PHYSIOLOGY OF LABOUR. METHOD OF HYGIENICAL ESTIMATION OF WEIGHT AND TENSION OF LABOUR WITH THE PURPOSE OF PROPHYLAXIS OF OVERSTRAIN AND INCREASE OF CAPACITY. HYGIENICAL REQUIREMENTS TO THE MODE OF LABOUR. A METHOD OF HYGIENICAL ESTIMATION OF DANGEROUS AND HARMFUL FACTORS OF OCCUPATIONAL ENVIRONMENTAL AND REACTION OF ORGANISM TO THEIR INFLUENCE. A SANITARY LEGISLATION ABOUT A LABOUR PROTECTION. PROFESSIONAL DISEASES AND POISONINGS BASES OF PREVENTIVE SANITARY SUPERVISION. METHOD OF EXAMINATION OF BUILD PROJECTS. METHOD OF SANITARY INSPECTION OF THE INHABITED PLACES AND HABITATION.
The work environment
Occupational hazards are often encountered in industry, agriculture, mining and other working environments. The major categories of environmental stress for a worker are: chemical agents; physical agents and conditions; biological agents and conditions; and psychosocial factors. They may act either singly or in combination.
The result of occupational accidents are caused by both environmental and human factors as often, as each of factors separately. The interaction between man and his working environment may lead to improvement of health, when work is fully adapted to humaeeds and factors, or to ill health, if work stresses are beyond human tolerance. Occupational diseases and injuries result from specific exposures at work. In addition, work exposures may aggravate certain illnesses or be a factor of varying importance in causing diseases of multiple etiologies.
Psychosocial Factors
A high degree of mechanization may increase psychosomatic disorders, reduce job satisfaction, and contribute to a higher rate of absenteeism. Factors such as inter-personal relations at work, work stability, shift work, speed, and safety are important. Workers engaged in repetitive tasks, controlled by machines, derive less satisfaction from their work.
Shift work creates a psychosocial working environment that may adversely influence the health of a worker. Night work, and the change of working hours from one shift to another, may subject the workers to certain stresses. Such stresses affect the nervous system, increasing the frequency of peptic ulcer and of nervous symptoms, such as fatigue, nervousness, irritation, and insomnia. These nervous symptoms are usually related to the lack of sleep, which in turn may be related to housing conditions, and especially to disturbance of sleep by noise during the day, if the worker is oight shift .
Gastro-intestinal diseases are part of multiple etiology, and the work environment may be a contributing factor, especially where there is emotional or psychological stress at work. Shift workers may have a higher incidence of peptic ulcer than day workers. Chronic gastritis and, to some extent, peptic ulcer were found in Egypt among night shift workers, and were attributed to the stress of a shift work as well as to the dietetic habits.
Effects of Exposure to Combined Stress
Workers are often exposed to more than one kind of stresses; then the outcome is complex. Human tolerance also varies. Workers may be easily affected by minor degrees of stress because of the lowered ” vital ” status of the exposed individuals. The environmental stress in this case does not cause the illness, but rather brings about, in vulnerable groups a rapid shift from the previously tolerated levels of existing illness, or of subclmical impairment, to a state of Usability. Such acute events have often occurred as a consequence of different environmental stress factors acting on individuals with quite different kinds of physiological handicaps. In developing countries, the employment of children, women, the elderly and the partially disabled is common. The degree of tolerance and susceptibility to psychological and physical stresses at work varies in these groups, and may result in health impairment and increased labour turnover.
The stress associated with night work was found, in a study carried out in Egypt, to contribute to a high incidence of high blood pressure; in this study of garage workers, exposure to toxic substances may have contributed to the high incidence of respiratory diseases that was found. In the viscose rayon industry, exposure to carbon disulfide has been associated with an increased incidence of atherosclerosis and cardiovascular diseases, in reports from studies carried out in different countries. The incidence of cardiac deaths among workers exposed to nitroglycol in the dynamite industry is reported to be higher than among the general population . Diet, smoking and mental strain may be a contributing factor in these diseases, although their importance in this connection remains to be determined.
Occupationally exposed groups are affected by the diseases prevailing in the community and, in some developing countries, by malnutrition. Exposure to dusts or gases, to heat stress, to the stress of physical effort, and to other conditions that are well tolerated by healthy individuals, may cause serious complications among workers suffering from, e.g., pulmonary tuberculosis, cardiovascular disease, damage to organs, such as the liver and the kidneys, as a result of parasitic diseases, or malnutrition. Tuberculous workers suffering from massive pulmonary fibrosis may develop silicosis more quickly than those who doesn’t suffer from lung disease. Cardiac patients are more liable to heart failure if they are required to exert considerable physical effort in a hot environment; the diabetic can suffer complications on night-shift work; and the worker whose liver and kidneys are affected by dysentery or other parasitic infestations may suffer from acute degenerative disease if exposed to carbon tetrachloride, mercury, and other toxic substances that might be tolerated by healthy individuals.
Appendix 1
Methods of assessment of work intensity and tension
Obligations of doctors of medical and sanitary departments of enterprises include necessity of assessment of work intensity, its physiological value, level of functional load of the working man organism, in other words to give quantitative evaluation of man’s work.
Such assessment is necessary when solving questions of working and rest conditions, duration of working time for women and adolescents, substantiation of working day duration, tariffication of work at substantiation of benefits concerning vacations and extra compensations, control of industrial environment factors.
Functional exertion of organism at work time may be characterized from two sides – energetic and informational. The first one prevails at physical and the second one at mental work.
Characteristics of the work that requires intensive mental work during receiving and analyzing information, physiologists call “tension”; body burden at work that requires muscle force and correspondingly energy supply – “intensity”.
As it was mentioned at the previous lecture, all types of work by their intensity are divided into light, medium complexity, heavy and very heavy, according to their tension – non-tensioned, slightly tensioned, tensioned and super tensioned.
For assessment of level of the work intensity and tension, ergonometric and physiological methods are used.
Ergonometric characteristics of work intensity are characterized by lading weight, work intensity, kind of working posture, value of static load.
Work power at physical labour is calculated by formula:
N = ![]() ,
,
where N – work power in Wt;
А – work in J;
Т – work time in sec.
Work, as physical concept, is mass transfer in space, considering terrestrial attraction, and is calculated by following formula:
А = 9.8×(Р×Н + ![]() +
+![]() )×6,
)×6,
where Р – mass, kg;
g – acceleration of gravity, = 9.8 m/sec2 ,
Н – hoisting height of the load, m;
L –horizontal transfer distance, m;
6 and 9.8 – scaling factor in J.
Static load value is calculated by multiplication of force value and holding time, and is expressed in kg/sec.
Characteristics of working posture and transfer in space are based on observations, measurements of body angle, transfer distance, timing etc.
Ergonomic indices of labour tension:
1. Number of objects under simultaneous observation.
2. Duration of concentrated observation or time of activities (in % from overall time of the working day).
3. Density of signals (announcements) per annum.
4. Emotional stress.
5. Interchangeability.
6. Tension of analyzers’ functions.
7. Memory volume required.
8. Intellectual tension.
9. Monotony etc.
Main indices of labour intensity are power and static load value as well as intensity (Density of muscular force per time unit).
Main indices of labour intensity definition are those ones of attention, density of processed information signals and emotional stress characteristics. Other criteria are additional.
To find out to which category belongs one work or another, it is necessary to use the most informative main indices, or two additional ones.
It is suggested to consider the level of physiological functions during work as physiological criteria of the level of intensity and tension of the work. Rating scale of intensity and tension of the work, developed by Kyiv Scientific and Research Institute of Occupational Hygiene and Diseases, provides for determination of pulse rate, energy expenditure, indicator of static force resistance, latent period of sensorimotor reactions, indicator of memory, attention etc. And at the same time physiological factors are determined at the beginning and at the end of the working day.
Based on the change level of researched functions after completing the working day category of the work is determined (in %). Such factors as pulse rate and energy expenditure are evaluate in absolute values.
Appendix 2
Method for assessment of fatigability during physical labour
Dynamometry. To measure muscle strength of the hand, spring-type hand dynamometer is used. Maximum hand power is defined by dynamometer scale in kg. Static muscle endurance of the hand is measured by the period during which tested person is capable to keep fast dynamometer at 75 % of maximum hand strength (figure 32.1-а).
Muscle strength and static muscle endurance of the whole body is measured by stationary dynamometer, which is very easy in operation: power of the hand measured by “lifting” facility, fixed by legs (figure 32.1-b).

Figure. 32.1 Dynamometers (a – hand; b – stationary)
Dynamometric measurements are carried out at the beginning and at the end of the working shift. At the training – before and after load (20 squats with
Ergography is defined as measurement of muscle efficiency using ergograph – device of desk-size. Еrgograph is twine sheave fixed on a special support, on one end of which hangs a load of a definite mass and another end has a loop for finger or a hand of the tested person. A twine is connected to a pen that records ergogram on a kymograph – frequency and flexion degree of a finger of a hand when lifting a load.
Decoding of ergograms that were taken at the beginning and at the end of the working shift allows determining muscle strength, fatigability resistance, fatigability, level of fatigability resistance resumption, content of done work and level of resumption of the done work content (fig. 32.2).
Fig. 32.2 Ergogram (1, 2) according to M.V. Lanyk
(average height of the second, third and fourth myograms at fulfillment of the first (ab) and the second (a1b1) works; fatigability resistance at the first (bc) and the second (b1c1) works )
These data are calculated according to depth of myograms in mm and their changes with time in seconds or minutes in the process of research.
Metering of strength and static endurance of muscles is also carried out by special device – dynamo-chromo-reflex meter. Force and duration of pressing hand dynamometer is registered by pointer microammeter (see fig 40.1.1а in “Hygiene of children and adolescents” section).
Physical working capacity and fatigability development are also determined by dynamic analysis of cardiovascular system:
– heartbeat frequency (pulse) before and after load and its restitution;
– systolic and diastolic blood pressure, systolic and minute blood volume, oxyhemometry.
Also electric cardiography is used (students study it in the department of physiology and in clinical departments) for determination of lung capacity, respiratory minute volume, respiration rate, ventilation of lungs by Douglas or Orsay-Fisher techniques, energy expenditure by means of the respiratory metabolism detection.
Electric tremormetry is detection of frequency amplitude of involuntary shaking of hands, inferior limbs allows to assess both level of physical fatigue and functional state of nervous system. Tremor of hands is determined using a special device ‑ electric tremormeter (fig. 32.3), which consists of metal plate of circa 20 х
Tremor of hands of not tired person is less than 3-5 swings (touches) per second, and of tired person ‑ 8-12 and even more swings per second.
Fatigue at mental and operator’s work is detected by series of psycho-physiological tests. (see Appendix 3).
Fig. 32.3 Electric tremormeter
Appendix 3
Attention analysis by search of numbers
Method gives an idea of extent and tempo of psychical processes. Its principle of operation is: tested person must find out numbers in ascending (and descending) orders on the table, where they are placed random, to point them and to call them as quickly as possible.
For the examination, it is necessary to have a stopwatch, a pointer and tables with numbers (fig. 32.4). A table is shown at the distance of
Fig. 32.4 Table for attention analysis by the search of numbers technique
Examination results are evaluated as follows. Numbers’ search in one table, on average less than 45 sec. is a good result, 45-55 sec. – satisfactory, more than 1 min. – unsatisfactory.
Examination of attention by search of numbers with switching
This method is aimed to determine an extent, switching and distribution of attention. Red and black tables with figures from 1 to 24 are demonstrated to the tested person. He must find out black and red figures, calling in turn first black figure than red one. He must find out black figures in ascending and red ones in descending orders (see fig. 40.2. in “Hygiene of children and adolescents” part).
The tested person obtains instruction:” You’ll see a table where 24 black and 24 red figures are located random. On the table you must point at and pronounce aloud all black figures in ascending order starting from one and all red figures in descending order starting from 24. No need to call the color Try to do this as quickly as possible”. An operator controls performance of the task with a stopwatch.
When assessing results, time of the task performance, number and character of mistakes are taken into consideration. Fulfillment of the task during 2 minutes shows adequate quality of attention, more than 3 minutes – insufficiency of attention functions. Mistakes in color are not serious if they are minor. More serious are mistakes of the order called figures. For example, some of the tested people in the middle of the table start calling figures of both number sequences in ascending or descending order. Such mistakes if the tested person does not correct them and continues to do them till the end of the examination testify about attention switch difficulties, i.e. about his physical or emotional fatigue.
Appendix 4
Examination of memory by memorization of geometric figures
This method is used for assessment of functional state of central nervous system (CNS) at the time of work when researches are carried out during the whole working day. At that it is necessary to underline that this test helps to study short-term memory capacity. This method allows determining extent of fatigue of the workers of operators’ professions.
The set of triangles with different hatch is shown to the tested person (fig. 32.5). His attention is paid to the difference between them. After that he is offered to remember 6 triangles with different geometric patterns during 8 seconds and after that to pick them out from the set that was shown at the beginning of the test.
Decrease of number of figures picked out correctly after 8-second remembering during working day may testify about dominance of inhibition processes in CNS as the result of growth of fatigue.
Fig. 32.5 Set of triangles
Appendix 5
Criteria of work classification according to its levels of intensity and tension
|
Criteria |
Work category |
|||
|
Light, non-tensioned (I) |
Medium complexity, slightly tensioned (ІІ) |
Heavy, tensioned (ІІІ) |
Very heavy, super tensioned (IV) |
|
|
External work power, Wt, where shoulder girdle, inferior limbs, body muscles are mainly attracted, maximum weight of the moved load, kg |
Work intensity |
|||
|
Up to 0.17 Up to 0.34 |
Up to 0.37 Up to 0.75 |
Up to 0.75 Up to 1.5 |
More than 0.75 More than 1.5 |
|
|
Static load. Value of static load per shift by keeping load by one hand, both hands, with the help of body muscles, legs |
Up to 5
|
6 – 15
|
16 – 40
|
More than 40
|
|
Working posture |
Stationary workplace, free position |
Stationary workplace. Forced forward inclinations of body (30о inclination angle) (50-100 times) per shift or being in inclined position during the period of time that covers 10-25% of working time of the shift. Transitional working place, walking up to |
Stationary workplace. Forced forward inclinations (about 30о inclination angle) 100-300 times per shift or being in inclined position during the period of time that covers 25-50% of working time of the shift. Staying in forced position (being on the knees, on tiptoes, hanging in the carrier, lying etc. (during the period of 50% of working time of the shift). Walking 4- |
Stationary workplace. Forced forward inclinations (inclination angle of 30оand more) 300 times per shift. Staying in inclined position more than 50% of working time of the shift. Staying in forced position (being on the knees, on tiptoes, lying, etc). more than 50% of working time of the shift. transitional, walking more than
|
|
Quantity of objects of simultaneous observation, duration of attentive observation, % of shift time, time of activity, %, time of signal (announcement) density variability per hour. Emotional stress. |
Intensity of work, work according to individual plan |
Work according to set schedule with opportunity of its correction in the process of work. |
Work conditions with strict timing, hyper-responsibility. |
Personal risk, danger, responsibility for safety of other people |
|
Tension variability of functions of analyzers |
Morning 7- |
Two shifts (excluding night shift) |
Three shifts (including work at night) |
Irregular shift work with night shift work. |
|
Visual |
Rough, without disadvantages |
With low accuracy |
Accurate |
With high accuracy |
|
Auditory |
No obstacles, discrete word intelligibility is 100%, there is background noise when speech can’t be heard at the distance of 2,5 m . There are obstacles when speech intensity level (SI) is 10-15 dB higher thaoise level (N), discrete word intelligibility is 70-80% |
There are obstacles when speech can’t be heard at the distance of
|
There are obstacles when speech can’t be heard at the distance of 1.5 m because of background noise. Discrete word intelligibility below 30% (N>SI on 5 db)
|
|
|
Operational memory capacity |
It is necessary to remember up to 2 elements during less than 2 hours |
It is necessary to remember up to 2 elements during 2 hours |
It is necessary to remember up to 3-5 elements during more than 2 hours |
It is necessary to remember more than 5 elements during one working shift |
|
Intellectual tension |
No need to make decisions
|
Solving simple tasks according to an instruction |
Solving complex tasks according to algorithm |
Creative work |
|
Monotonous work |
|
|
|
|
|
Quantity of operation elements
|
More than 10 |
10-6 |
6-3 |
3-2 |
|
Repetitive duration of fulfillment of operations, sec. |
More than 100 |
100-46 |
45-20 |
20-2 |
|
Time of passive observation of working process, % of shift duration |
80 |
90 |
95 |
98 |
Appendix 6
Quantitative assessment of intensity of physiological functions
|
Level of intensity of physiological functions |
Average value of energy expenditure, Joule/sec. |
Average pulse rate per 1 min., per shift |
Change of functions after working day completion |
||||
|
Decrease |
Increase |
||||||
|
Muscle endurance |
Operational memory capacity |
Latent period of Simple visual and motor reaction (SVMR) |
Latent period of Complex visual and motor reaction (CVMR) |
Time of attention concentration distinction |
|||
|
І |
up to 174 |
up to 80 |
up to 10 |
up to 5 |
no increase |
up to 5 |
up to 5 |
|
ІІ |
175-290 |
81-95 |
11-30 |
6-25 |
1-25 |
6-30 |
6-25 |
|
ІІІ |
291-406 |
96-110 |
31-50 |
26-50 |
26-50 |
31-60 |
26-50 |
|
IV |
407 and > |
111 and > |
51 and > |
51 and > |
51 and > |
61 and > |
51 and > |
Heaviness and labor tension
Ergonomic and physiological metods are used to determine the heaviness and tensity of degree estimation of the labor .Ergonomic method allows defining a degree of psychophysiologocal loading on a man. Therefore they also use the ergonomic time-study of work process. Determine duration of separate elements of work operations in different periods of workday considering the condition of functional organism systems during labour activity. Main ergonomic labor heaviness indeces are: power of external work, translocating loads mass, size of static loading and description of work pose.
Leading ergonomic labor tension indeces are number of objects of simultaneous supervision, category of visual works, duration of concentrated supervision and active motions, number of objects of simultaneous supervision, signals (reports) density for a certain period of emotional and intellectual tension, labor monotony, which is determined by a number and repeating of discrete elements of work operations, duration of their execution and time of passive supervision.
As physiological criteria of heaviness and labor tensity degree estimation they use dynamics indeces changes of physiological functions during a workday. Physiological labor heaviness indeces are considered to be energy expense sizes, descriptions of physical capacity, static endurance and frequency of heart contractions. Labor tension is evaluated according to volume of operative memory, latent periods of general and differentiated visually- motoric reaction, switching and stability of attention .
Volume of efficient memory can be defined by a method of remembering of geometrical figures. Investigated person is proposed to view a set of triangles with different shading. He has to memorize 6 triangles during 6-8 seconds, then he has to choose triangles from a set of 36 triangles and compose them in same sequency .
Latent period of simple visually motored reaction is determined by chronoreflexometrs of different constructions. Time between serving of light signal and beginning of motion reaction is evaluated. Experiment is held 10 times and then middle time is estimated.
For determination of latent period of differentiated visually-motored reaction investigated person is proposed a stereotype irritants series, which consist of positive (for example, white and green) and negative (for example, red) irritants. Calculate a middle duration of latent reaction period and count up, amount of false decisions.
Study of attention functions by searching method allows to realize the condition of its switching speed. Investigated person is offered, to find , to show and to name 25 will placed numbers as soon as possible . Researches are repeated with three different tables and then the mean numbers of the searching time are determined. Labour heaviness (light, middle, difficult, very difficult) and tenacity (unstrained, strained, lustily strained) are determined by limitative indeces, the descriptions of labored activity, that indicate the greatest heaviness and tension.
MEMORY PROPERTIES
1. Research of shot duration memory
A Method is based on recreation of figures (two-digit ciphers). For the experiment the demonstration tables, with 12 two-digit ciphers, or rical figures are used. For each investigation a table is proposed , which a person attentively studies during 30 sec.
|
67 |
51 |
42 |
|
56 |
24 |
96
|
|
83 |
74 |
39
|
|
28 |
49 |
63
|
Later investigate is offered to cover the table and to recreate the ciphers. Investigated records on 12 figures cells, which it memorized into on advance prepared form with. For analysis amount of right named ciphers are taken into account. Percentage of right recreated ciphers is summer up.
2. Research of long-term memory
Investigated is offered to reproduce the ciphers, which were offered before on the following day. Among ciphers, which will be reproduced from memory only those, which a person memorized from the table are taken into account.Supply Form and results estimation are anagogic to previous.
3. Casting memory
Investigated is given a card with 10 couples of word written on it.
For example: Lock-door,
Hour-day,
Lake-fence,
Animal-forest,
Eye-ear,
Night- star,
Pen – calculator,
Way-road,
arden-flowers,
Rain – umbrella.
On a table in front of investigated person there are cards, placed with blank side up, on which the first words of each words couple of are written. The Teacher reads out words couples and is proposes to students to tip over the cards with textual page and to add to each word a suitable couple. Experiment takes 30 sec. The Results are evaluated by amount of right reproduced couples. Record form and results estimation to previous task.
Results are recorded into beneath brought table.
|
Amount of given words |
Amount of right reproduced words |
|
|
|
Index of rich in content memory is a coefficient of verbally-logical imprinting, that is determined by dint of number dale right reproduced trace on amount of given words couples.
ATTENTION PROPERTIES
1. Attention steadiness
Necessary for work is: Anfimov tables and stopwatch.
Investigated on extent of 2 min with most (possibly) speed and exactness must delete in form two certain letters, for example “k” and “е” not missing the lines. After command “start” task takes 2 min. After got through time an experimenter gives a command “stop”.
The results are recorded into following table:
|
General amount of looked through signs (P) |
Quantity of right marked signs (A) |
Amount of admitted mistakes |
|
|
Quantity of pretermited signs (B) |
Quantity of wrong deleted signs (C) |
||
|
|
|
|
|
Determine work exactness (T) and work productivity (E).
Work exactness calculed by formula:
T =A/(A+B+C)
Where A- amount of right marked signs;
B- amount of wrong pretermited signs;
C – amount of wrong deleted signs.
Work productivity calculed by formula:
E = P x T
Where P- general amount of looked over signs;
T- work exactness.
2. Switching of attention
Work is hold by the means of Platonov-Shults table.
For experiment they use 3 tables with variously located red and black colored numbers.For the 1 table the task is to find as quick as possible black ciphers in growth order.
On the ІІ table the investigated person must find the black ciphers in falling order.
For the ІІІ table the task is to find the black ciphers in falling order and red ones in growth order simultaneously.
For speed estimation of switching attention they use results of performed task. Fix time (A), that is used by investigated person on execution of task for finding of black ciphers in ascending order from 1 to 25. Time (B) expended on finding of red ciphers in falling order from 24 to 1 and time (C) expended on mix counting of black and red ciphers from 25 to 1, changing black and red cipher.
Switching (T) time is counted up by formula:
T =C – (A+B)
Where C- time expended on execution of task on mixed table “C”;
A- task execution time on table “A”;
B- task execution time on table “B”.
3. Research of attention (Kholina`s test )
Investigated is offered 2 tables. One is on the table turned with clean side up the teacher keeps the other one. In each table ciphers from 1 to
HEAVINESS (light, middle, difficult, very difficult) and labor TENSITY (tense, little strained, strained, very strained) is determined by limit active indeces, meaning those descriptions of labored activity, that indicate on most considerable heaviness and tension.
There is great amount of other methods for evaluation of attention estimation, information alteration speed, different memory types and other, which can be found in psychological practical works and methods on study of physiology-hygienic aspects of professional people activity.
4. Determination of exactness and motions coordination with the help of phonotremometer
Takes into account a passing speed on labyrinth and amount of touches to walls.
Strikes off an index of phonotremometery ( I ).
I = (1/ passing time on labyrinth + 1/amount of touches to walls of labyrinth) x 100%
Criteria of an estimation of the basic psycho-physiological parameters at students
|
Parameters |
Degree of expressiveness of parameters |
||
|
Good |
Satisfactory |
Unsatisfactory |
|
|
Kholina`s test (%) |
75-100 |
50-74 |
Less than 50 |
|
Platonov-Shults`s test (sec) |
Less than 25 |
25-32 |
More than 33 |
|
Index of phonotremometery |
More than 10 |
8-10 |
Less than 8 |
Occupational Accidents
Accidents result from both environmental hazards and human factors. The contributing environmental factors include the layout of the workplace, unsatisfactory machine guards, inadequate maintenance of equipment, defective lighting, excessive noise and vibration, unsuitable floors, walls, celeings, etc. On the the other side, we must include poor adaptation to the industrial mechanized environment, a casual attitude towards work, and incorrect methods of work. In addition, the physical and physiological capacities of the worker may not face the job requirements; thus his visual acuity may be inadequate, this worker may suffer from hearing loss or other forms of partial incapacitation, and his psychological state, particularly his alertness, may be unsatisfactory.Despite this,the failure to observe safe practices and to make proper use of mechanical safeguards and personal protective equipment account for many accidents. Most authorities consider human factors much more important than environmental hazards in accident causation, the former being possibly responsible for 85 % of all accidents.
Hygienic classification of work
(by indeces of harmfullness and danger of factors of industrial enviroment, hardness and effort of working process).Terms and determination of main definition used in classification.
Dangerous and harmful factors of working conditions can be physical, chemical, biological factors of industrial environment, psycho physiological factors in work organization, working places staff and equipment.
Harmful industrial factor is factor, which influence on the worker in the indicated condition can cause illness or firm decreasing of capacity.
Dangerous industrial factor is a factor, which influenced on the worker can cause trauma or other sudden worsening of health.
Difficulty (heaviness) of work – a line of working process, which reflexes loading on borne-muscular system and functional system (cardiovascular, respiratory, etc.), which provides its action.
Tensity of work – is a characteristic of working process, which reflects loading on the central nervous system.
Classification is necessary for hygienic estimation of real conditions and kind of work on working places, determining of priorities in holding of sanitary condition. The base of hygienic classification is presented by harmful factors of industrial environment, the lever of difficulty and tensity of working process.
Principal of condition differentiation and kind of work foresee degree deflection of sizes of industrial environment and working process from active hygienic norms and influence on functional state and health of workers.
There are three types of conditions and kinds of work.
I – optimal condition and kind of work, where unpleasant influence (on worker’s health) of harmful and dangerous industrial factors on worker’s health is absent. Apiaries condition for keeping high level of capacity (absent or according to level, which is good for population.
II – permissible conditions and kind of work when level of dangerous and harmful industrial factors don’t overcome hygienic norm on working place. And possible functional change caused by working process, renovate during Brea time, during working and home rest before beginning next shift and don’t cause unpleasant influenced in the next period on the health of working and their children.
III – harmful and dangerous conditions and kind of work due to which sanitary norm and rules possible influence of dangerous and harmful factors of industrial environment in the quantities which increased hygienic norm, psychophysiological factors of working action, which causes functional changes in the organism, which can lead to firm of decreasing capacity and disorders of working health.
There are three degrees of harmful and dangerous conditions of kind of work:
I – conditions and kind of work, which cause functional violations which have a reverse character during early indication and after interruption of influence.
II – conditions and kind of work, which cause functional violation, which assist increasing indexes of morbidity with temporary loosing of work capacity and in some cases appear ance of signs or easy form of professional diseases.
III – conditions and kind of work with increased danger of development of professional diseases, higher illness with temporary of working lass.
In case of presence of two or more dangerous and harmful industrial factors and factors of working action condition of work it is necessary to hold according estimation to higher class and degree.
Classification exclude work in extreme conditions during which combination of conditions and kind of work forro high risk of development of hard form of acute professional diseases, handicapness and danger for life. Degree of risk in extreme condition of work caot be characterized quantitative indeces of harmfullress, danger, difficulty and tensity of work.
Criterias classification of work according to difficulty and effort
|
Criterions |
Class of work |
||||
|
Easy effort |
Middle easy effort |
Hard effort |
Very hard effort |
||
|
Physical work Power of external work, Wt, in which shoulders part, Inferior extremities and trunk take part |
< 0,17
< 0,34 |
0,18 – 0,37
0,35 – 0,75 |
0,38 – 0,75
0,76 – 1,5 |
> 0,75
> 1,5 |
|
|
Maximal weight of moving load, kg |
Less than 5 |
6 -15 |
16 – 40 |
> 40 |
|
|
Static loading Value of static loading for shift during holding of load by one hand, by two hands, by means of muscles of trunk and legs |
< 18000 < 43200 < 61200 |
< 43200 < 97200 <129600 |
Before 97200 Before 208800 Before 266400 |
>97200 >208800 >266400 |
|
|
Working pose |
Stationary-working place |
Stationary working place, strained slope (angle of slope 300) 50-100 times in a shift or stay in slope during 10-25% from time of working shift. Stationary working place, walking 4km in a shift |
Stationary working place, strained slope (angle of slope 300) 100-300 times in a shift or stay in slope during 25-50% from time of working shift. Stay in strained pose (on knee, lay during) before 50%, walking from 4 to |
Stationary- working places, strained slope (angle of slope 300 and more) 300 times in a shift or stay in slope more half of working time. Stay in strained pose (on knee, squat, lying) more half of time shift. Stationary place, walking |
|
|
Attention |
Work tension |
||||
|
Quantity of simultaneous observed objects |
To 5 |
From 5,1 to 10 |
From 11 to 25 |
>25 |
|
|
Durability of observing (% from shift) |
To 25 |
26-50 |
51-75 |
>75 |
|
|
Durability of active action (% from shift) |
From 10 to 20 |
21-50 |
51-80 |
>80 |
|
|
Density of signal for 1 hour |
To 75 |
To 175 |
To 300 |
>300 |
|
|
Emotional effort |
Work according individual plan |
Work according to putting scheduler with possibility of its correction for action |
Work in condition of deficiency time with increased responsibility |
Personal risk, danger, responsibility for safety of other peoples |
|
|
Replacement |
Morning 7-8h. |
Two shifts (without night) |
Three shifts (with night work) |
Regular replacement with night work |
|
|
Tension of function of visual and hearing analisator |
Coarse, absence of outside noises
Noises are absent, legible of words to 100% |
Almost the exact. Have outside noises, through them can hear-speech to 2,5m There are noises, level of speech intensity (P) on 10-15DB more level (P>S). Legible of words 70-80% |
Exact Exact Hear speech to 2m
There is noise, word legible 30-60% (P=S)
|
High exact High exact To 1,5m
There is noise, word legible less 30% (S>P on 5DB) |
|
|
Amount of operative memory |
Necessary to keep in mind 2 elements during 2 hours |
Necessary to keep in mind 2 elements during 2 hours |
Necessary to keep in mind 3-5 elements during 2 hours |
Necessary to keep in mind 5 elements during shift |
|
|
Intellectual tension |
Absence of necessity to take decision |
Solution of simple tests according instruction |
Solution of simple tests according order |
Creative work |
|
|
Monotonoulity Number of elements in way |
More than10 |
6-10 |
3-6 |
2-3 |
|
|
Durability of operation making which repeats |
More than 100 |
46-100 |
20-45 |
2-20 |
|
|
Time of passive observation for course of industrial process in % to shift durability |
80 |
90 |
95 |
98 |
|
http://www.britannica.com/eb/article-9108516/occupational–disease
Occupational exposures contribute to the morbidity and mortality of many diseases. However, occupational diseases continue to be underrecognized even though they are responsible for an estimated 860,000 illnesses and 60,300 deaths each year. Family physicians can play an important role in improving the recognition of occupational disease, preventing progressive illness and disability in their own patients, and contributing to the protection of other workers similarly exposed. This role can be maximized if physicians raise their level of suspicion for workplace disease, develop skills in taking occupational histories and establish routine access to occupational health resources.
The patient with a possibly work-related illness frequently seeks care initially from a family physician. The physician’s recognition of a possible link between work and disease often determines the diagnostic tests that are performed and the treatment that is recommended. Early diagnosis of an occupational illness may prevent progressive morbidity and disability from conditions such as occupational asthma and may facilitate the reversal of adverse effects from exposures to substances such as lead.1 The identification of an occupational illness in one patient also provides the physician with an opportunity to protect other patients with similar exposures.2 Since much remains to be learned about the effects of toxins on health, the family physician is in a crucial position to contribute new information about occupational disease.
A variety of factors are responsible for the present underrecognition of occupational illnesses. Some of these factors include the difficulties physicians can encounter in dealing with the Workers’ Compensation system, the reluctance of patients to connect a health problem with their work (primarily because they fear they will lose their jobs) and the present managed care environment, which reduces the time available to take a complete occupational history.
This article describes ways in which family physicians can improve the detection of occupational disease in their patients. In particular, physicians need to raise their level of suspicion for occupational disease, build skills for efficiently obtaining an occupational history and develop routine access to occupational medicine resources.
Raising the Level of Suspicion
Occupational disease is surprisingly common. An estimated 860,000 illnesses and 60,300 deaths from workplace exposures occur annually in the
Since the spectrum of occupational diseases is extremely broad (Table 1), many conditions commonly encountered in primary care practice may be work related. The following illustrative case is but one example of an illness with an occupational source.
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Illustrative Case
A 38-year-old man reported several weeks of generalized headaches. A diagnosis of stress-tension headache was made, and he was given an analgesic. Because he continued to have pain, computed tomographic (CT) scanning was performed. The CT scan was normal.
The patient was referred to a neurologist and then to a specialty headache clinic. Various treatments were applied without effect.
An occupational history revealed that he had been a spray painter for 11 months. While at work, he was routinely exposed to mixed organic solvents. When he was taken out of work for four weeks, his headaches cleared.
Musculoskeletal Disorders
Patients with musculoskeletal disorders involving the arm and neck frequently seek medical care. Work tasks contribute to symptoms in a significant proportion of these patients. More than 60 percent of reported occupational illnesses are work-related musculoskeletal disorders of various types.14 Specific diagnoses, such as localized nerve entrapment (e.g., carpal tunnel syndrome), tendinitis (e.g., lateral epicondylitis, de Quervain’s tendinitis), muscle strain and less well-defined regional pain syndromes, have been associated with jobs in all sectors of the economy. Repetition, force, awkward or static postures, vibration, work speed and restricted tasks are job factors that may contribute to the development of these ailments.
|
Respiratory Diseases
A variety of respiratory diseases are also commonly occupational in origin. Pneumoconiosis due to inhalation of asbestos, silica or other nonorganic dust should be considered in patients who report progressive dyspnea and dry cough. Airway diseases, including rhinosinusitis, bronchitis and asthma, have been increasingly recognized as work related.
A widening array of exposures has been linked to occupational asthma related to possible exposure to allergens (e.g., grain dust), respiratory irritants (e.g., sulfur dioxide) or substances acting through other mechanisms (e.g., isocyanates). Less frequently, recurrent “flu” or “pneumonia” may actually be symptoms of hypersensitivity pneumonitis from exposure to mold, other organic materials or certain chemicals.
Neurologic Disorders
The nervous system is a frequent target of toxins, including organic solvents (e.g., toluene and chlorinated hydrocarbons), metals (e.g., lead and manganese) and pesticides (e.g., organophosphates). Peripheral polyneuropathy may be caused by agents such as lead, methyl butyl ketone and organophosphate pesticides. More commonly, chronic organic solvent exposure is responsible for a syndrome that includes headaches, fatigue, light-headedness, cognitive difficulties and depression.
Cancer and Heart Disease
Work exposures also contribute to a notable percentage of cancers and have been increasingly recognized as factors in the development of coronary artery disease.
Stress-Related Illnesses
Stress has also emerged as an important hazard in the contemporary workplace. It has been associated with a range of emotional and physical ailments, including coronary artery disease and myocardial infarction. The risk of stress-related illness is increased in jobs with high emotional/psychologic demands and low potential for control by the worker.
Work Conditions and Illness
As the focus of business has shifted from manufacturing to service in most industrialized countries, traditional notions of hazardous work have, by necessity, been expanded. Occupational illnesses continue to occur in manufacturing, construction and agricultural sectors, but they are also increasingly being recognized in the burgeoning service sector. For example, rapidly expanding computer use has been associated with musculoskeletal and eye problems in a growing number of office workers.
Today a significant proportion of occupational illnesses are related to building conditions, such as inadequate fresh-air ventilation, low humidity and the presence of cigarette smoke, volatile organic compounds and fibers, molds or other microbiologic materials.
Typically, workers with symptoms related to indoor air quality report upper airway and eye irritation, frequently accompanied by fatigue and difficulty concentrating. These symptoms generally occur in a group of workers in the same environment. Furthermore, the workers report rapid clearing of the symptoms when they leave the workplace. Other illnesses, including asthma, hypersensitivity pneumonitis and respiratory infections, have also been linked to specific building-related exposures.
Index of Suspicion
An occupational etiology should be considered if an illness fails to respond to standard treatment, does not fit the typical demographic profile (i.e., lung cancer in a 40-year-old nonsmoker) or is of unknown origin. Much is still unknown about the health effects of most workplace exposures. The introduction of new chemicals and other materials has far outpaced general knowledge of their potential toxicity. Consequently, family physicians continue to play a crucial role in recognizing unsuspected links between exposures and specific illnesses.
PROFESSIONAL DISEASES AND POISONING
Lead Poisoning Plumbism
www.faqs.org/health/ Sick-V3/Lead-Poisoning.html
www.epa.gov/reg3wcmd/ lp-whyislead.htm
The best way to know if a person is being exposed to lead is to have a blood lead level (BLL) test. In
Purpose
OLPPP investigates and follows up on reported cases of lead poisoning in individual workers. The purpose of these investigations is to ensure that:
-
- workers receive proper medical care
- conditions in the workplace that resulted in lead poisoning are corrected
- workers do not carry lead contamination home and poison their families.
Case Investigation Activities
To achieve these goals, OLPPP:
- Calls the lead-poisoned worker to address concerns about his or her health, learn about the workplace, and identify household members and co-workers at risk;
- Talks to the employer to review the company’s lead safety measures and make recommendations on how to control lead exposure;
- Contacts the doctor who is treating the lead-poisoned worker to review the case and provide information and assistance.
Saturnism.
Synonyms.—Chronic Lead-poisoning; Saturnism.
Definition.—A chronic intoxication due to absorption of lead.
Etiology.—Individual susceptibility is much greater in some cases than in others, and sleeping iewly painted rooms, or drinking water flowing through lead pipes, has occasioned the disease.
The most common means of receiving the poison, however, is due to contact by workers in lead, such as paint manufacturers, painters, plumbers, workers in type-foundries, shot-makers, pottery-glaziers, lace-makers, calico-printers, glass-grinders, and the habit of dressmakers of biting off thread, some of which is lead-dyed.
It may be taken in the food, in which lead chromate is used to impart a rich yellow color, and may be found in bread, milk, butter, and candy. Chocolate, candy, and tobacco wrapped in lead-foil may also give rise to plumbism.
Women are more susceptible than men, and adults than children, though most likely on account of more frequent exposure rather thaatural susceptibility.
Pathology.—The pathological changes occur in the peripheral nerves, muscles, kidneys, liver, mucous membranes, and bloodvessels.
The most constant changes are found in the peripheral nerves, the nerve-endings exhibiting a neuritis, to be followed by atrophy of the muscles. The cord is usually free from structural change, though degeneration may occur in patches, in the nerve-trunks. The atrophied muscles are pale in color, and, in advanced stages, show fibroid degeneration.
In lead-encephalopathy, arterio-sclerosis of the cerebral bloodvessels is found, which sometimes is followed by softening of the brain, and by hemorrhages. Parenchymatous degeneration of the kidneys and liver is common.
Symptoms.—The symptoms vary, depending upon individual susceptibility, amount of lead absorbed, and the length of time of exposure. Anemia is an early and characteristic symptom, and usually of the chlorotic type. The hemoglobin may be considerably diminished, though the erythrocytes are rarely less than 3,000,000. There is impaired nutrition, with consequent loss of flesh and strength.
An almost constant and characteristic symptom is a blue line at the juncture of the gums with the teeth, and is clue to the presence of lead sulphid, formed by the union of the lead in the blood with sulphuretted hydrogen, the latter resulting from the decomposition of tartar upon the teeth. If the patient’s teeth be free from tartar, the blue line may be absent. The gums are frequently soft, swollen, and spongy, and there is a metallic taste, and the breath is fetid.
Gastro-intestinal symptoms are also characteristic, lead colic causing the most intense suffering. Commencing with an obscure paiear the navel, it radiates in every direction, until the entire abdomen seems involved. The pain is griping and excruciating in character, the patient not infrequently screaming in his agony. The pain may extend to the back, hip, thighs, and legs; in fact, no part of the body seems free from pain.
The abdominal walls are tense and hard, sometimes knotted, and the umbilicus is drawn inward. The bowels are not tender to pressure, neither does pressure alleviate the pain, as in some other forms of colic. The patient is frequently troubled with nausea and vomiting, the material thrown off the stomach being a slimy fluid, more or less mixed with acrid bile. The tongue is pale, broad, and flabby, and its movements controlled with difficulty; the skin is soft and moist, the pulse not at first affected, but when the disease is long continued and severe, it becomes soft, feeble, and increased in frequency.
The bowels are obstinately constipated; if anything passes, it is in hard scybalous masses, with a brownish water; the sphincters seem to be sometimes so contracted that neither urine nor feces can be passed, and it is v/ith greatest difficulty that we can introduce the nozzle of a syringe.
Paralysis is common, especially that affecting the extensor muscles of the forearm, producing wrist-drop. Less frequently the deltoid, the biceps, the brachialis and pectoral muscles are involved.
Saturnine arthralgia, pain in the articulations, is not an uncommon symptom.
Cerebral symptoms, or lead-encephalopathy, occur where large quantities of lead are absorbed, and it is characterized by convulsions, delirium, coma, neuro-retinitis, and sometimes insanity.
|
Figure1. Wrist-drop due to paralysis from lead-poisoning. |
|
|

Diagnosis.—The history of exposure to lead-poisoning, the blue line on the margin of the gums, the wrist-drop, the anemic condition, and the lead-colic are such characteristic symptoms that the diagnosis is easily made.
Prognosis.—Unless degeneration of the heart and kidneys has taken place or severe cerebral symptoms develop, the prognosis is favorable.
Treatment.—”The first object of treatment is to mitigate the intense pain, and open the bowels, after which means to remove the lead should be immediately used. Among the most efficient means for the relief of pain is the administration of chloroform in doses of from twenty to thirty drops every half hour or hour; it may be administered in mucilage, water, rectified spirits, or, what is preferable to all, glycerin. I usually order it in the following” manner:
- Defined as persistent eating of non-nutritive material for 1 month or more
- Always search for lead lines in any child with an ingested foreign body
- Main source of lead intoxication is lead paint used in houses painted before 1980
- Absorption is greater in children than adults
- Lead may be inhaled as well as ingested
- Symptoms develop more quickly through GI tract
- Toxicity more severe with co-existing iron, zinc, or calcium deficiency
- Pathology
- Lead concentrates in metaphyses of growing bones
- Distal femur
- Both ends of tibia
- Distal radius leading to
- Failure of removal of calcified cartilaginous trabeculae in provisional zone
- Clinical findings
- Neurological
- Learning disability
- Decreased IQ
- Mental retardation
- Encephalopathy
- Motor deficits
- Seizures
- Cerebral edema
- Hearing loss
- Gastrointestinal
- Abdominal pain
- Nausea
- Vomiting
- Diarrhea
- Constipation
- Anorexia
- Metallic taste in mouth
- Ileus
- Renal
- Tubular damage
- Azotemia
- Gout
- Hematologic
- Affects blood synthesis
- Hemolysis
- RBC stippling
- Iron deficiency
- Musculoskeletal
- Muscle and joint pain
- Soft tissue
- Blue-black line in gum margins
- Endocrine
- Decreased stature
- Decreased growth hormone
- Decreased vitamin D levels
- Laboratory findings
- Predate bone changes on x-ray
- Serum Lead Level >1.2 umol/L
- Urine lead level elevated
- Peripheral Smear
- Stippled erythrocytes
- Complete Blood Count
- Urine microscopy of sediment or renal biopsy
- Acid-fast inclusion bodies in tubular nuclei
- Pathognomonic for lead poisoning
- Free Erythrocyte Protoporphyrin (FEP) > 0.6 umol/L
- Imaging findings
- Cerebral edema in acute lead intoxication
- Particles of lead in GI tract
- Bands of increased density at metaphyses of tubular bones (growing bone)
- Metaphyses of growing bones may be dense normally
- Lead lines more apt to be seen in proximal fibula and distal ulna where growth is not as great as other long bones
- Lead lines may persist
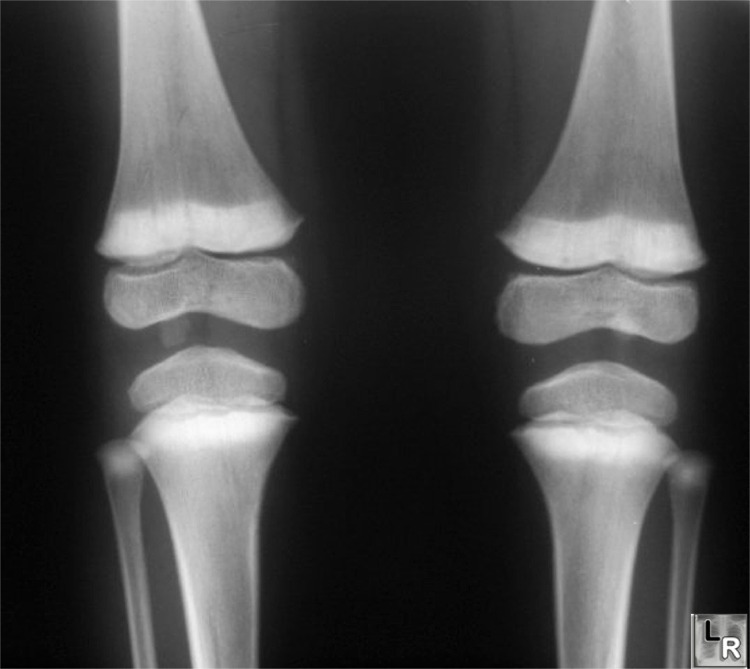
Frontal radiograph of both knees of a child with lead poisoning show dense metaphyseal bands
involving not only distal femurs and proximal tibias but proximal fibulas as well
- Bone-in-bone appearance
- Abnormalities in bone modeling
- Erlenmeyer flask appearance to distal femur
www.lead.org.au/ bblp/silent-epidemic.html
http://www.healthy.hartford.gov/Lead_Poisoning/PbIntro.htm
PNEUMOCONIOSIS
Pneumoconiosis is a disease of the lungs caused by long-term breathing of dust, especially certain mineral dusts. Forms of pneumoconiosis include black lung disease (coal worker’s pneumoconiosis), silicosis, and asbestosis. The disease typically resultsfrom working in a mine for many years, but factory work and other occupations can expose people to the ill effects of breathing dusts. The term “pneumoconiosis” comes from the Greek pneumon, meaning lung, and konis, meaning dust.
What Causes Pneumoconiosis?
Only microscopic-size dust particles, about 1/5,000 of an inch across or smaller, are able to reach the tiniest air sacs (the alveoli) in the lungs. There they cannot be removed, and accumulate to cause a scarring and thickening of the lungs called fibrosis . Eventually, the lungs begin to lose their ability to supply oxygen to the body.
THE WAR AGAINST BLACK LUNG
The prevalence of black lung disease did not begin to decrease until it became clear that the cause was excessively high levels of coal dust in mines. Largely due to the efforts of coal miners’ unions, occupational safety conditions improved.
In 1969, the Mine Health and Safety Act set standards in the United States for maximum allowable levels of coal dust in mines. The Act also provided compensation for miners who developed black lung disease. Death rates from pneumoconiosis have been declining since the Act was passed.
Breathing coal dust was an occupational hazard for coal miners, especially those who did not wear protective masks.
Corbis-Bettman.
Black lung disease is caused by breathing coal dust, usually in mines. Silicosis results from inhaling silica dust from sand and rock, primarily in mines, quarries, and in occupations such as sandblasting. Asbestosis comes from breathing tiny asbestos fibers in mining, building construction, and other industries. Less commonly, other kinds of dust are continuously inhaled in work-related situations and cause pneumoconiosis.
What Happens When People Have Pneumoconiosis?
Symptoms
Because pneumoconiosis usually takes 20 or 30 years to develop, workers often do not notice symptoms until they are over 50. The main symptoms are coughing and difficulty in breathing, which gradually increases. Complications include emphysema and increased risk of tuberculosis. Asbestosis patients are more likely to develop lung cancer, especially if they smoke cigarettes. Damaged lungs make the heart work harder, and heart problems can accompany severe cases of pneumoconiosis.
Diagnosis
Diagnosis is made by physical examination and through a medical history that tells the doctor which dusts patients have been exposed to. The doctor may also take chest x-rays and pulmonary (lung) function tests.
Treatment
There is no cure for pneumoconiosis, because the dust cannot be removed from the lungs. Even if it could, the damage done to the lungs from years of inflammatory reaction to the dust could not be undone. Except in a mild form called simple pneumoconiosis, the disease is progressively disabling. The only treatment is to avoid smoking and further exposure to dust, and to treat complications.
Prevention
Pneumoconiosis can be prevented by enforcing maximum allowable dust levels in mines and at other work sites, and by using protective masks. Regular medical examinations, including chest x-rays for people at risk, can detect pneumoconiosis during its earlier stages, before it becomes disabling.
See also
Emphysema
Environmental Diseases
COAL WORKERS PNEUMOCONIOSIS, COMPLICATED
This picture shows complicated coal workers pneumoconiosis. There are diffuse, small, light areas (3 to
Taking the Occupational History
An illness that fails to respond to standard treatment, does not fit the typical demographic profile or is of unknown cause should raise suspicion of an occupational etiology. An illness that fails to respond to standard treatment, does not fit the typical demographic profile or is of unknown cause should raise suspicion of an occupational etiology.
A standardized set of questions asked of every patient is the single most important method of recognizing the link between illness and occupation. In a busy practice, a set of screening questions and a self-administered questionnaire can be helpful in obtaining an efficient occupational history.
Screening Questions
Key screening questions include the following:
1. What type of work do you do?
2. Do you think your health problems might be related to your work?
3. Are your symptoms different at work and at home?
4. Are you currently exposed to chemicals, dusts, metals, radiation, noise or repetitive work? Have you been exposed to chemicals, dusts, metals, radiation, noise or repetitive work in the past?
5. Are any of your co-workers experiencing similar symptoms?
If the answers to one or more of these questions suggest that a patient’s symptoms are job related or that the patient has been exposed to hazardous material, a comprehensive occupational history should be obtained.
Self-Administered Occupational History
Every patient’s chart should include a self-administered occupational history form that the patient fills out before a visit. The completed form is then available for subsequent review and periodic updating by the family physician or office staff. A sample form for a self-administered occupational history is provided in Figure 1.
|
Comprehensive Occupational History
The elements of the comprehensive occupational history are listed in Table 2.
Job History. A job history, including employer names, dates of employment, job titles and major job duties, serves as the framework for assessing occupational exposures and the risk of illness. The job history should include a list of all positions held, because some occupational diseases, particularly work-related cancers, have long latent periods.
Job duties are distinguished from job titles because titles alone often provide little or misleading information about occupational exposures. Furthermore, workers with the same job title, even within the same company, may have vastly different exposures based on their job duties.
Military service should also be included in the job history. Hazardous exposures are common in military settings (e.g., asbestos exposure iaval shipyards and dioxin exposure in Vietnam).
Exposures. The second element of the history is an assessment of specific exposures. Major exposures should be listed for each job in the job history. The physician should ask for additional details about job tasks that appear relevant to the patient’s current symptoms.
|
TABLE 2 Elements of the Occupational History |
|
|
|
List of jobs Lifetime history, with dates of employment and job duties Military history Exposures Type Chemicals (e.g., formaldehyde, organic solvents, pesticides) Metals (e.g., lead, arsenic, cadmium) Dusts (e.g., asbestos, silica, coal) Biologic (e.g., HIV, hepatitis B, tuberculosis) Physical (e.g., noise, repetitive motion, radiation) Psychologic (e.g., stress) Assessment of dose Duration of exposure Exposure concentration Route of exposure Presence and efficacy of exposure controls Quantitative exposure data from inspections and monitoring Timing of symptoms in relation to work Symptoms occur or are exacerbated at work and improve away from work Symptoms coincide with the introduction of new exposure at work or other change in working conditions Presence of similar symptoms among co-workers with the same type of job and exposures Evaluation of nonwork exposures Home environment (e.g., water, air, soil contamination) Hobbies or recreational activities |
Exposures are recorded for each of the patient’s various job duties. These exposures may include metals, chemicals, dusts, physical factors (i.e., repetitive motion, noise, radiation), microorganisms and stress. Both indirect and secondary exposures should be recorded because the patient’s health can be affected by exposures originating in other parts of the workplace. For example, asthma in a woman assembling spark plugs may be exacerbated by exposure to volatilized products from a molding operation
Exposure dosage should also be assessed. Although a patient may present a list of numerous chemicals used in a workplace, some substances may be used infrequently or in very small amounts, whereas others may be used daily, gallons at a time.
The presence of exposure controls may significantly affect the extent of exposure. Ventilation is a crucial control and includes both general and local systems. The patient should be asked specific questions about general ventilation, including the presence of operable doors and windows, the location of walls and partitions that may affect air flow, and the configuration of the mechanical ventilation system. Workers are usually aware of a local exhaust ventilation system, such as a hood, a vacuum apparatus attached to a machine or exhaust slots on a tank. The patient should be asked whether the exhaust mechanisms are functioning.
Personal protective equipment such as respirators, gloves and earplugs are other commonly used exposure controls. To assess exposure dosage, the physiciaeeds to know whether the patient uses the protective equipment consistently, whether the equipment fits correctly (especially a respirator), whether the equipment is appropriate for the exposure and whether the equipment is stored and maintained properly.
Temporal Relationship of Symptoms to Work. The timing of symptoms in relation to work is often crucial in the assessment of a potential occupational illness. A patient with asthma may state that symptoms appear soon after he or she arrives at work and then abate after the shift and on weekends. The timing of symptoms may be more specifically linked to the use of a certain substance, the activation of a specific process or a change of materials or other work conditions. However, it is important to recognize that as many job-related illnesses progress, the clear relationship of symptoms to work may be obscured by a lack of marked improvement away from work.
Symptoms Among Co-workers. The probability that work is contributing to a common illness is strengthened if the patient’s co-workers are experiencing similar symptoms. When queried, patients with occupational illness commonly report others who are similarly affected.
Nonoccupational Exposures. Nonwork activities may also contribute to illness and therefore should be assessed as part of the comprehensive history. Tobacco smoking and excessive alcohol use contribute to a variety of diseases and may interact with occupational exposures to increase the risk of adverse health effects. Recreational activities, hobbies, unpaid work (e.g., home renovations) and drug use are other potential sources of hazardous exposure. For example, a miner may be exposed to noise both at work (drilling and blasting) and at home (snowmobiling and hunting) or a construction painter may be exposed to lead during bridgework and while scraping and repainting the house. The history should allow the physician to evaluate the relative contribution of exposures, both on and off the job, to an illness.
Additional Exposure Information
It is often desirable to supplement the occupational history with additional exposure data. Patients may have only partial knowledge of the specific substances to which they have been exposed.
With the patient’s permission, the physician can request exposure information from the employer. The Occupational Safety and Health Administration’s (OSHA) Hazard Communication and Access to Medical Record Standards mandate access to this information for both clinicians and workers.
Alternative strategies may be employed if the patient is reluctant to have the physician contact the employer. The patient may make the request for exposure information, or the physician may contact the manufacturer or distributor of the suspect materials. Labels from workplace containers provide the names of appropriate contacts. The patient can also ask representatives of a trade union, if present, to obtain exposure data. Employers are sometimes amenable to a site visit by the physician. This visit can provide valuable exposure information.
In response to a request for exposure data, the physician usually receives a material safety data sheet (MSDS) for each substance used in the workplace. The MSDS identifies the hazardous ingredients and notes potential health effects of the substance. The MSDS is often limited, however. Since many substances remain unstudied and their toxic effects are unknown, they have not been deemed harmful by OSHA. As a result, they are not covered in MSDS materials. The lack of toxicity data is also reflected in the emphasis the MSDS places on acute health effects. The potential effects of chronic lower level exposure often are not included in the MSDS. Therefore, the physician should view the MSDS as an informational starting point that frequently requires supplementation.
In addition to the MSDS, quantitative exposure data are often available. These data typically include levels of air contaminants that are compared to OSHA permissible exposure limits (PELs). However, if the air level of a substance is below the recommended PEL, it should not automatically be assumed that the substance carries no risk of adverse health effects. The limitations of monitoring techniques and OSHA’s standard setting process frequently call this assumption into question.22 Consequently, even if air levels of various substances are below the PELs, a patient whose history is consistent with a work-related illness is likely to be experiencing the adverse effects of exposure.
Occupational Health Resources
The need for consultation or referral depends on the physician’s skill, confidence and time, as well as the specifics of a given case. A telephone consultation or referral to an occupational medicine specialist can provide information on the extent of a patient’s exposure, the likely health effects of the exposure, appropriate diagnostic tests, possible workplace interventions to reduce exposure and recommendations on the patient’s return to work. Corroboration by an occupational medicine specialist may also increase the family physician’s confidence in his or her professional assessment of the situation.
Many occupational health centers employ multidisciplinary teams that include industrial hygienists, nurses and social workers. This structure allows occupational illness to be addressed comprehensively. In addition, resources are available to conduct workplace evaluations, to provide educational programs and to help patients access appropriate benefits systems and cope with the emotional ramifications of an occupational disease.
Types of the preventive sanitary inspection
The preventive sanitary inspection includes:
1) Working out of the sanitary legislation basis and it s scientific background:
– participation in the working out of the State Standards of Ukraine (SSU), for different manufactures and products, particularly for water, production of food and light industry;
– participation in the working out of the building norms and rules (BNandR);
– working out the Sanitary rules and norms (SRandN), maximum allowable concentrations (MAC), maximum allowable limits (MAL), maximum allowable doses (MAD), dose limits (DL), minimum residue limits (МRL), oriented safe influence levels (OSIL), technical terms (TT), Norms of radiation safety of Ukraine (NRSU), Systems of industrial safety standards, Systems of „human–machine”, environmental safety etc.
2) The organization and carrying out of the sanitary inspection of different types of projects during all project stages – for settlements, living, educational, public, industrial constructions and also projects of technological lines, conveyers, ventilation systems, design solutions for protection from noise, vibration, heat, electromagnetic, ultraviolet, ionizing radiation and laser emission, chemical and dust pollutants in the air of working area;
– project appraisal of the different lathers, mechanisms, machines, vehicles;
– expert evaluation of the projects of the sanitary and technical, ergonometrical equipment of interiors of the different types of premises (residential, educational, hospital, industrial, workplaces, vehicle cabins, other objects, mechanism control means etc.).
The organization and project documentation appraisal is carried out according to the norms, regulations, instructions, state standards listed above and other official documents.
At first the type and level of the industrial environment influence on the working and living conditions of workers – basic materials, manufactured products, by–products, wastes, gas– and vapor wastes, sewage, solid wastes, the air, water reservoirs, soil polluted by them, assessment of methods and instruments of waste processing must be assessed during analysis of the technology of the projected industrial manufacture. Also the sizes of the sanitary protection zones have to be determined.
During this procedure following data have to be known:
– the site development choice act for the construction;
– construction passport, data on the existing buildings nearby, ground constructions, underground communications, their capacity;
– geological and hydrological data of the site;
– technical terms for connection to present communications, water, power, gas supply, or creation of the new, more powerful communications;
– data on the water reservoirs, soil condition, sources of atmospheric air pollution.
Basics of the constructional and technical drawings
Positive quality of the constructional and technical drawings is their clearness, instant perception, detailed image of separate elements, internationality – independence on the language. Only the explication (explanation to the drawings) and explanatory notes are not international and need corresponding translation if they are written in another language.
Tree types of projections are used in the constructional drawings:
1) Central projection demonstrates usual, visual image of the object: lines that represent the object picture get narrower when going “deeper”.
2) Axonometric, also known as parallel oblique projection (technical sketch) on which all lines picturing the object are parallel and do not narrow in depth.
3) Orthogonal, also known as parallel rectangular projection is used for imaging separate details of the project – facades, plans, slits. Their combination by the axis lines is called ЕПЮР (EPUR).
The uniformed modular system (UMS), marking out the separate elements of the buildings according to their size and including the corresponding scale is used for constructional drawings.
Types of constructional and technical drawings
1. Topographic – situational layouts – are the copies of an increased scale of the topographic maps on which the site development of the projected object, all existing objects around the area and landscape elements (forests, shrubberies, water pools, hills, marshes etc.) are drawn. The downhill gradient is pictured with contour lines. Contour lines are the lines connecting the points of the same height above sea-level. The hill tops are marked with the numbers in meters. The downhill direction is marked with bergstriches.
2. Engineering and construction drawings are the images of the ground (bridges, hollows, cuts, trestles, roads) and underground buildings (pipelines, cables, tunnels etc.) – on the situation and general layouts.
3. Architectural and building drawings are the images of different purpose buildings – living, educational, public, industrial.
4. Industrial drawings picture the technological lines, conveyers, machines, lathers.
5. The drawing of the electrical schemes, radio schemes, electronic schemes, etc.
Basics of the preventive sanitary inspection
The main purpose of the preventive sanitary inspection is the control of the observance of the current state sanitary regulations and rules during each stage of the project creation and the construction process.
The first stage of the project consists of the evaluation of the project task and its technical background. The role of the medical service at this stage is the ecological and sanitary-hygienic assessment of the certain construction plan in a sense of the hygienic characteristics of the existing objects in the area and objects in project (their positive and negative influence on each other).
The second stage of the project consists in:
– the sanitary examination of project materials: draft design (images of the site and constructions in axonometric, oblique views (projections) or their general view);
– the examination of the general layout or the plan of site development;
– the architectural and construction project examination (facades and slits of the buildings with explications and explanatory notes or textual part of the project, drawings of sanitation facility elements – ventilation, cold and hot water-supply and sewerage, electricity and gas supply, low current electrical communications);
– technical and construction drawings by which the construction is performed.
The third stage of the project consists in the transposition of the individual or typical project to the certain land area: participation in the land allocation and evaluation commission, situational layout expertise. The situational layout is a zoomed copy of the topographical map with the image of the site development and surrounding existing objects.
The forth stage of the project consists in sanitary inspection during the construction progress, control of the observance of all the elements of the approved project. If it is necessary to correct the project (for economical, technical or other reasons) these corrections have to be agreed with sanitary inspection.
The fifth stage of the project consists in participation in the commission, responsible for the launch (putting) of the object into operation, making of the technical, sanitary passports of the object.
For this purpose the commission observes the completed object, points out the necessary finishing work or the construction flaws to be corrected. The state commission allows the object’s launch into operation after all the discovered flaws are removed. The act of the object launch is then generated and signed by all the members of the commission including the sanitary doctor.
Types of the preventive sanitary inspection
The preventive sanitary inspection includes:
3) Working out of the sanitary legislation basis and it s scientific background:
– participation in the working out of the State Standards of Ukraine (SSU), for different manufactures and products, particularly for water, production of food and light industry;
– participation in the working out of the building norms and rules (BNandR);
– working out the Sanitary rules and norms (SRandN), maximum allowable concentrations (MAC), maximum allowable limits (MAL), maximum allowable doses (MAD), dose limits (DL), minimum residue limits (МRL), oriented safe influence levels (OSIL), technical terms (TT), Norms of radiation safety of Ukraine (NRSU), Systems of industrial safety standards, Systems of „human–machine”, environmental safety etc.
4) The organization and carrying out of the sanitary inspection of different types of projects during all project stages – for settlements, living, educational, public, industrial constructions and also projects of technological lines, conveyers, ventilation systems, design solutions for protection from noise, vibration, heat, electromagnetic, ultraviolet, ionizing radiation and laser emission, chemical and dust pollutants in the air of working area;
– project appraisal of the different lathers, mechanisms, machines, vehicles;
– expert evaluation of the projects of the sanitary and technical, ergonometrical equipment of interiors of the different types of premises (residential, educational, hospital, industrial, workplaces, vehicle cabins, other objects, mechanism control means etc.).
The organization and project documentation appraisal is carried out according to the norms, regulations, instructions, state standards listed above and other official documents.
At first the type and level of the industrial environment influence on the working and living conditions of workers – basic materials, manufactured products, by–products, wastes, gas– and vapor wastes, sewage, solid wastes, the air, water reservoirs, soil polluted by them, assessment of methods and instruments of waste processing must be assessed during analysis of the technology of the projected industrial manufacture. Also the sizes of the sanitary protection zones have to be determined.
During this procedure following data have to be known:
– the site development choice act for the construction;
– construction passport, data on the existing buildings nearby, ground constructions, underground communications, their capacity;
– geological and hydrological data of the site;
– technical terms for connection to present communications, water, power, gas supply, or creation of the new, more powerful communications;
– data on the water reservoirs, soil condition, sources of atmospheric air pollution.
Basics of the constructional and technical drawings
Positive quality of the constructional and technical drawings is their clearness, instant perception, detailed image of separate elements, internationality – independence on the language. Only the explication (explanation to the drawings) and explanatory notes are not international and need corresponding translation if they are written in another language.
Tree types of projections are used in the constructional drawings:
1) Central projection demonstrates usual, visual image of the object: lines that represent the object picture get narrower when going “deeper”.
2) Axonometric, also known as parallel oblique projection (technical sketch) on which all lines picturing the object are parallel and do not narrow in depth.
3) Orthogonal, also known as parallel rectangular projection is used for imaging separate details of the project – facades, plans, slits. Their combination by the axis lines is called ЕПЮР (EPUR).
The uniformed modular system (UMS), marking out the separate elements of the buildings according to their size and including the corresponding scale is used for constructional drawings.
Types of constructional and technical drawings
1. Topographic – situational layouts – are the copies of an increased scale of the topographic maps on which the site development of the projected object, all existing objects around the area and landscape elements (forests, shrubberies, water pools, hills, marshes etc.) are drawn. The downhill gradient is pictured with contour lines. Contour lines are the lines connecting the points of the same height above sea-level. The hill tops are marked with the numbers in meters. The downhill direction is marked with bergstriches.
2. Engineering and construction drawings are the images of the ground (bridges, hollows, cuts, trestles, roads) and underground buildings (pipelines, cables, tunnels etc.) – on the situation and general layouts.
3. Architectural and building drawings are the images of different purpose buildings – living, educational, public, industrial.
4. Industrial drawings picture the technological lines, conveyers, machines, lathers.
5. The drawing of the electrical schemes, radio schemes, electronic schemes, etc.
Basics of the preventive sanitary inspection
The main purpose of the preventive sanitary inspection is the control of the observance of the current state sanitary regulations and rules during each stage of the project creation and the construction process.
The first stage of the project consists of the evaluation of the project task and its technical background. The role of the medical service at this stage is the ecological and sanitary-hygienic assessment of the certain construction plan in a sense of the hygienic characteristics of the existing objects in the area and objects in project (their positive and negative influence on each other).
The second stage of the project consists in:
– the sanitary examination of project materials: draft design (images of the site and constructions in axonometric, oblique views (projections) or their general view);
– the examination of the general layout or the plan of site development;
– the architectural and construction project examination (facades and slits of the buildings with explications and explanatory notes or textual part of the project, drawings of sanitation facility elements – ventilation, cold and hot water-supply and sewerage, electricity and gas supply, low current electrical communications);
– technical and construction drawings by which the construction is performed.
The third stage of the project consists in the transposition of the individual or typical project to the certain land area: participation in the land allocation and evaluation commission, situational layout expertise. The situational layout is a zoomed copy of the topographical map with the image of the site development and surrounding existing objects.
The forth stage of the project consists in sanitary inspection during the construction progress, control of the observance of all the elements of the approved project. If it is necessary to correct the project (for economical, technical or other reasons) these corrections have to be agreed with sanitary inspection.
The fifth stage of the project consists in participation in the commission, responsible for the launch (putting) of the object into operation, making of the technical, sanitary passports of the object.
For this purpose the commission observes the completed object, points out the necessary finishing work or the construction flaws to be corrected. The state commission allows the object’s launch into operation after all the discovered flaws are removed. The act of the object launch is then generated and signed by all the members of the commission including the sanitary doctor.
Aims, tasks and legal basics of the regular sanitary inspection
Regular sanitary inspection is the series of measures for the control of compliance to hygienic regulations, sanitary rules and instruction documents during the object exploitation.
The aim of the regular sanitary inspection is the creation of favourable conditions for life, labour, rest, treatment; the prevention of hazardous environmental influence or working conditions on human health and hazardous influence of adverse conditions of the object on the collective health and the environment.
The legal basics of the regular sanitary inspection are the legislative instructions and methodic materials: State standards, building and sanitary norms and rules (BNandR, SNandR), maximum allowable levels, concentrations, doses (MAL, MAC, MAD) and others, and also the legal documents as a basis for the disciplinary, administrative, penalty sanctions in case of the significant sanitary regulation breaches. These documents include the following:
– Instruction “The order of the application of the fines for the sanitary legislation breaches”. The decree of Ministry of public health of Ukraine № 64 from 1994;
– Instruction “On the order of … the ban of the personnel from work or other activity (in case of significant breaches of the sanitary legislation)”. The decree of Ministry of public health of Ukraine № 66 from 1995;
– Instruction “The order of the State sanitary-and-epidemiological service administrative or preventive sanctions application: limitation, temporary ban, ban, interruption or cancellation of the object exploitation”. The decree of Ministry of public health of Ukraine № 67 from 1995;
– The order of the application of the financial sanctions for breaches of the sanitary legislation. The decree of Ministry of public health of Ukraine № 135 from 1995 and others.
Legislative documents on criminal charge for rude breaches of the sanitary legislation – ecological or socially hazardous also exist.
The types of the regular sanitary inspection
1. The deep sanitary inspection of the object is carried out if:
– the object is being launched into exploitation after the construction or reconstruction. In this case, the aim is to generate the detailed description of the object, and its sanitary passport;
– the urgent sanitary inspection is required, or in case of incidents during and after the elimination of their consequences.
2. The periodic sanitary inspection of the object during the exploitation is carried out to control of the compliance to the sanitary standards and rules and to the requirements and recommendations of previous inspections. These inspections may be:
– routine, which are conducted in the fixed monthly, quarter, semi-annual and other periods;
– sporadic (raid) or non–routine inspections, which allow to check for the breaches of the sanitary procedure during the object exploitation without warning;
– unplanned, urgent or emergency sanitary inspections are conducted on request of the object employees (for example, manufacture workers) or population, or in case of the infectious disease outbreaks, nutritional or occupational poisonings, accidents and others.
Methods which are used for the object sanitary inspection
1. The analysis of the technical documentation (the object technical passport, production technology and others), sanitary documentation (the sanitary passport, sanitary journals, personal sanitary books of the nutrition, commercial, educational or medical institutions employees).
2. The visual inspection of the object, personnel, object exploitation elements, the usage of the organoleptic research methods.
3. The usage of the express laboratory for the research of the physical hazards (noise, vibration, lighting, electromagnetic waves of different frequency, microclimate parameters), the dust and other environmental factors as a method of the assessment of the object exploitation conditions.
4. The usage of the sampling, express or laboratory research of the chemical, bacteriological and others biological hazards which may also be used in the assessment of the object sanitary conditions.
5. The usage of the calculation methods of the qualitative and quantitative assessment of certain object characteristics according to the appropriate formulas and nomograms (for example: calculation of the parameters of protection from ionizing radiation, density of the ultrahigh and other frequencies electromagnetic fields).
6. The final aim of the regular sanitary inspection is the compilation of the object sanitary description during the deep sanitary inspection, and also its sanitary passport or sanitary inspection act during the regular, planned, periodical, raid or urgent sanitary inspections.
The special cards for the inspected object, designed for each object type, are used to make the document generation process easier. These schemes can be found in appendices to practical part of the lesson, their examples – in appendices 2 and 3.
The final point of the object sanitary description or inspection act should contain the recommendations or instructions for the sanitary regulation breaches removal, preventive, health-improving measures and the terms of their conduction. The appropriate legal sanctions, including the object closure and other legal measures are applied in case of the significant sanitary rule breaches that may be dangerous for the personnel or environment.
The object sanitary inspection card
1. Study the official legislative and normative documents that regulate the requirements to projection, building, exploitation of the objects of certain type and purpose (hospital, school, hostage, manufacture, certain department and so on).
2. Work out the map (plan) of the sanitary inspection, that widely covers such questions as:
2.1. Passport data (name of the object, its address, who is responsible for exploiting the object, the time of its construction or reconstruction etc.).
2.2. The characteristics of the object location, its surrounding area (sizes, site configuration, relief, ground (soil) and hydrological conditions of the built–up area, percentage of the built–up and green area, communications, sanitary-hygienic zone adequacy, the outside objects which may be the air, soil, water pollutants or noise sources, microwave radiation).
2.3. The construction and planning characteristics (particularities) of the object (type of the building, presence of the built–in objects, the main building structure characteristics, main functional premises planning and sizes, their orientation and compliance to requirements).
2.4. The sanitary improvement of the object (water–supply system, hot–water supply, sewerage and other systems for liquid waste collection and disposal, heating, ventilation, natural and artificial lighting, solid waste disposal system and etc.).
2.5. The compliance of the sanitary equipment to requirements and main technical and sanitary standards.
2.6. The compliance of the object exploitation and its equipment to requirements (the optimal technological process usage, the usage of allowable reagents, departmental and state sanitary inspection periods and regularity, compliance of the technical, sanitary equipment, sales of production etc. to the usage terms).
2.7. The sanitary condition of the premises and object equipment (organization and regularity of the tidying, the usage of the general and individual prophylactic measures, compliance of the ventilating, refrigerating, lighting and other systems to the hygienic requirements).
2.8. The influence of living, educational or labor conditions at the object on the human health and sanitary conditions of life (pollution levels of certain biosphere objects, typical complaints of the object residents or employees, cases of diseases, that may be caused by the certain object etc.).
2.9. The individual determination of the object condition and sanitary state, or usage of the laboratory data for that (noise, lighting, electromagnetic waves, air, water, food products bacteriological pollutions etc.).
2.10.The listing and assessment of the object features or the environment parameters that do not comply to the hygienic standards.
2.11.The description of the background of the measures for the object sanitary condition improvement, reconstruction recommendations etc.
2.12.The sanitary inspection results should be formally summarized as the object sanitary description (its sanitary passport elaboration) or the sanitary regulation breach act with appropriate sanctions (fines, object closure, the correction term schedule etc.) listed.
Appendix 3
THE APARTMENT SANITARY INSPECTION CARD
1. Address: str. ________________________, building № ________, app. № ______. Householder last name __________________________________________.
2. Floor _______, number of rooms _______, rooms facing the street ______, rooms facing the backyard _______, darkening by the nearby buildings (yes, no) __________, room orientation (by compass)______________, open spaces in the apartment _____________.
3. Total area of the apartment ___________ m2, height _________ m.
4. Number of residents ___________, of them children ______________.
5. Living area per 1 person _________ m2, the air cube ____________ m3.
6. Exterior walls ___________________, decoration of inside walls _________, floor _______________, windows _________________, doors _____________.
7. Heating: central, local, hot–water, stream (sufficient, insufficient); the air temperature _______________.
8. Ventilation: natural (wickets, transoms presence, end–to–end aeration – possible or not); artificial (local, inlet, outlet, operates quietly, or noisily, with vibration); central (inlet, outlet, inlet-outlet, ventilation aperture location) ____________________________________________________________________________________________________________________________________________________________________________________________________________
9. Natural lighting (daylight) (number of windows and their location, glassing type, glass quality), glass dirtiness (mild, moderate, severe), shadowing (present, absent), the lighting with direct solar rays (possible or not)________ ________________________________________________________________________________________________________________________________________
10. Artificial lighting: electrical (incandescent lamps, luminous lamps), lighting system (general, local, combined), type of lights (their number and location, height, lamp power), lighting (equally spread or not; sufficient or not)_________________________________________________________________________________________________________________________________________________________________________________________________________
11. Water-supply (central, local).
12. Sewer system (present or absent), toilet (located in the house, outside, warm, cold, waterproof, absorbent rakings) ________________________ ________________________________________________________________________________________________________________________________________
13. Kitchen – stove (gas, electrical), area ________ m2, cube _______ m3 ____________________________________________________________________
14. Utility room presence (which type) _______________________________________
15. Domestic animals (present, absent, which) ____________________________________________________________________
16. Insects present indoor (present, absent, which) ___________________________________________________________________, rats, mice (present, absent) ______________________________________________
17. High humidity in the rooms (present, absent, cause) ________________________________________________________________________________________________________________________________________
18. Noise, vibrations (yes, no, cause) _________________________ ________________________________________________________________________________________________________________________________________
19. Resident’s complaints _______________________________________________ ________________________________________________________________________________________________________________________________________
20. Additional data: ____________________________________________________ ____________________________________________________________________________________________________________________________________________________________________________________________________________
Summary of the object sanitary state.
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Recommendations __________________________________________________________________________________________________________________________________________________________________________________________________________________
Date of inspection Signature
“____”______________ 200_ _____________________
Example of the sanitary passport of the object
MINISTRY OF PUBLIC HEALTH OF UKRAINE
KIEV municipal sanitary-and-epidemiological station
radiological department
8/10, Necrasovska str. phone: 216-60-20
Estonska str. phone: 442-50-46
Kyiv-53, 252053
SANITARY PASSPORT
Allows to work
with IONIZING RADIATION SOURCES (IRS)
Кyiv – 2012
1. Institution: Research institution of the ear, throat, nose. 5, Zoologichna str, Kyiv-57; phone 441-49-97.
2. Authority: Ministry of public health of Ukraine. 7, Hrushevskogo str, Kyiv.
3. Supervisor: Academy of medical science of Ukraine.
4. Department of institution receiving the passport: Radiological department.
5. Person (with position), responsible for the radiological safety at the object: Pokotilenko Alexander Gavrilovich, PhD, decree № 120/3 from 5.02.1996. Phone 441-49-42.
6. Types of allowed operations with the ionizing radiation sources (IRS):
|
№ |
Type and kind of IRS |
Type and kind of operations |
Operations site |
Limitation |
|
1. |
Operations with open IRS І131, Тch132, Р32, S35. |
Radioisotopic diagnostics |
Radioisotopic laboratory |
Indicated doses usage /tо 10 μCurie on І131. |
|
2. |
Operations with close IRS Сs137, С060. |
Cancer treatment with (using) the application method |
Close IRS laboratory |
/to100 μCurie on the operating site |
|
3. |
Gamma-therapy unit ГУТ-С060– 400 mg–eq. redium. |
Cancer distant gamma(ray) teletherapy |
Telegamma-therapy laboratory |
Opening the working tubule only after the patient fixation and from the control desk |
7. Mandatory radiological control:
– personal dosimetry – permanently for all staff;
– exposure dose rate determination – on the operating sites, behind protective screens and walls of the adjacent rooms – periodically;
– radiometric control – in all rooms of the open isotopes department and radioactive waste storages – periodically.
8. The sanitary passport issued basing on:
– the act of the launch of the newly constructed (reconstructed) department building into operation № 17/4 from 6.02.96;
– the passport for the gamma-therapy unit ГУТ-С060 (GUT-С060)– 400 mg–eq. radium;
– “The instruction of operation with IRS” being present and the personnel being familiar with it;
– decree of the research institution’s director on appointment of the person, responsible for the radiological safety.
9. The sanitary passport is valid until 01.01.2010
|
Stamp |
The chief state sanitary doctor (officer) of Kyiv |
(signature) |
|
|
|
|
|
Date of the sanitary passport issue 6.02.97 |
|
|
|
|
|
|
|
Performed by the head of the radiological department of the Kyiv municipal SES (SEI) sanitary doctor |
(signature) |
|
|
|
|
|
|
This document exists in 3 copies, that have been given to: 1 – the institution – head of the radiological department of the research institution of ear, throat, nose 2 – the central radiological directorate of the Ministry of public health of Ukraine 3 – the radiological department of the Kyiv municipal SES (SEI) |
(signature)
(signature)
(signature) |
|

