White arrow is a fracture on the neck of the condyle. Black arrow shows the condyle pulled to the medial. The same injury can be seen on the opposite side

3D CT reconstruction of mandible fracture, white arrow marks fracture, red arrow marks moderate displacement and open bite

occlusal radiograph of a mandibular parasymphasis fracture
Treatment
Like all fractures, consideration has to be given to other illnesses that might jeopardize the patient, then to reduction and fixation of the fracture itself. Except in avulsive type injuries, or those where there might be airway compromise, a several day delay in the treatment of mandible fractures seems to have little impact on the outcome or complication rates.
General Considerations
Since mandible fractures are usually the result of blunt force trauma to the head and face, other injuries need to be considered before the mandible fracture. First and foremost is compromise of the airway. While rare, bilateral mandible fractures that are unstable can cause the tongue to fall back and block the airway. Fractures such as a symphyseal or bilateral parasymphyseal may lead to mobility of the central portion of the mandible where genioglossus attaches, and allow the tongue to fall backwards and block the airway.In larger fractures, or those from high velocity injuries, soft tissue swelling can block the airway.
In addition to the potential for airway compromise, the force delievered to break the jaw can be great enough to either fracture the cervical spine or cause intra-cranial injury (head injury). It is common for both to be assessed with facial fractures.
Finally, vascular injury can result (with particular attention to the internal carotid and jugular) from high velocity injuries or severely displaced mandible fractures.
Loss of consciousness combined with aspiration of tooth fragments, blood and possibly dentures mean that the airway may be threatened.
Reduction
Reduction refers to approximating the ends of the bones edges that are broken. This is done with either an open technique, where an incision is made, the fracture is found and is physically manipulated into place, or closed technique where no incision.
The mouth is unique, in the that teeth are well secured to the bone ends but come through epithelium (mucosa). A leg or wrist, for instance, has no such structure to help with a closed reduction. In addition, when the fracture happens to be in a tooth bearing area of the jaws, aligning the teeth well usually results in alignment of the fracture segments.
To align the teeth, circumdental wiring is often used where wire strands are wrapped around each tooth then attached to a stainless steel arch bar. When the maxillary (top) and mandibular (bottom) teeth are aligned together, this brings the fracture segments into place. Higher tech solutions are also available, to help reduce the segments with arch bars using bonding technology.
Fixation
Simple fractures are usually treated with closed reduction and and indirect skeletal fixation, more commonly referred to as maxillo-mandibular fixation (MMF). The closed reduction is explained above. The indirect skeletal fixation is accomplished by placing an arch bar, secured to the teeth on the maxillary and mandibular dentition, then securing the top and bottom arch bars with wire loops.
Many alternatives exist to secure the maxillary and mandibular dentition including resin bonded arch bars, Ivy loops (small eyelets of wires), orthodontic bands and MMF bone screws where titanium screws with holes in the head of them are screwed into the basal bone of the jaws then secured with wire.
Closed reduction with direct skeletal fixation follows the same premise as MMF except that wires are passed through the skin and around the bottom jaw in the mandibule and through the piriform rim or zygomatic buttresses of the maxilla then joined together to secure the jaws. The option is sometimes used when a patient is edentulous (has no teeth) and rigid interal fixation cannot be used.
Open reduction with direct skeletal fixation allows the bones to be directly mandipulated through an incision so that the fractured ends meet, then they can be secured together either rigidly (with screws or plates and screws) or non-rigidly (with transosseous wires). There are a multitude of various plate and screw combinations including compression plates, non-compression plates, lag-screws, mini-plates and biodegradable plates.
External fixation, which can be used with either open or closed reduction uses a pin system, where long screws are passed through the skin and into either side of a fracture segment (typically 2 pins per side) then secured in place using an external fixator. This is a more common approach when the bone is heavily comminuted (shattered into small pieces, for instance in a bullet wound) and when the bone is infected (osteomyelitis).
Regardless of the method of fixation, the bone need to remain relatively stable for a period of 3–6 weeks. On average, the bone gains 80% of it’s strength by 3 weeks and 90% of it by 4 weeks. There is great variation depending on the severity of injury and health of the wound and patient.

Maxillomandibular fixation with circumdental wires, archbars and elastics for a condyle fracture

Rigid internal fixation of parasymphasis fracture of the mandible. White arrow marks fracture, black arrow marks arch bar on lower teeth

Rigid internal fixation of right condyle fracture with mini-plate on the neck of the condyle. Black arrow marks right earlobe, white arrow marks head of the condyle

External fixation of left mandible fracture
Special Considerations
Condyle
The best treatment for condylar fractures is controversial. There are two main options, namely closed reduction or open reduction and fixation. Closed reduction may involve intermaxillary fixation, where the jaws are splinted together in the correct position for a period of weeks. Open reduction involves surgical exposure of the fracture site, which can be carried out via incisions within the mouth or incisions outside the mouth over the area of the condyle. Open reduction is sometimes combined with use of an endoscope to aid visualization of fracture site. Although closed reduction carries a risk of the bone healing out of position, with consequent alteration of the bite or the creation of facial asymmetry, it does not risk temporary damage to the facial nerve or result in any facial scar that accompanies open reduction. A systematic review was unable to find sufficient evidence of the superiority of one method over another in the management of condylar fractures. Paediatric condylar fractures are especially problematic, owing to the remaining growth potential and possability of ankylosis of the joint.
Edentulous mandible
A broken jaw that has no teeth in it faces two additional issues. First, the lack of teeth makes reduction and fixation using MMF difficult. Instead of placing circumdental wires around the teeth, existing dentures can be left in (or Gunning splints, a type of temporary denture) and the mandible fixated to the maxilla using skeletal fixation (circummandibular and circumzygomatic wires) or using MMF bone screws. More commonly, open reduction and rigid internal fixation is placed.
When the width of the mandible is less than 1cm, the jaw looses its endosteal blood supply. Instead, the blood supply comes largely from the periosteum. Open reduction (which normally strips the periosteum during the dissection) can lead to avascular necrosis. In these cases, oral surgeons sometimes opt for external fixation, closed reduction, supraperiosteal dissection or other techniques to maintain the periosteal blood flow.
High Velocity Injuries
In high velocity injuries, the soft tissue can be severely damaged far from the bullet wound itself due to hydrostatic shock. Because of this the airway must be carefully managed and vessels well examined. Because the jaw can be highly comminuted, MMF and rigid internal fixation can be difficult. Instead, external fixation is often used.
Pathologic fracture
Fractures where large cysts or tumours are in the area (and weaken the jaw), where there is an area of osteomyelitis or where osteonecrosis exist cause special challenges to fixation and healing. Cysts and tumours can limit effective bone to bone contact and osteomyelitis or osteonecrosis compromise blood supply to the bone. In all of the situations, healing will be delayed and sometimes, resection is the only alternative to treatment.
Prognosis
The healing time for a routine mandible fractures is 4-6 weeks whether MMF or rigid internal fixation (RIF) is used. For comparable fractures, patients who received MMF will loose more weight and take longer to regain mouth opening, whereas, those who receive RIF have higher infection rates.
The most common long-term complications are loss of sensation in the mandibular nerve, malocclusion and loss of teeth in the line of fracture. The more complicated the fracture (infection, comminution, displacement) the higher the risk of fracture.
Condylar fractures have higher rates of malocclusion which in turn are dependent on the degree of displacement and/or dislocation. When the fracture is intracapsular there is a higher rate of late-term osteoarthritis and the potential for ankylosis although the later is a rare complication as long as mobilization is early. Pediatric condylar fractures have higher rates of ankylosis and the potential for growth disturbance.
History
Management of mandible fractures has been mentioned as early as 1700 B.C. in the Edwin Smith Papyrus and later by Hippocrates in 460 B.C., “Displaced but incomplete fractures of the mandible where continuity of the bone is preserved should be reduced by pressing the lingual surface with the fingers…”. Open reduction was described as early as 1869.[32] Since the late 19th century, modern techniques including MMF (see below) have been described with titanium based rigid internal fixation becoming commonplace since the 1970’s and biodegradable plates and screws being available since the 1980’s.
Treatment depends on the type of fracture, its severity, the individual’s age and general health. The first priority in treating any fracture is to address the entire medical status of the patient. Medical personnel are trained not allow a painful, deformed limb to distract them from potentially life-threatening injury elsewhere or shock. If an open fracture is accompanied by serious soft tissue injury, it may be necessary to control bleeding and the shock that can accompany loss of blood.
First aid is the appropriate initial treatment in emergency situations. It includes proper splinting, control of blood loss, and monitoring vital signs such as breathing and circulation.
|
Fractures of the lower jaw (mandible) are suspected in patients with post-traumatic malocclusion or focal swelling and tenderness over a segment of the mandible. Other clues include defects (stepoff) of the dental occlusal surface, alveolar ridge disruptions, and anesthesia in the distribution of the inferior alveolar or mental nerve. Some fractures result in palpable instability. Fractures of the mandibular condyle usually cause preauricular pain, swelling, and limited opening of the mouth (trismus). With a unilateral condylar fracture, the jaw deviates to the affected side when the mouth is opened.
Fractures of the midface, which includes the area from the superior orbital rim to the maxillary teeth, can cause irregularity in the smooth contour of the cheeks, malar eminences, zygomatic arch, or orbital rims. Infraorbital nerve anesthesia, enophthalmos, or diplopia suggests an orbital floor fracture. An injury near the orbit requires an eye examination, including, at least, assessment of visual acuity, pupils, and extraocular movements. Trismus and a defect on palpation of the zygomatic arch suggest zygomatic arch fracture. The Le Fort classification Facial Trauma: Le Fort classification of midface fractures. can be used to describe midface fractures. Traumatic malocclusion and upper alveolar ridge fractures may suggest a maxillary fracture that involves the occlusal surface. Brain injury and fractured cervical vertebrae are possible when trauma has been severe enough to fracture facial bones. In major impact injuries, hemorrhage and edema due to a facial fracture may compromise the airway.
|
|
||||||||
|
|
|
|
||||||
|
||||||||
A panoramic dental x-ray is preferred for an isolated mandibular fracture. Fine-cut CT (1-mm slices) is done in axial and coronal planes to diagnose facial fractures.
An oral endotracheal airway may be required to maintain airway patency in patients with hemorrhage, edema, or significant tissue disruption. Definitive facial fracture management is complex and may include internal fixation.
Tooth socket fractures: Fractures through a tooth socket are open fractures. They require antibiotic prophylaxis (typically with a broad-spectrum antibiotic that is particularly effective against anaerobes, such as penicillin) given orally as a liquid or parenterally.
Mandible fractures: For a fractured mandible, treatment ranges from soft diet alone to maxillomandibular fixation (wiring the jaw shut), rigid open fixation, or both. If fixation is available within the first few hours after injury, closure of any lip or oral lacerations should be delayed until the fracture has been reduced. For maxillomandibular fixation, metal bars (arch bars) are attached to the buccal surface of the upper and lower teeth and then wired to each other after correct occlusion has been established. Patients with maxillomandibular fixation should always carry wire cutters in case of vomiting. Fixation may need to last several weeks. Eating is restricted to liquids, pureed foods, and supplements. Because only part of the teeth surfaces can be brushed, control of plaque formation, infection, and halitosis is accomplished using a 60-sec rinse with 30 mL of chlorhexidine 0.12% every morning and evening. Jaw-opening exercises usually help restore function after fixation is discontinued.
Condylar fractures may require only 2 to 3 wk of maxillomandibular fixation, followed by a soft diet. However, severely displaced, bilaterally fractured condyles may require open reduction and fixation. Condylar fractures in children should not be rigidly immobilized because ankylosis and abnormal facial development may result. Flexible (elastic) fixation for 5 to 10 days is usually sufficient.
Midface fractures: Fractures of the midface are treated surgically if they cause malocclusion, enophthalmos, diplopia, infraorbital nerve anesthesia, or unacceptable cosmetic deformity. Surgical treatment usually consists of internal stabilization using fine screws and plates. Surgery can often be delayed until swelling subsides, particularly if the indication for surgery is not clear.

PRINCIPLES OF MANAGEMENT OF FRACTURES:
- Reduction of the fracture-Reduction can be done in 2 days: Open Reduction or Closed Reduction, as will be discussed below
- Fixation & stabilization of the fracture-Direct or Indirect
- Immobilization of segments at fracture site
- Occlusion restored-to allow the patient to bite in his original position
- Infection eradicated/prevented-infection can prevent or delay healing, thus it is of essence that infection be avoided.
TREATMENT OPTIONS FOR MANDIBULAR FRACTURE
- No treatment (conservative management)
- Closed reduction
- Open reduction internal fixation (ORIF)
Reduction of Fracture
Can be closed or open reduction

intermaxillary fixation (IMF) with upper and lower archbars and tie wires
Closed reduction
-In closed reduction, there is no direct opening/exposure/ manipulation/visualization of the fracture area
–Occlusion is used as a guide, in the sense that the teeth are brought into occlusion and tied together (i.e. intermaxillary fixation, or IMF) by means of archbars & tie wires or elastics, or tie wires alone (eg: eyelets) No attempt is made to directly approximate the fracture site, hence it is also an indirect way of fixing the fracture segments together ( ie indirect fixation)
It is thus important to recognize any pre-existing occlusal abnormalities such as a gap between the upper and lower front teeth when the patient bites in his usual occlusion (anterior open bite) or a class III occlusion (whereby the lower dentition is relatively more protruded compared to the upper dentition.

Open reduction internal fixation (ORIF)-fixation via extraoral approach
Open reduction
Open reduction is a surgical procedure done by direct visualization of the fracture area, and the fracture segments are re-approximated manually and fixed with the help of titanium screws & plates. If open reduction is done, the teeth do not need to be tied together for as long a time as in closed reduction.
-The surgical approach can be from inside of the mouth (intra-oral) or externally through the facial skin (extra-oral), depending on the site of fracture and accessibility. Eg, fracture of the parasymphysis and symphysis are often approached intra-orally, while fracture at the angle or ramus of the mandible are approached extra-orally.
The common approach in management of a mandibular fracture is through open reduction and internal fixation (ORIF).
ADVANTAGES AND DISADVANTAGES
Advantages of open reduction (or disadvantages of closed reduction)
- Bone fragments re-approximated exactly by direct visualization. This promotes primary bone healing, and thus, absolute stability.
- Decreased period of time that the upper and lower teeth are tied together (immobilization). Therefore, this allows early return to normal function of the mouth (i.e. better speech, diet, oral hygiene)
- Open reduction is the option of choice in patients with medical conditions such as seizures, neurological/psychological disorders, gastrointestinal tract disorders (esp gastritis).
Disadvantages of open reduction (or advantages of closed reduction)
- More expensive(the plates & screws are made of titanium)
- Foreign body left in body (plates and screws are ofteot removed from the body. If they are to be removed, a second surgery is required)
- Need operation room and equipment in most cases
- May leave unsightly scars if the fixation is done from the extra-oral approach.
- There is some risk to the neurovascular structures and teeth/tooth buds, as drills and screws penetrate the jaw bone.
- Require specialized skills for placing plates & screws.
Fixation & Stabilization
-Direct vs Indirect: Direct fixation is done using screws and plates placed against the fracture site to directly prevent it from movement. Indirect fixation is done by intermaxillary fixation (IMF). When the occlusion is tied together in its original bite, the fracture segments are automatically approximated together without any direct fixing of the fracture site.
Direct fixation can be: Intraoral vs Extraoral: Intraoral fixation devices include plates and screws, while extraoral fixation can be seen as metal bars protruding out of the skin after the operation.
Immobilization
The period of immobilization depends on type of fracture & bone involved:
Eg:-mandible fracture(closed reduction): 4-6 weeks
-Mandible fracture (open reduction): 2 weeks is sufficient
-condyle fracture: 2-3 weeks (condyles should not be fixed for too long a period of time for fear of TMJ problems in the long run due to bony fusion of the condyle process (known as “ankylosis”).
Factors affecting choice of treatment
1. Patient factors (eg cost, duration of intermaxillary fixation, medical condition, occupation that makes a long period of immobilizationg very inconvenient etc.)
2. Type of fracture (Some fractures do not require active treatment, such as condylar fracture)
3. Skill of surgeon
4. Availability of hardware and equipments
Complications of fracture
- Delayed union: often due to infection
- Malunion/malocclusion: fracture segments join together in an abnormal position.
- Non-union: often due to infection
- Infection
- Nerve parasthesia/numbness (eg. inferior alveolar nerve)
Fractures of the condylar process and head
Classification
General considerations
Controversy has surrounded all aspects of fractures of the condylar process. There have been several proposed classification methods of these types of fractures.
Following, the AO classification is presented along with a simplified version. The AO classification allows for better communication between radiologists and surgeons. On the other hand, the simplified version better reflects the clinical treatment implications.
AO Classification
The condylar process and head is a subunit of the mandible and is defined by an oblique line running backward from the sigmoid notch to the upper masseteric tuberosity. The condylar process is differed into three subregions:
- Head
- Neck
- Subcondylar (caudal) area
Frontal view.
Three lines are used to define these subregions:
1. The first line parallels the posterior border of the mandible
2. The sigmoid notch line runs perpendicular to the first line at the deepest portion of the sigmoid notch
3. A line below the lateral pole of the condylar head that is also perpendicular to the first line.
Clinical pearl: the neck region can be divided into high and low halves by equally dividing the distance between the sigmoid notch line and the lateral pole line.
Treatment implications – simplified classification. In contrast to the descriptive, previously defined anatomical classification, a more simplified one is outlined and used in the Surgery Reference.
The surgeon decides to treat condylar process fractures in an open or closed method. To perform an open reduction and internal fixation, there must be room in the superior fragment for at least two screws fixing the same plate.
Clinically, this equates to open treatment of condylar neck fractures or subcondylar (caudal) fractures (A). The surgeon may elect to place one or two plates depending on the location and configuration of the fracture.
Fractures at a level where there is inadequate space for two holes to be drilled for the plate (B) require special techniques of osteosynthesis. For that reason, among others, most surgeons choose closed treatment for these joint fractures.
General considerations
Fractures of the condylar process (unilateral or bilateral) can occur in isolation. They are more often combined with other mandibular fractures.
Imaging
Routine diagnosis of this type of fracture should include radiographs taken in two planes at 90° to each other; the minimum requirement is a PA view and a panoramic view.
CT or digital volume tomography (DVT) imaging may be used as an alternative.
Panoramic view showing left condylar process fracture in association with an anterior body fracture.
Towne’s (oblique PA) view of the above patient. X-ray taken at 90° to show displacement of left condylar process fracture. Vertical shortening of the left mandible is noted along with the right anterior body fracture.
CT scans give the surgeon the best information with regard to fracture location, morphology, fragmentation, and associated injuries.
CT scan 3-D reconstruction illustrates right condylar process fracture.
Coronal view of the above patient shows angulation and luxation of the condylar process fracture.
Clinical findings
The dental occlusion can give orientation about the fracture location. With a unilateral condylar process fracture and subsequent reduction of height in the ramus region, the clinician will see an ipsilateral premature occlusion and contralateral open bite. The dental midline will shift toward the side of fracture.
The occlusion shows premature contact on the right with the deviation of the jaw to the affected side that is commonly seen with a right mandibular condyle fracture.
Bilateral fractures with shortening and dislocation result in anterior open bite with minimal deviation of the midline.
Pitfall: widening of the lower face
Bilateral condyle fractures associated with fractures of the symphysis and body region often produce a widening of the mandible and subsequent malocclusion. These fractures are very difficult to treat. Great care must be taken when performing the open reduction and internal fixation of the body fractures to assure the mandible is narrowed to its pre-injury status. Failure to recognize and/or correct the widening of the body fractures will prevent anatomic reduction of the condylar fractures and subsequent occlusal and functional complications.
Bilateral condylar process fracture
CT and/or digital volume tomography (DVT) is extremely useful especially in cases of high and/or intracapsular fractures of the condyle.
This coronal view demonstrates bilateral condylar process fracture with displacement. On the patient’s right side there is a condylar neck fracture with angulation and on the left side there is sagittal condylar head fracture medial to the lateral pole. On the right side, the height of the mandible is not reduced.
The increased width of the mandible in ramus/condyle region may indicate that there is an associated fracture in the anterior mandibular arch.
Subcondylar fracture
Detail of a panoramic x-ray showing a subcondylar fracture.
Neck fracture
Example of (low) neck fracture
Plain x-ray taken at 90° to demonstrate displacement of condylar process fracture.
… and panoramic views of a (low) neck fracture.
Example of a (high) neck fracture
3-D reconstructions are useful in identifying fracture height, direction and severity of displacement.
This 3-D reconstruction illustrates a (high) neck fracture with displacement. Note the associated anterior body fracture of the contralateral side.
Nondisplaced, nondislocated fracture
Nondisplaced, nondislocated fractures suggest the presence of periosteal support for stability and may not require open treatment.
X-ray in the PA plane shows no vertical shortening.
X-ray shows that no displacement occurred.
Biomechanics
Hunting bow concept
The mandible is similar to a hunting bow in shape, strongest in the midline (symphysis) and weakest at both ends (condyles). The most common area of fracture in the mandible is therefore the condylar region.
A blow to the anterior mandibular body is the most common reason for condylar fracture. The force is transmitted from the body of the mandible to the condyle. The condyle is trapped in the glenoid fossa. Commonly, a blow to the ipsilateral mandible causes a contralateral fracture in the condylar region. If the impact is in the midline of the mandible, fractures of the bilateral condylar region are very common.
Clinical findings
Direct trauma to the TMJ area is unusual but may be associated with fractures of the zygomatic complex.
With a condylar fracture, there is very often shortening of the ramus on the affected side. This will result in an ipsilateral premature contact of the teeth. In case of bilateral fractures, the patient may present an anterior open bite. The condylar fragment may be displaced (most often laterally) based on the angulation of the fracture and predominant muscle pull.

